
Abstract
Introduction:
The rising prevalence of obesity poses major challenges in the perioperative management of patients undergoing orthopaedic procedures, particularly proximal femur fracture fixation. Obese individuals frequently present with multiple comorbidities and altered physiology that influence every phase of surgical care. This review aims to identify these challenges and outline practical strategies to optimise perioperative outcomes.
Methods:
A comprehensive literature review was performed using Medline, PubMed, EMBASE, Cochrane Library, and ProQuest databases. Search terms included obese, proximal femur fracture, intertrochanteric fracture, perioperative complications, surgical challenges, and postoperative outcomes. Articles published up to 30 January 2025 were analysed, including discussions on the ‘obesity paradox’ and its clinical implications.
Results:
Preoperative challenges include a higher incidence of obstructive sleep apnoea, pulmonary hypertension, and left ventricular dysfunction. Altered pharmacokinetics necessitate weight-adjusted anaesthetic dosing—benzodiazepines by total body weight and opioids by ideal body weight. Intraoperatively, large panniculus and excessive soft tissue complicate positioning and exposure, requiring specialised tables, taping techniques, and modified instrumentation. Postoperatively, increased risks of wound dehiscence, thromboembolism, delayed mobilisation, and respiratory compromise demand layered closures, early physiotherapy, and CPAP/BiPAP support. Interestingly, the ‘obesity paradox’ suggests that selected obese patients may exhibit favourable survival, warranting individualised care.
Conclusion:
Management of proximal femur fractures in obese patients mandates a multidisciplinary, individualised approach. Optimising comorbidities, meticulous intraoperative planning, and proactive postoperative protocols are key to minimising complications and improving outcomes in this complex population.
Introduction
Life expectancy has plateaued and started to drop in 2015; however, the obesity epidemic peaked in the late 1970s. This decrease in life expectancy is mostly caused due to obesity-related comorbidities of diabetes, heart disease, stroke, and chronic liver disease. As a result, the perioperative requirements for obese surgical patients are expected to rise significantly.[1] Hip fracture cases are on the rise and are a major health concern, with a reported incidence of 2.5 million cases every year in the United States alone. Published studies have concluded that various factors affect the overall prognosis of patients with intertrochanteric fractures, some of them including race/ethnic differences, sex differences, pre-existing medical comorbidities, including dementia, diabetes, congestive heart failure, arrhythmias, renal disease, lung disease, electrolyte imbalance, and hypothyroidism.[2]
Although obesity can cause a variety of adverse complications, in recent years, some researchers have found that obesity may lead to better clinical outcomes for some diseases, which seems to contradict people’s understanding of obesity and is called the ‘obesity paradox’. Although the pathophysiology of the ‘obesity paradox’ is still unclear, it can be hypothesised that fat is the first energy substance consumed after traumatic stress, followed by high energy consumption in obese patients. Therefore, the consumption of fat significantly reduces the consumption of essential proteins, thereby avoiding a decrease in immunity and loss of nutrients in obese patients.[3–5]
This study aims to highlight the challenges and suggest solutions in the preoperative, intraoperative, and postoperative management of proximal femur fractures in obese patients.
Methods
To systematically address the perioperative challenges faced by obese patients undergoing proximal femur procedures, a comprehensive literature search was conducted on 30 January 2025. The search employed several key medical and research databases, including Medline, PubMed, EMBASE, Cochrane Library, and ProQuest.
Utilising specific search criteria, the following key terms were incorporated: ‘preoperative complications in obese patients’, ‘surgical challenges in obese patients’, and ‘intertrochanteric fractures in obese patients’. To ensure a thorough exploration of existing literature, the reference sections of retrieved articles were meticulously reviewed for additional pertinent publications, fostering an exhaustive understanding of the topic.
The search methodology employed Boolean operators—specifically ‘AND’ and ‘OR’—to refine and expand the search results effectively. This approach enabled the identification of studies that were not only relevant but also comprehensive, encompassing various aspects of preoperative, intraoperative, and postoperative challenges associated with obesity and proximal femur fractures.
Only full-text articles available for review were included in this analysis, ensuring that the selected studies provided detailed insights and practical implications. Duplicate publications were carefully filtered out, guaranteeing that the review drew exclusively from unique contributions to the field. As a result, this meticulous and systematic search strategy facilitated the collection of high-quality data, which was essential for addressing the multifaceted challenges in the management of obese patients with proximal femur fractures.
Results and Discussion
The challenges have been divided into three sections for ease of discussion and based on various papers, namely preoperative, intraoperative and postoperative challenges.
Preoperative Challenges
Obstructive Sleep Apnoea (OSA)
Cardiovascular disease, left ventricular failure, and advanced age are all correlated with the severity of OSA.[6] According to the American Society of Anaesthesiologists Task Force on Perioperative Management of Patients with OSA, patients with confirmed or suspected OSA should have a preoperative evaluation done well in advance of surgery so that a perioperative management plan can be prepared and carried out.[7]
A thorough review of medical data, including sleep studies, patient interviews, and physical examinations, should be part of the preoperative evaluation. When OSA is suspected, a targeted interview may cover topics such as morning headaches, apnoea episodes, frequent arousals during sleep, snoring, and daytime somnolence.
