
Abstract
Background:
Among intensive care unit (ICU) patients, thrombocytopenia is a common abnormality, having a prevalence of about 50%. This thrombocytopenia may lead to an increased risk of bleeding, impaired wound healing and organ haemorrhage in severe cases. Relative thrombocytopenia serves as a sign of heightened risk. Hence, addressing the thrombocytopenia early and regular monitoring helps in better management of sepsis patients.
Methods:
This prospective study analysed 115 patients diagnosed with sepsis and septic shock from April 2023 to December 2024 in a tertiary care hospital. Data collected includes demographic factors and clinical parameters (CBC, SOFA score, ICU stay duration, outcome and 28-day mortality).
Results:
Among 115 patients, 36.52% had thrombocytopenia. The 28-day mortality of sepsis patients with thrombocytopenia was 23.18% (P < .001). Major bleeding episodes occurred in 40% patients with thrombocytopenia (P = .034) and they also required transfusions of packed whole blood (73% P < .001), fresh frozen plasma (FFP) (67% P < .001), cryoprecipitate (26% P = .005) and platelets (45% P < .001). The 28-day mortality was lower among thrombocytopenic patients whose thrombocytopenia resolved compared with those in whom it did not resolve (40% vs. 60%, P < .0001).
Conclusion:
Sepsis patients developing thrombocytopenia face significantly worser outcome, especially in those whose platelet count did not resolve during the course, faces more risk of mortality. They also had the increased risk of major bleeding episodes and the need for multiple transfusions. These findings emphasize the need for routine monitoring of platelet counts in the sepsis patients.
Introduction
Sepsis is defined as an organ dysfunction due to an imbalanced/dysregulated response of the host to systemic infection.[1,2] According to the Sepsis-3 definition, the essential criteria are the presence of organ dysfunction. The systemic involvement ranges from neurological, endocrine, cardiovascular and other systems. The presence of organ dysfunction is calculated by an acute change in total SOFA score of 2 or more points as a consequence of systemic infection.[3]
Globally, sepsis affects an estimated 48.9 million people annually, accounting for nearly 11 million deaths or 20% of all global deaths. Southeast Asia and India report high incidences, with factors such as limited healthcare access, under-reporting and a high prevalence of infectious diseases contributing to the burden.[4,5]
Worldwide, the mortality rate for sepsis varies but often ranges from 20% to 30%. Septic shock is one of the common complications of sepsis that is caused by severe disease progression. The clinical manifestations observed include persistent hypotension and a need for vasopressor therapy to maintain the MAP of ≥65 mmHg and a lactate level >2 mmol/L in addition to adequate fluid resuscitation.[6,7]
Sepsis can lead to various complications, the most common being disseminated intravascular coagulation. Organ failure, especially of the kidneys, liver or lungs are also common. Other complications of sepsis include thrombocytopenia, increased risk of secondary infections and latent immune suppression. There are residual and long-lasting cognitive and physical impairments in patients who survive sepsis.[8]
Among intensive care unit (ICU) patients, thrombocytopenia is a common abnormality, with a prevalence of about 50%.
Thrombocytopenia is defined as a low platelet count. The count may be as low as 150,000 cells/μL. It is classified as mild, moderate or severe based on platelet levels. Platelet counts less than 50,000 increase the bleeding risk.[9]
This thrombocytopenia may lead to an increased risk of bleeding, impaired wound healing and organ haemorrhage in severe cases.[10]
This usually results from several etiological factors. Reduced platelet production (e.g., bone marrow disorders), increased peripheral destruction (e.g., autoimmune illnesses, infections) and splenic sequestration of platelets may lead to this condition.[11]
Thrombocytopenia in sepsis is often caused by disseminated intravascular coagulation (DIC), immune-mediated destruction of platelets or reduced production of platelets from bone marrow.
Several mechanisms contribute to sepsis-associated thrombocytopenia, although the exact aetiology is unknown. These include activation of platelets due to vascular injury, suppression of marrow and platelet-targeted antibodies. Several articles emphasise that thrombocytopenia in sepsis correlates with increased severity of illness and mortality. Emerging biomarkers such as PF4 and soluble P-selectin have been investigated to understand this relationship better. Yet the causation and association remain uncertain and unexplored.