The physical exam should include the airway, nasopharyngeal anatomy, neck circumference and tongue volume. As the diagnosis of OSA is associated with a significantly increased incidence of postoperative complications, including respiratory failure, postoperative cardiac events and unplanned intensive care admission, the preoperative preparation for patients with confirmed OSA may include CPAP or BiPAP, preoperative oral appliances and preoperative weight loss. Preoperative initiation and perioperative use of CPAP or BiPAP can reduce postoperative complications such as hypercarbia, hypoxemia and pulmonary artery vasoconstriction.[8–10]
It is recommended to start CPAP in the preoperative duration for severe OSA cases. The evidence is insufficient in regards to cancelling or delaying surgery to further investigate such patients or to perform sleep studies for a definitive OSA diagnosis.[11–13] Due to the increased sensitivity to central and peripheral effects of opioids along with respiratory depressant effects of opioids, these drugs should be used with caution in patients with OSA.[14] Interrupted sleep and nocturnal intermittent hypoxemia may increase pain by activating the inflammatory pathway.[15,16]
Cardiovascular Problems
There are several risk factors for pulmonary hypertension, left ventricular failure, and pulmonary thromboembolism in obese patients. An ECG and an echocardiography to evaluate the shape and function of the ventricles and valves should be part of the preoperative evaluation for individuals with pulmonary hypertension. To maximise the patient’s cardiopulmonary condition, preoperative care should be carried out in collaboration with pulmonary and/or cardiology specialists. A validated method for risk stratification in the bariatric population is the obesity surgery mortality risk score (ORMRS). This method divides groups into low, intermediate, and high risk based on five preoperative variables: BMI, male gender, hypertension, known risk factors for pulmonary embolism (PE), and age ≥45 years.[17]
Metabolic Syndromes (MetS)
Obesity is a significant risk factor for developing MetS, which encompasses a cluster of conditions including hypertension, hyperglycaemia, dyslipidaemia, and abdominal obesity. These MetS only exacerbate the overall health profile of patients but also complicate the perioperative management of obese individuals undergoing proximal femur procedures.
The presence of MetS in obese patients increases susceptibility to cardiovascular complications during surgery. Hypertension is prevalent in this population, leading to elevated risks of cardiac events such as myocardial infarction and stroke. Additionally, obesity-related insulin resistance (IR) frequently results in T2D, which can lead to poor wound healing, increased risk of infection, and prolonged recovery times.[18]
Dyslipidaemia, characterised by abnormal lipid levels, further complicates surgery. Elevated triglycerides and low levels of high-density lipoprotein (HDL) cholesterol are often seen in obese patients, increasing the risk of atherosclerosis and cardiovascular diseases. This not only affects the patient’s overall health status but may also influence the choice of anaesthetic agents and their dosages during surgery.[19]
Moreover, abdominal obesity contributes to an inflammatory state that can lead to chronic low-grade inflammation, affecting the body’s response to surgical stress and complicating postoperative recovery. The interplay between obesity and MetS may also lead to an increased risk of thromboembolism, necessitating vigilant postoperative monitoring and prophylactic measures.[20]
These metabolic complications highlight the importance of preoperative optimisation in obese patients. Effective management of MetS components—such as controlling blood pressure, optimising glycaemic control, and managing lipid levels—can improve surgical outcomes and reduce postoperative complications. The integration of a multidisciplinary approach involving endocrinologists, cardiologists, and anaesthesiologists is essential to ensure comprehensive care for these patients, ultimately leading to enhanced recovery and better outcomes following proximal femur procedures.[21]
Pharmacologic Considerations
Anaesthetic drug-dosing is typically based on patient weight and clinical condition; in obesity, the pharmacokinetic parameters of medications are altered. In obese patients, the amount of adipose tissue increases in proportion to the increase in total body weight, while the amount of lean body weight remains relatively constant, resulting in a reduced proportion of lean body weight per kilogram [Table 1].
Pharmacologic considerations in obese patients [22-24]
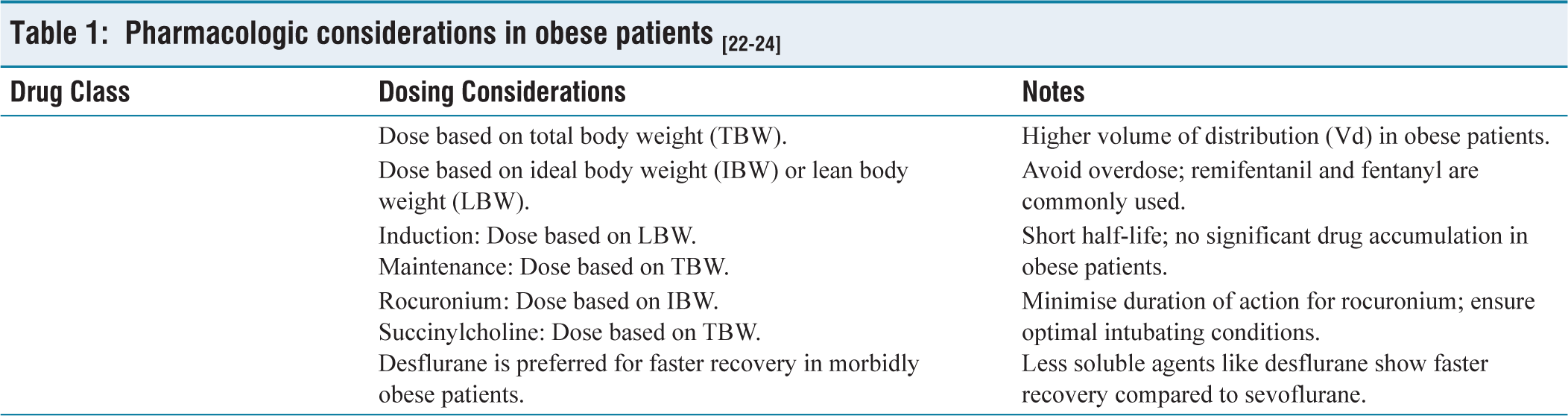
For individual drugs, benzodiazepines, being lipophilic, have a higher volume of distribution in obese patients and should be dosed based on total body weight.[22] Opioids like remifentanil and fentanyl should be dosed based on ideal or lean body weight, not total body weight, to avoid overdose.[23,24] Propofol, with its short half-life, should be dosed based on lean body weight for induction of anaesthesia, but total body weight is appropriate for maintenance without increased drug accumulation.[25–27] Dexmedetomidine, used for sedation, anxiolysis, and pain relief, may result in increased serum concentrations when dosed by total body weight due to a larger volume of distribution and reduced clearance.[28,29] For neuromuscular blockers, rocuronium should be dosed based on ideal body weight, while succinylcholine should be dosed based on total body weight.[30] Regarding volatile anaesthetics, the solubility of inhaled agents influences uptake and recovery, which is affected by increased fat stores in obese patients. Desflurane, a less soluble agent, has shown faster recovery compared to sevoflurane in morbidly obese patients undergoing gastric bypass surgery with epidural analgesia. However, no such difference was observed between sevoflurane and desflurane in studies without epidural analgesia.[31]
Airway Challenges
One of the main causes of anaesthesia-related morbidity and mortality in the obese population is airway management complications. Both difficult mask breathing and difficult laryngoscopy are independently predicted by obesity. Furthermore, OSA and neck circumference are separate indicators of a problematic airway.[32]
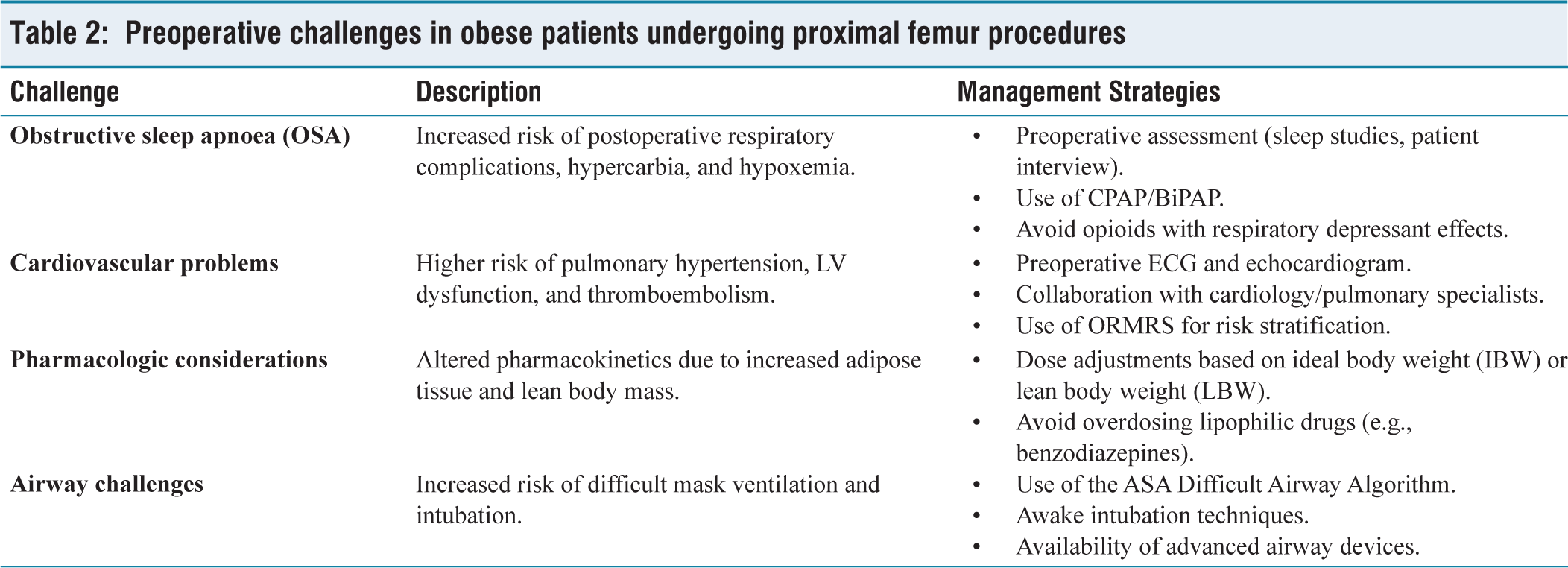
The ASA’s Difficult Airway Algorithm provides a guideline for the management of the difficult airway.[33–36] In the obese population, where difficult mask ventilation and intubation are more likely, the ASA’s Difficult Airway Algorithm suggests the use of techniques such as awake induction, recruitment of additional personnel, as well as the immediate availability of additional advanced airway devices, including tracheotomy equipment.[37] Standard operating room tables have a safe weight capacity of approximately 450 lbs. Specific operating tables designed to hold up to 1,000 lbs should be allocated as needed to prevent patient falls and ensure intraoperative safety. Nerve injury is a known complication related to surgery and patient positioning. Studies have demonstrated an increased risk of nerve injury in the obese surgical population.[38,39] Venous access is more difficult in this population, making both intravenous line insertion and laboratory blood sampling quite challenging[40] [Table 2].