With this background in mind, this study was done to estimate the incidence of thrombocytopenia in sepsis patients in an ICU setup and to analyse various factors influencing them.
Materials and Methods
A prospective observational study was conducted among patients admitted to the ICU of Apollo Hospital, a tertiary care centre in South India, from April 2023 to December 2024. The institutional review board approved this study. Informed consent was obtained from the patients. Privacy and patient confidentiality were maintained as per norms. The inclusion criteria of the study comprised adult patients (age > 18 years) who were diagnosed with sepsis or septic shock and hospitalised to the medical ICU. The exclusion criteria of the study are chemotherapy usage in the last 30 days before admission, haematological malignancies (e.g., acute myeloid leukaemia), a history of platelet disorders and patients who refused written consent.
Methodology: Patients in the ICU setup of Apollo Hospitals presenting with sepsis were provided with an information sheet about the study and those who were willing to participate were given an informed consent form in the local language (Tamil). Detailed medical history, physical examination, complete blood counts and biochemistry panel were determined in all patients within 24 hours of admission or onset of sepsis or septic shock. We measured platelet counts in serial intervals to determine the thrombocytopenia in sepsis patients. We followed the patients for 28 days to determine the mortality rate.
Statistical Study Plan:
The sample size was calculated based on the following formula
N = z2pq/d2
Z = standard normal variant = 1.96
Prevalence − 51.1%
d = clinical allowable error = 10%
P = .511
q = 1 − P = .489
n = (1.96 )2 × (0.511*0.489)/(0.1)2 = 96
with considering 20% non-response rate = 96 + 19 = 115
The sample size was 115. The data was collected in Microsoft Excel using a structured questionnaire. The descriptive statistics were presented with percentages for categorical data and mean ± SD for continuous data. The median with interquartile range was presented for the skewed data. The chi-square test or Fisher’s exact test determined the association between clinical profile and demographic factors. The data was analysed using the software SPSS.
Results
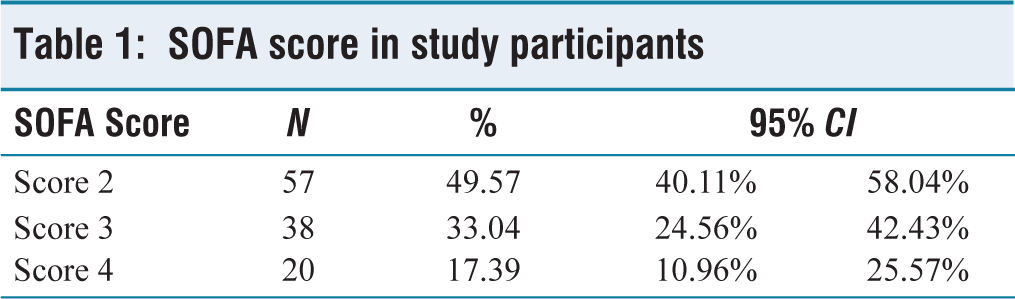
The study included 115 participants. The mean age of the patients in our study was 58 years, with a range from 22 to 88 years. Gender distribution showed that the majority were males, comprising 52.17% (95% confidence interval (CI ): 42.66%–61.57%). Females accounted for 47.83% (95% CI: 38.43%–57.34%) of study participants. Of the 115 sepsis patients, 17.39% had no comorbidities. Hypertension was present in 14.78% (95% CI: 8.85%–22.61%) and diabetes in 13.91% (95% CI: 8.17%–21.61%). Patients with both hypertension and diabetes constituted 24.35%, while 29.57% had other comorbidities, showing the highest proportion among the groups. The major source of infection is pneumonia (35%), followed by UTI (22%), skin and soft tissue infections (15%) and systemic and bloodstream infections (9%). Unknown sources are observed in nine patients (8%) and all other sources contribute 12% of overall cases. The severity of illness based on SOFA scores showed that 49.57% patients had a score of 2, 33% of patients had a score of 3 and 17% patients had a score of 4, [Table 1].