Preoperative challenges in obese patients undergoing proximal femur procedures
Intraoperative Challenges
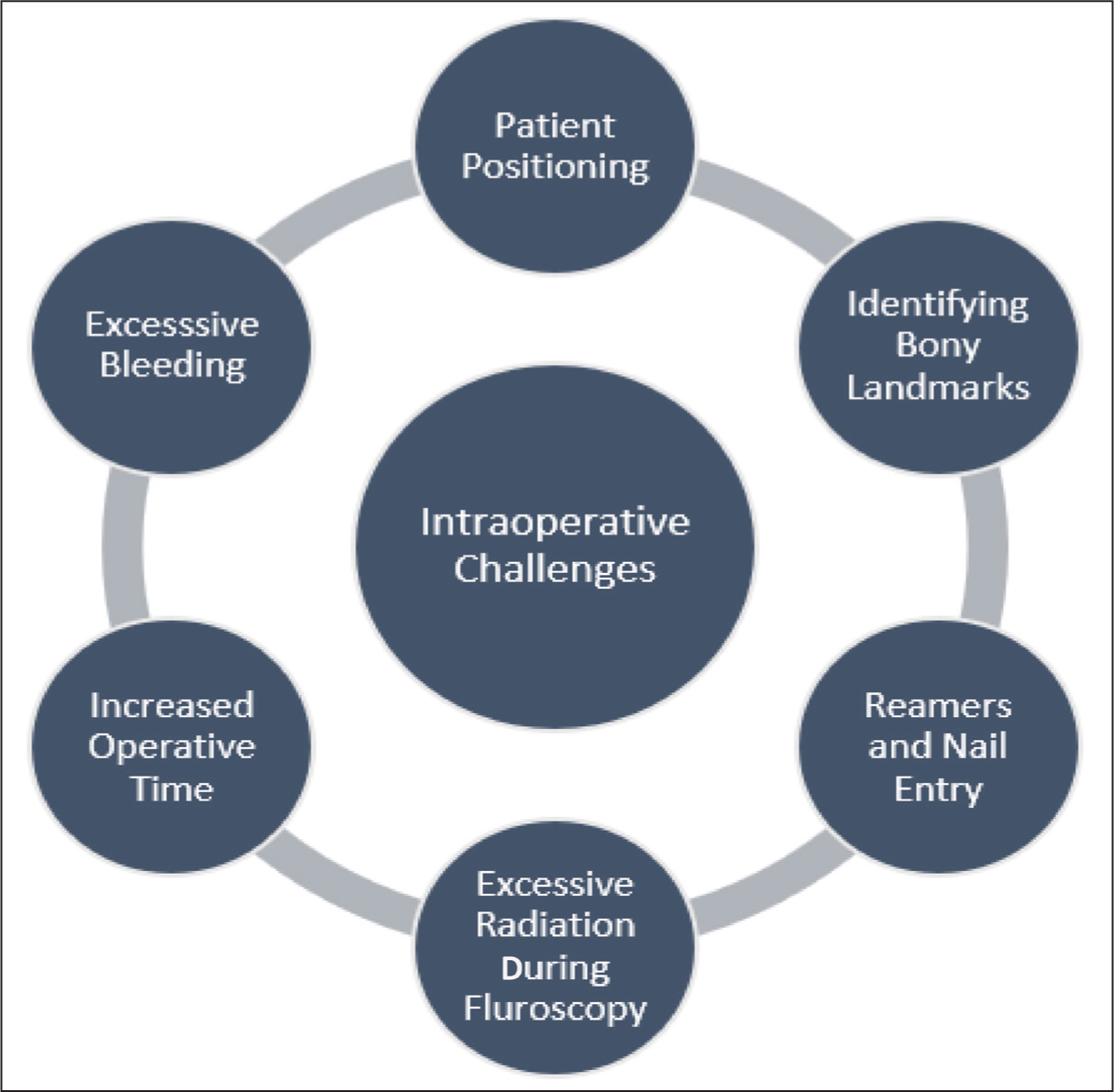
During intramedullary nailing of the femur in obese patients, there are unique difficulties related to patient positioning, fracture table use, and surgical technique [Figure 1].
Intraoperative challenges
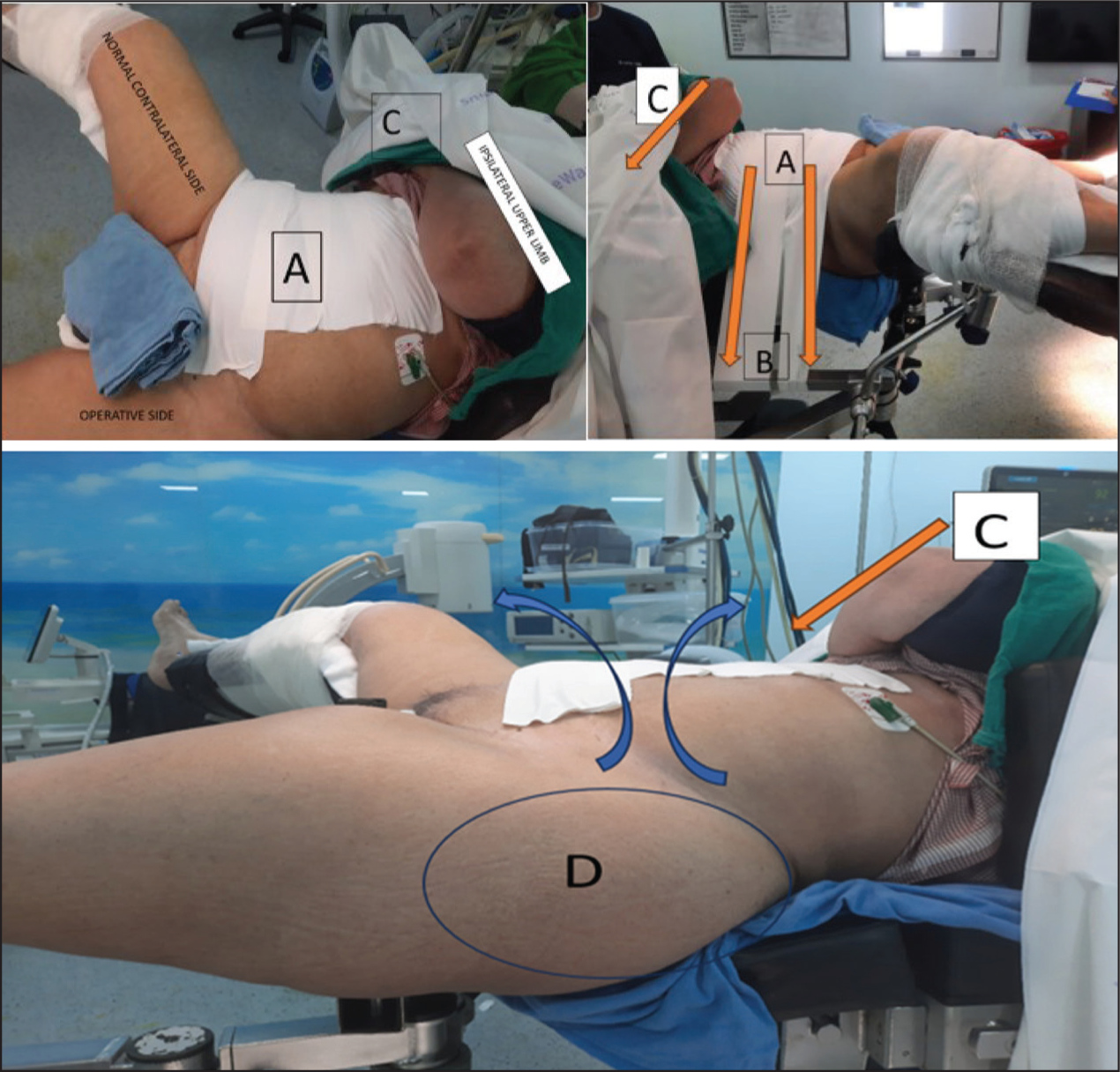
Positioning challenges in supine obese patients frequently include a large abdominal panniculus obscuring the greater trochanter entry site, pendulous breasts impeding in-line reaming, and excessive thigh soft tissue hindering lateral imaging. To address these issues, a multi-step taping technique is employed.[41] First, liquid adhesive is applied to the abdomen below the breasts and along the midline to improve tape adhesion and prevent skin tears. Silk tape is then placed over the adhesive to create an anchor. A second adhesive layer and vertical silk tape are applied along the midline, followed by horizontal tape strips extending to the contralateral side of the table to retract the panniculus [Figure 2]. The ipsilateral arm is secured across the chest, and the torso is stabilised to prevent intraoperative shifting. This arm positioning also aids in upper torso rotation, further displacing soft tissue. Finally, the contralateral limb is positioned to minimise soft tissue interference with lateral fluoroscopic imaging.[41] Fracture table use in obese patients carries risks of perineal injury or injury to suspended extremities due to excessive traction, as well as well-leg compartment syndrome or nerve palsy, especially in the hemi-lithotomy position, exacerbated by increased soft tissue pressure from knee flexion.[42,43]
Abdominal panniculus taping [liquid adhesive is applied to create a sticky surface on the skin, protecting against skin tears, with surgical tape (silk) placed on top to form a base for additional tape in multiple directions. Tape is placed along the patient’s midline (A), extending to the opposite side and secured to the table (B), pulling the central abdominal panniculus and excess soft tissue away from the midline. (C) The ipsilateral arm is positioned over the chest, pulled across to the contralateral side, and taped to the bed to rotate the upper torso. (D) Improved exposure of the proximal hip is achieved, with reduced overhanging abdominal tissue, providing better access for the intramedullary nail insertion, compared to the contralateral hip, which is obscured by excess tissue.]