SOFA score in study participants
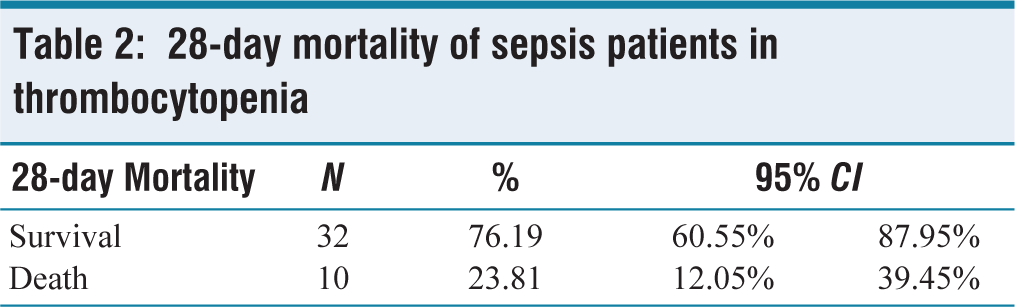
According to the mortality results, 82.61% of patients survived for over 28 days, while 17.39% (95% CI: 10.96%–25.57%) did not. Thrombocytopenia was observed in 36.52% of patients (95% CI: 27.74%–46.01%), while 63.48% (95% CI: 53.99%–72.26%) did not [Figure 1]. Out of the total cases, 76.19% (n = 32) survived, with a 95% CI ranging from 60.55% to 87.95%. However, 23.81% (n = 10) died within the 28 days, with a CI of 12.05%–39.45% [Table 2].
28-day mortality of sepsis patients in thrombocytopenia
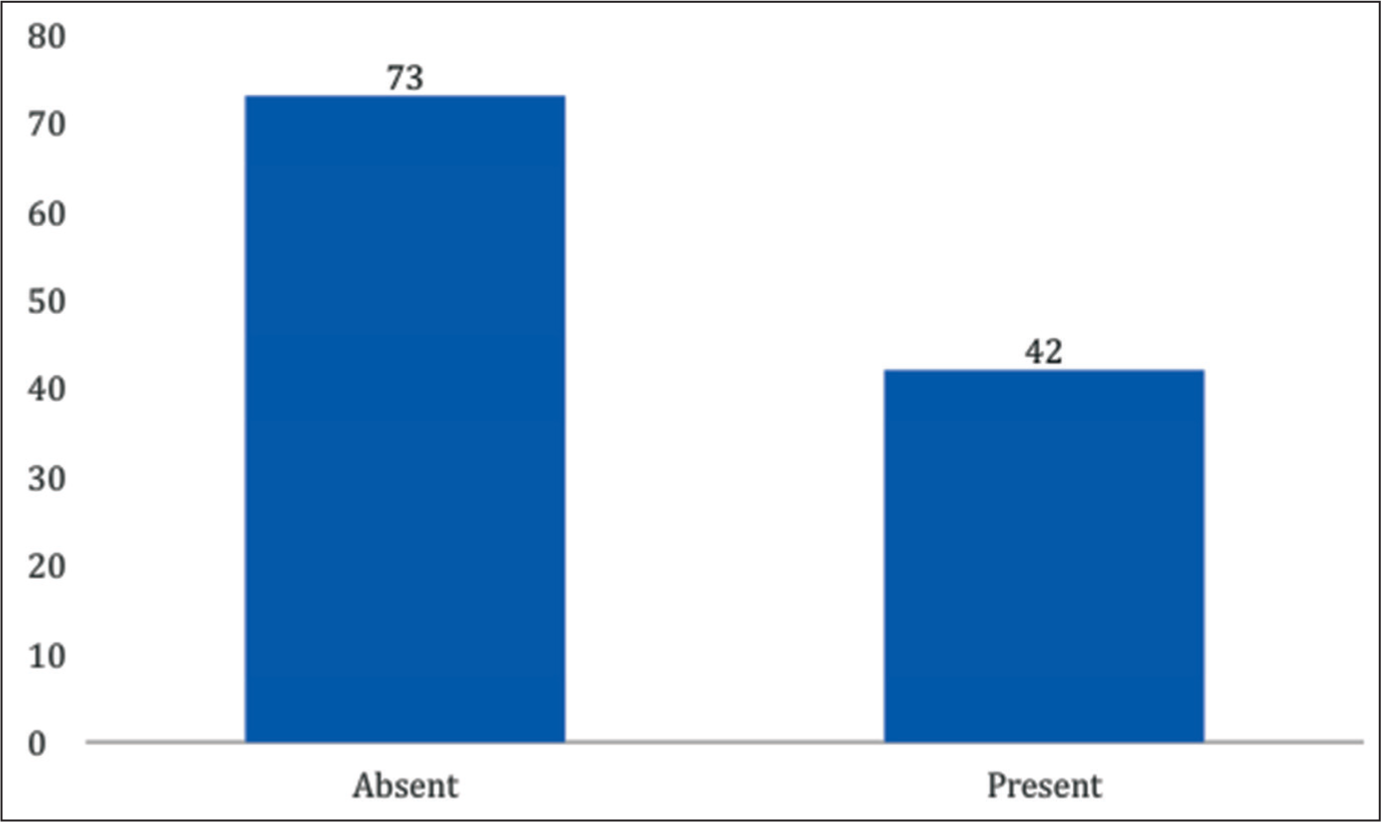
Bar chart depicting the incidence of thrombocytopenia in sepsis patients
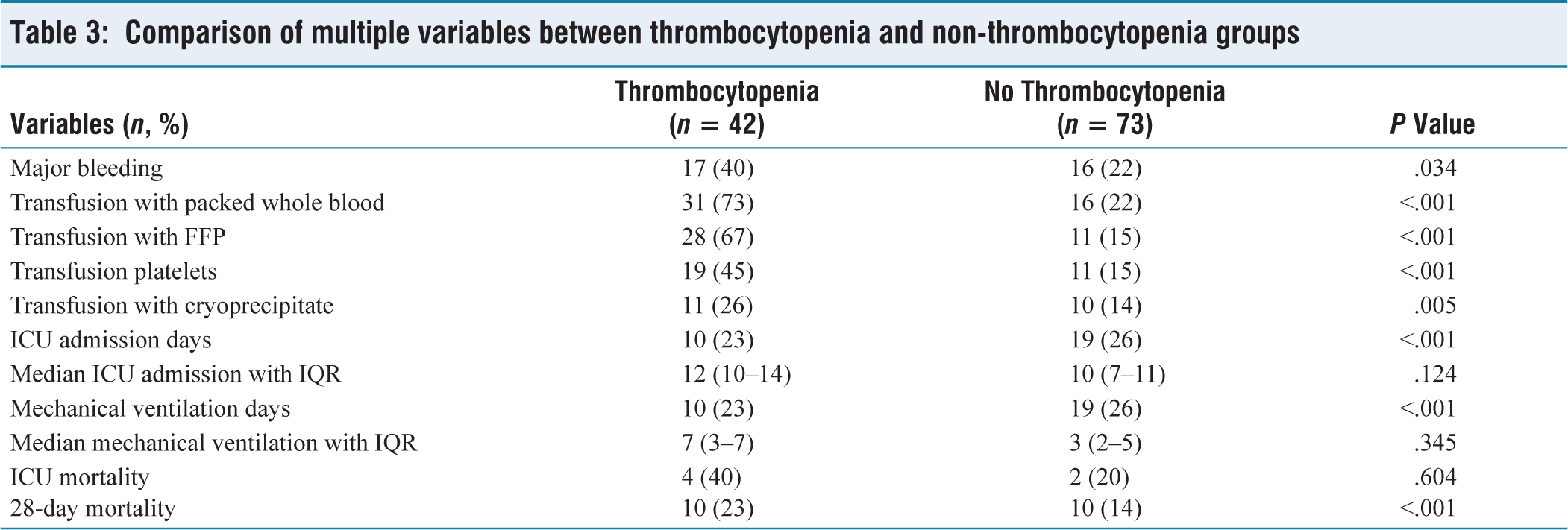
Patients with thrombocytopenia showed major bleeding episodes (40% vs. 22%, P = .034) compared with those without thrombocytopenia (22%). The transfusion requirements for packed whole blood (73% vs. 22%, P < .001), fresh frozen plasma (FFP) (67% vs. 15%, P < .001), cryoprecipitate (cryo) (26% vs. 14%, P = .005) and platelets (45% vs. 15%, P < .001) all showed significant when compared with patients without thrombocytopenia [Table 3]. ICU mortality among thrombocytopenic patients was 40% compared to 20% in those without thrombocytopenia (P = .604), while 28-day mortality was 23% versus 14% (P < .001). The ICU mortality rate for thrombocytopenic patients in those patients whose thrombocytopenia resolved was 0% and for those whose condition persisted was 40% (P < .0001) [Table 4]. The 28-day death rate for resolved cases was lower (40%) compared to unresolved cases (60%, P < .0001) and hospital mortality rates were 30% versus 60% (P < .005) [Table 5].
Comparison of multiple variables between thrombocytopenia and non-thrombocytopenia groups
Showing the mortality in sepsis patients with thrombocytopenia, resolved/unresolved

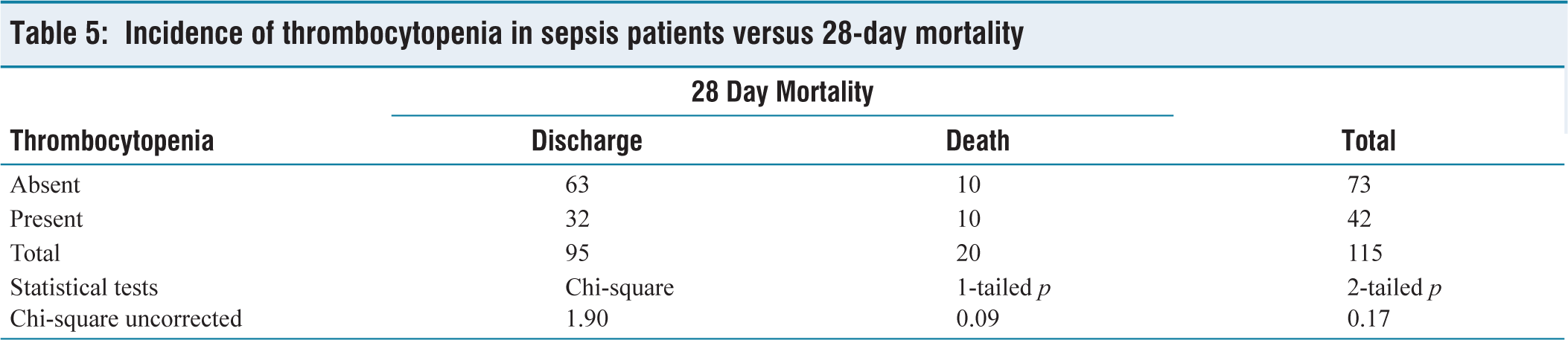
Incidence of thrombocytopenia in sepsis patients versus 28-day mortality
Among patients, 14.29% (n = 6) experienced no bleeding episodes, with a 95% CI of 5.43% to 28.54%. About 26.19% (n = 11) reported one to two bleeding episodes (95% CI: 13.86%–42.04%). The majority of cases, 38.10% (n = 16), had three to four episodes of bleeding, with a CI of 23.57%–54.36%. Last, 21.43% (n = 9) experienced more than four bleeding episodes, with a CI of 10.30%–36.81%.
Out of 73 patients without thrombocytopenia, 10 died, whereas among the 42 with thrombocytopenia, 10 also died. This indicates a higher mortality proportion in the thrombocytopenia-present group. However, the chi-square value of 1.90 and the P value of .17 suggest that thrombocytopenia and 28-day mortality had no statistical significance.