Surgical challenges include difficulty identifying anatomical landmarks and cumbersome nail entry due to imaging and reduction difficulties.[2] In obese patients, while performing the surgeries involving fluoroscopy, there is an excessive radiation exposure to the surgeon as well as the patient, as compared to operating on a non-obese patient.[44]
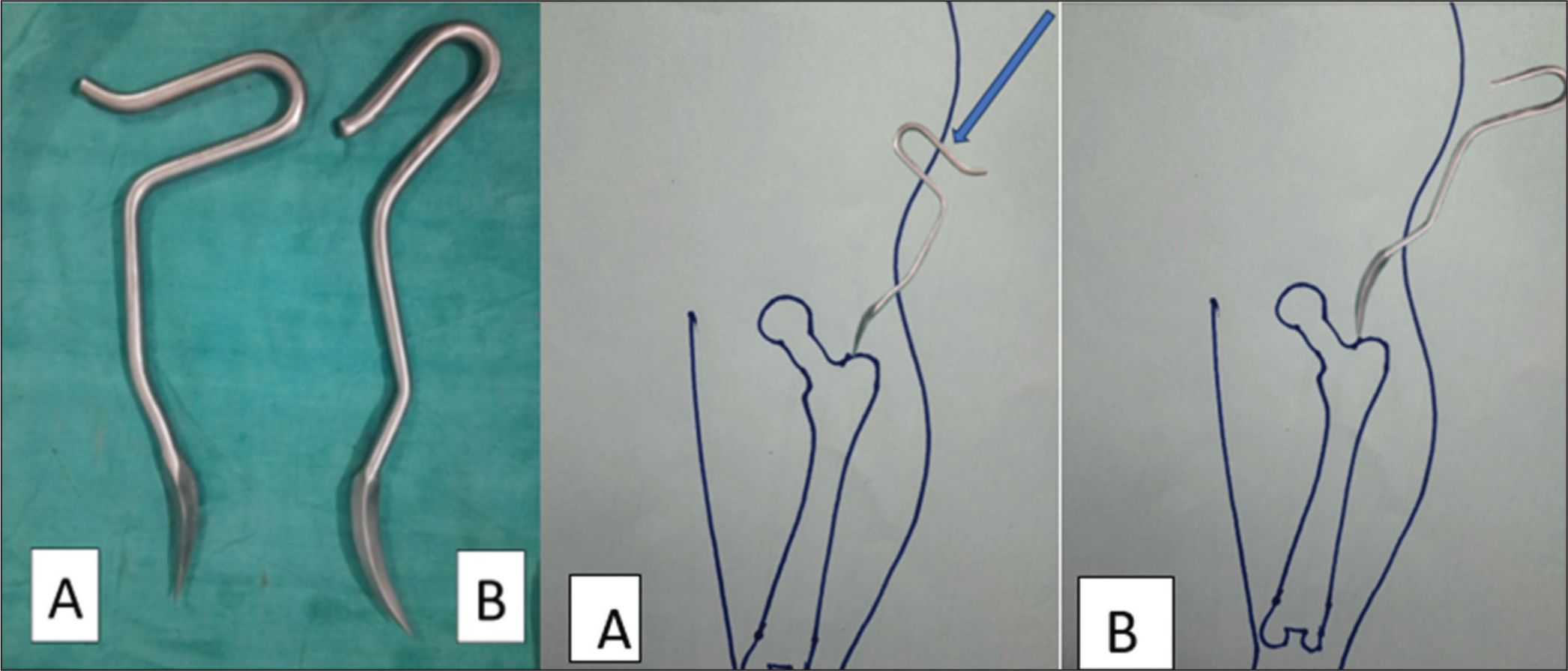
Guidewire deflection by the abdominal panniculus can be problematic. An awl can better penetrate subcutaneous tissue and allow for medial pressure against the panniculus while maintaining guidewire control.[41] Using routine straight or small curved awls can also find difficulty in making the entry point, so an awl with a high horizontal offset handle can be used to overcome this issue [Figure 3]. These awls are not readily available, and if you are working in a tertiary setup with a high volume of such patients, then it is prudent to get a custom-made high-offset awl for use. This will enhance the ease and improve the overall functional outcomes at the same time, reduce the intraoperative time and difficulties.[45]
Comparison of normal and high offset entry awl in obese patients
After establishing the starting point, a guidewire is inserted through the awl before reaming. Reaming itself is complicated by soft tissue pressure on the rigid reamer, potentially leading to lateral entry or femoral shaft fracture. Rigid reamers are also prone to lateralisation