Discussion
The mean age of the participants in our study was 58 years (range: 22–88 years). Patients aged 51–60 years formed the largest group (31.30%), followed by those aged 61–70 years (23.48%). Similar findings have been observed in other studies focusing on sepsis patients, where middle-aged and older individuals are predominant due to reduced immunity and increased comorbid conditions.[12]
Gender distribution: The current study revealed a male predominance, with 52.17% males and 47.83% females. While males were marginally higher, this gender disparity aligns with previously reported findings. Male susceptibility to infections such as sepsis has been attributed to immunological differences and hormone-mediated effects.[13]
Comorbidities in study participants: Comorbid conditions significantly impact sepsis outcomes. In our cohort, 17.39% had no comorbidities. The presence of hypertension (14.78%) and diabetes (13.91%) was comparable to previous studies, indicating that these conditions exacerbate immune dysfunction in sepsis.[14–16] Patients with both hypertension and diabetes constituted 24.35%, whereas 29.57% had other systemic illnesses. The high prevalence of comorbidities reflects a well-established link between chronic illnesses and susceptibility to severe sepsis.[14–16]
SOFA score and sepsis severity: Our results showed that the majority of patients had SOFA scores of 3 (37.39%) and 4 (35.65%), indicating moderate-to-severe organ dysfunction. The SOFA score remains a validated predictor of sepsis severity and mortality, consistent with numerous studies.[17,18]
Twenty-eight-day mortality in study participants: In our study, the total 28-day mortality rate was 17.39%. This rate aligns with global sepsis mortality rates, which range from 15% to 30%, depending on the study population and healthcare setting.[19] The survival rate in our study (82.61%) may reflect early recognition and appropriate management of sepsis, including timely administration of antibiotics and supportive therapy.[20]
Incidence of thrombocytopenia in sepsis patients: Thrombocytopenia was present in 36.52% of patients, which aligns with findings from studies indicating thrombocytopenia as a common haematological abnormality in sepsis. The absence of thrombocytopenia in 63.48% suggests that platelet levels may vary depending on the timing of assessment, the severity of illness and underlying conditions.[21]
Thrombocytopenia and 28-day mortality in sepsis patients: It is observed from the study that the patients with thrombocytopenia had a higher mortality rate (23.81%) compared to those without it. This trend, while not statistically significant (P = .17), aligns with reports that emphasise thrombocytopenia as an indicator of poor outcomes in sepsis [Figure 2].
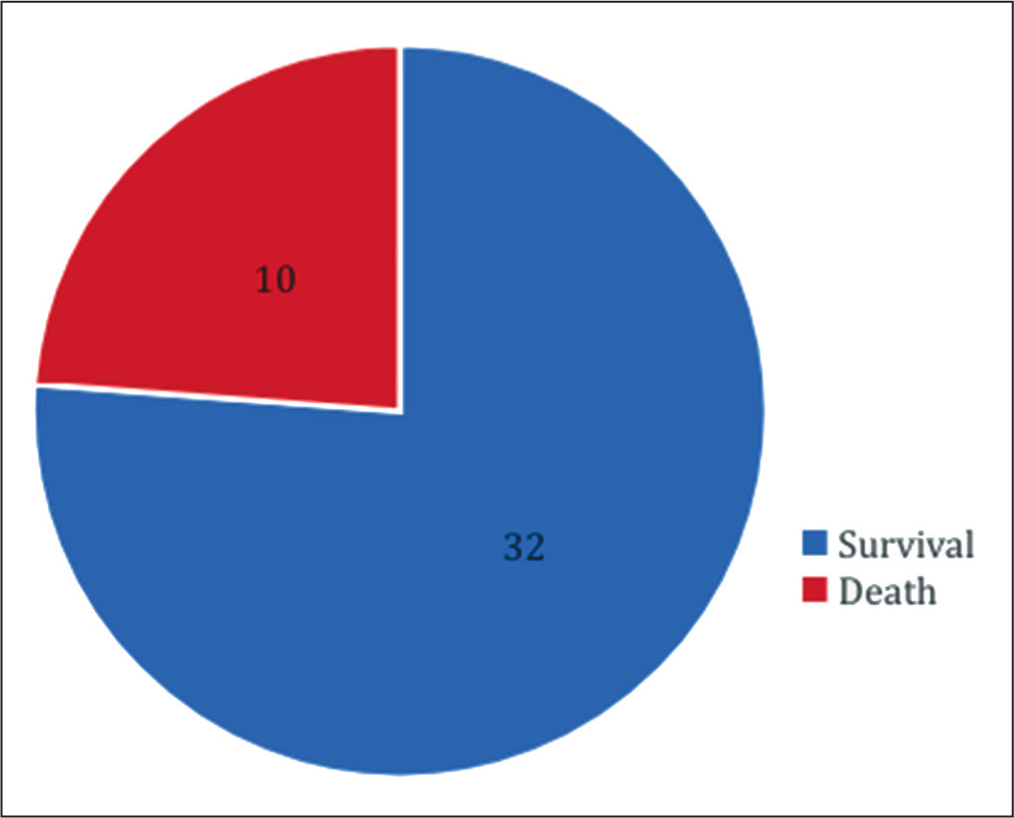
Pie chart depicting 28-day mortality of sepsis patients in thrombocytopenia
Comparison between thrombocytopenia and non-thrombocytopenia groups: In any instance of thrombocytopenia, a significant rise in the necessity for platelet or platelet product transfusions will be evident. As a result, it was linked to higher rates of transfusions involving blood and blood products. Such findings are observed in several studies showing that thrombocytopenic patients often require more aggressive hemostatic support due to a higher propensity for bleeding complications. A study by Stephan et al.[22] demonstrated that thrombocytopenic patients required more blood product transfusions, which may contribute to a pro-inflammatory state and worsen outcomes in sepsis.
The prolonged ICU stay and mechanical ventilation days among patients with thrombocytopenia reflect the severe course of illness in these individuals. Previous studies have similarly reported prolonged ICU duration in thrombocytopenic patients. The median ICU and ventilation days observed in this study further emphasise the resource-intensive care required for these patients.
ICU and 28-day mortality rates were higher among thrombocytopenic patients, particularly those whose thrombocytopenia did not resolve. These findings align with data from Williamson et al.[23]
According to this study, persistent thrombocytopenia is generally an independent predictor of mortality. This was particularly noted in patients with critical illnesses. The thrombocytopenia that has not been corrected suggests the presence of ongoing systemic inflammation. This secondary infection could stem from DIC or bone marrow dysfunction. All these conditions are linked to adverse health outcomes, leading to mortality or morbidity.
Comorbidities and incidence of thrombocytopenia: While thrombocytopenia was most common in patients with other systemic illnesses (41.18%), no significant association was noted between comorbidities and thrombocytopenia (P = .16). This result mirrors existing literature, where conditions such as hypertension and diabetes are known to exacerbate inflammation but may not directly influence platelet counts.[24,25]
Incidence of thrombocytopenia and 28-day mortality in sepsis patients: The mortality rate of patients with thrombocytopenia (10/42) was elevated in comparison to those without it (10/73). The statistical significance was not achieved (P = .17). However, this tendency is cause for alarm. And it highlights thrombocytopenia as a potential risk factor for death. Similar findings are observed in previous studies as well.[26]
SOFA score and incidence of thrombocytopenia: The highest thrombocytopenia incidence was observed in patients with SOFA score 3 (20/43), though the association was not significant (P = .22). Other research suggests that increasing SOFA scores are associated with a reduction in platelet counts, illustrating the cumulative effects of organ dysfunction.[27]
Conclusion
The overall incidence of thrombocytopenia with sepsis in ICU patients was 36.52%, underscoring its frequent occurrence in this group. Thrombocytopenia was associated with higher 28-day mortality (23.81%) compared to patients without thrombocytopenia. But it was not statistically significant (P = .17). Persistent thrombocytopenia was linked to poor health outcomes significantly; the poor outcomes include ICU mortality, hospital mortality and 28-day mortality. Thrombocytopenia was strongly associated with increased bleeding episodes and higher transfusion requirements, emphasising its impact on resource utilisation and complications.
Footnotes
Acknowledgements
The authors acknowledge Dr Venkatachalam, Director of Medical Services; Dr Muralidharan M, Director of Medical Education, and Mr Lokesh, Biostatistician, Apollo Hospitals, Chennai, Tamil Nadu, for their constant support. I sincerely express my gratitude to my guide Dr Soukat Ali and co-guides Dr Prabu P and Dr Vignesh, for their valuable suggestions, support and guidance throughout this endeavour.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
The institutional ethical committee approved the protocol (AMH-DNB-033/03-23).
Informed consent
Informed consent was obtained from all the study participants.
Credit author statement
All authors contributed equally to the manuscript. All authors participated equally in conceptualisation, methodology, supervision, investigation, validation, Literature search, manuscript preparation and manuscript editing. All authors read and approved the final manuscript.
Data availability
The data supporting the findings of this article is not publicly available. Questions about the data can be directed to the corresponding author.
Use of artificial intelligence
No.
Consent for publication
The Institutional Ethics Committees approved the study protocol.