due to soft tissue and iliac crest pressure. To mitigate these risks, a flexible reamer with a double-prolonged Hohmann retractor is used. The retractor applies medial pressure to the starter wire to prevent lateral deviation. If lateral deflection occurs, the retractor medialises the reamer distally. The flexible reamer maintains its rotational axis, and the retractor counteracts lateralisation from medial soft tissue compression.[46]
During reaming the femoral canal with flexible reamers, skin abrasions due to excessive overhanging pendulous skin have been extensively reported. Care should be taken by using tissue protection sleeves and taping of excessive loose skin. Superficial abrasions near the entry points make it more susceptible to superficial infections and difficult wound management, which in turn may lead to inferior functional outcomes.[47]
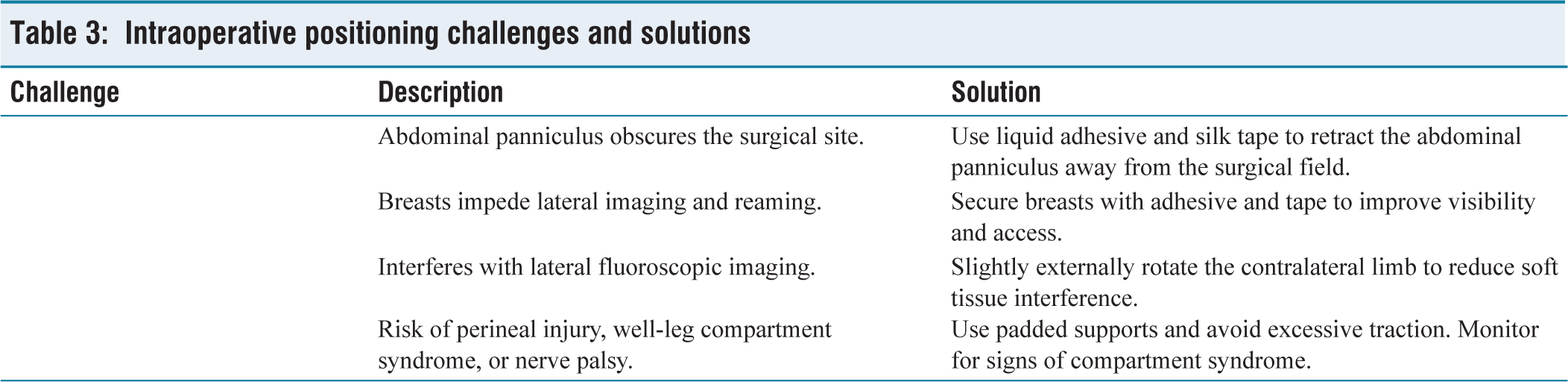
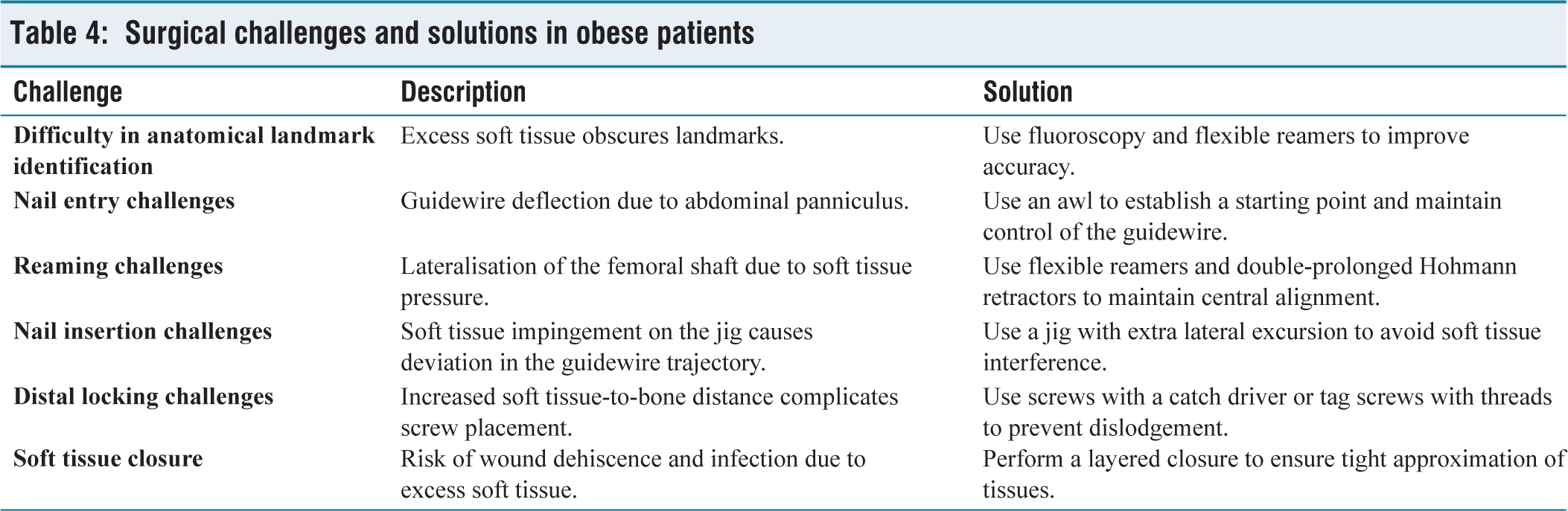
Nail insertion can be hampered by soft tissue impingement on the jig, causing guidewire deviation and suboptimal lag screw placement. A jig with increased lateral excursion allows percutaneous lag screw placement, avoiding soft tissue impingement.[41] For distal locking, accurate entry point location is crucial. If the soft tissue-to-bone distance is large, tagging the screw or using a catch driver can prevent dislodgement. Finally, layered soft tissue closure is essential for a tight closure [Tables 3 and 4].
Intraoperative positioning challenges and solutions
Surgical challenges and solutions in obese patients
Postoperative Challenges
The main known challenges include wound care, pneumonia, pressure sores, thromboembolism prevention, and rehabilitation strategies for obese patients. Postoperative complications following surgery in obese patients present a significant clinical challenge. Wound complications, including infection and dehiscence, are more prevalent in this population due to factors such as increased tension on wound closures, larger surgical incisions, compromised blood supply to adipose tissue, and the presence of skin folds that create a warm, moist environment conducive to bacterial growth.[2]
Subcutaneous seroma formation has been reported to increase with the increase in subcutaneous fat thickness. As the depth to bone increases, the chances of having potential dead spaces in soft tissue planes also increase. This leads to higher chances of developing a collection, and therefore, putting a subcutaneous drain can aid in countering this problem.[48]
Pulmonary complications, such as pneumonia and atelectasis, are also of heightened concern due to reduced functional residual capacity, impaired diaphragmatic excursion, and increased risk of aspiration. The risk of pressure ulcers is elevated due to increased weight bearing on bony prominences and potential for prolonged immobility. Furthermore, obese patients are at increased risk for venous thromboembolism (VTE), including deep vein thrombosis (DVT) and PE, due to a combination of factors, including increased venous stasis, hypercoagulability, and impaired fibrinolysis, and therefore fixed-dose LMWHs may be suboptimal in this population. Current practice guidelines recommend utilising weight–based dosing of LMWH in obese patients, that is, 0.5 mg/ kg subcutaneously once daily instead of a fixed 40 mg subcutaneous once daily dose.[49]
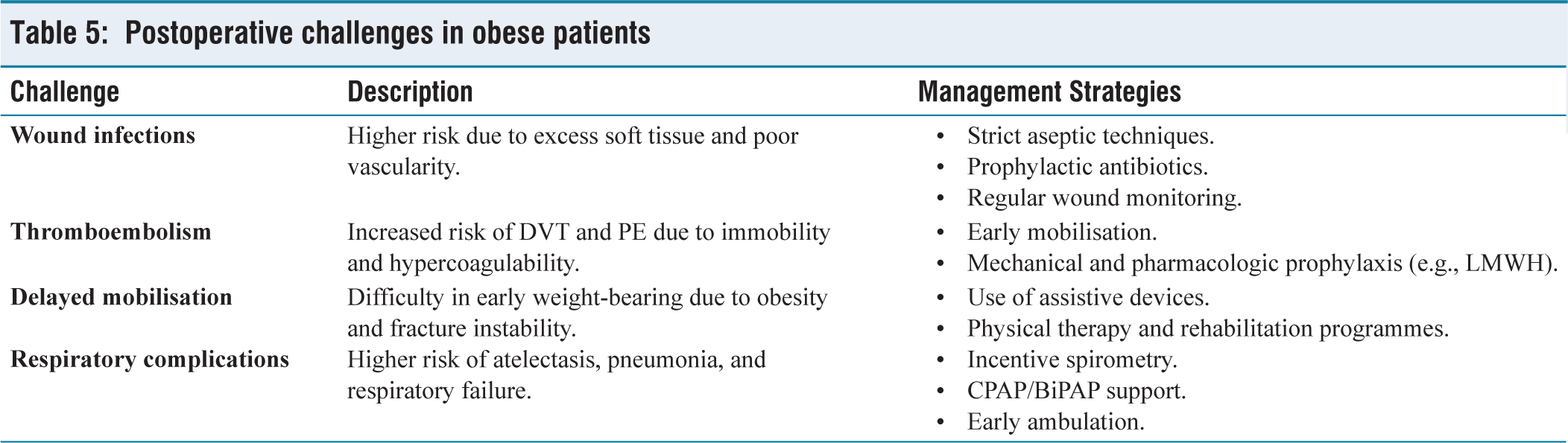
Finally, effective postoperative rehabilitation requires careful consideration of the patient’s weight, potential comorbidities, and any specific surgical restrictions to optimise functional recovery while minimising complications. Addressing these potential complications through meticulous surgical technique, diligent postoperative care, and a multidisciplinary approach is crucial for optimising outcomes in obese patients undergoing a procedure [Table 5].
Postoperative challenges in obese patients
Conclusion
This study has comprehensively outlined the multifaceted challenges encountered in the perioperative management of obese patients undergoing proximal femur fracture surgery. Preoperatively, careful attention must be paid to the increased prevalence of OSA, cardiovascular comorbidities, altered pharmacokinetics, and difficult airway management in this population. Intraoperatively, specific strategies, including modified positioning techniques, specialised equipment, and meticulous surgical technique using flexible reamers and retractors, are essential to overcome challenges related to soft tissue, imaging, and fracture reduction. Postoperatively, vigilance regarding wound care, thromboembolism prevention, respiratory complications, and tailored rehabilitation protocols is paramount. By proactively addressing these challenges through a multidisciplinary approach, surgeons can optimise outcomes and minimise complications in obese patients undergoing proximal femur fracture repair. A key learning point is the importance of recognising the ‘obesity paradox’, where, despite increased risks, some obese patients may exhibit better outcomes in certain situations. This underscores the need for individualised patient assessment and management, moving beyond generalised assumptions about obesity and surgical outcomes.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Not required as this is not using patient data.
Credit author statement
RS: Conceptualization, Writing, Methodology, data search
AV.: Data curation, Writing- Original draft preparation, editing
RV: Visualization, Investigation, Editing, Concept
Disclaimer
The views expressed in the submitted article are our own and not an official position of the institution or funder.
Use of artificial intelligence
AI tools were used to improve the english and used as a part to streamline the already searched articles.