
Abstract
Background:
Musculoskeletal (MSK) medicine has undergone a rapid transformation in recent years, with artificial intelligence (AI) emerging as a key driver of innovation. Existing literature has predominantly explored AI in diagnostic imaging, predictive analytics, and Natural Language Processing for clinical decision support. While several studies have touched upon AI’s potential in medical education, there remains limited evidence specifically evaluating its role in MSK teaching, the pedagogical outcomes, and integration into established curricula. This gap is critical given the changing dynamics of healthcare delivery, the need for scalable training solutions, and the increasing emphasis on personalised, technology-driven learning. The current work addresses this shortfall by synthesising recent evidence and examining how AI-based tools can enhance MSK education.
Methods:
A comprehensive literature search (2018–2025) was conducted across PubMed, Scopus, and Web of Science using predefined keywords relating to AI and MSK teaching. Eligible studies were peer-reviewed articles, case studies, and trials in English that met specific inclusion criteria. From the 342 screened articles, 43 were selected for detailed analysis. Data extraction focused on AI applications in MSK training, reported benefits, limitations, and integration strategies. Non-peer-reviewed and opinion-based sources were excluded.
Inclusion criteria:
Peer-reviewed articles, case studies, and trials published in English between January 2018 and 2025, focusing on AI applications in MSK education among healthcare professionals in training. Both qualitative and quantitative studies were included.
Exclusion criteria:
Non-peer-reviewed articles, editorials, opinion pieces without empirical evidence, studies on non-human/animal subjects, and studies unrelated to AI or MSK systems.
Results:
The literature reveals that AI has enhanced MSK training through immersive technologies such as 3D modelling, augmented reality (AR), and virtual reality (VR). These innovations reduce reliance on traditional cadaveric and apprenticeship-based models, offering cost-effective, scalable, and interactive learning. AI-driven platforms facilitate personalised case-based learning, improve diagnostic accuracy, and support tailored intervention planning. However, significant challenges remain—most notably, limited longitudinal data on educational outcomes, barriers to large-scale adoption (cost, infrastructure), data privacy concerns, and the absence of standardised frameworks for integrating AI into formal MSK curricula.
Conclusion:
While AI shows considerable promise in transforming MSK teaching, the field lacks robust, outcome-focused research to guide evidence-based adoption. Addressing these gaps through targeted studies, standardisation of teaching protocols, and blended integration with conventional training will be essential to realising AI’s full potential in enhancing both learner competence and patient care outcomes.
Keywords
Introduction
With growing prevalence of musculoskeletal (MSK) disorders, ranging from osteoporosis to intricate bone fractures, and the rise in complex MSK tumours necessitate upgrading traditional teaching methods. Conventional MSK education often relies on the use of cadavers, which may be limited by availability, ethical considerations, and institutional resources.[1] Obstacles in improving patient outcomes by rectifying the chances of human errors and increasing surgical accuracy can be mitigated using artificial intelligence (AI).[2] These limitations can be addressed through AI, which favours better visualisation of structures, improving diagnostics, and providing better learning experiences with immediate feedback.[3] AI has even made non-clinical tasks essential for new trainees, such as record keeping, patient scheduling, and patient safety, much easier.[4]
Methodology
Literature Inclusion and Exclusion Criteria
Data was gathered from peer-reviewed articles, case studies, and conference proceedings. Both qualitative and quantitative studies, including randomised controlled trials, observational studies, cohort studies and expert opinion papers have been reviewed. Studies focusing on the application of AI in MSK education among health professionals in training were included. Studies published from 2018 to 2025 in English were included in the search.
Non-peer-reviewed articles, editorials, and opinion pieces without evidence are excluded. Studies involving animal models or non-human subjects are omitted. Studies not related to AI or MSK systems are not considered.
Manuscript Selection and Data Extraction
A thorough search was conducted in various databases like PubMed, Scopus and Web of Science using keywords, including ‘AI in MSK training’, ‘Machine learning in MSK teaching’ and ‘AR and VR in MSK disorders’. Studies meeting the inclusion criteria were considered, and reviewers independently extracted data. Boolean operators were applied to refine the search and ensure the inclusion of studies pertinent to both AI technologies and MSK education.
Search and Selection Process
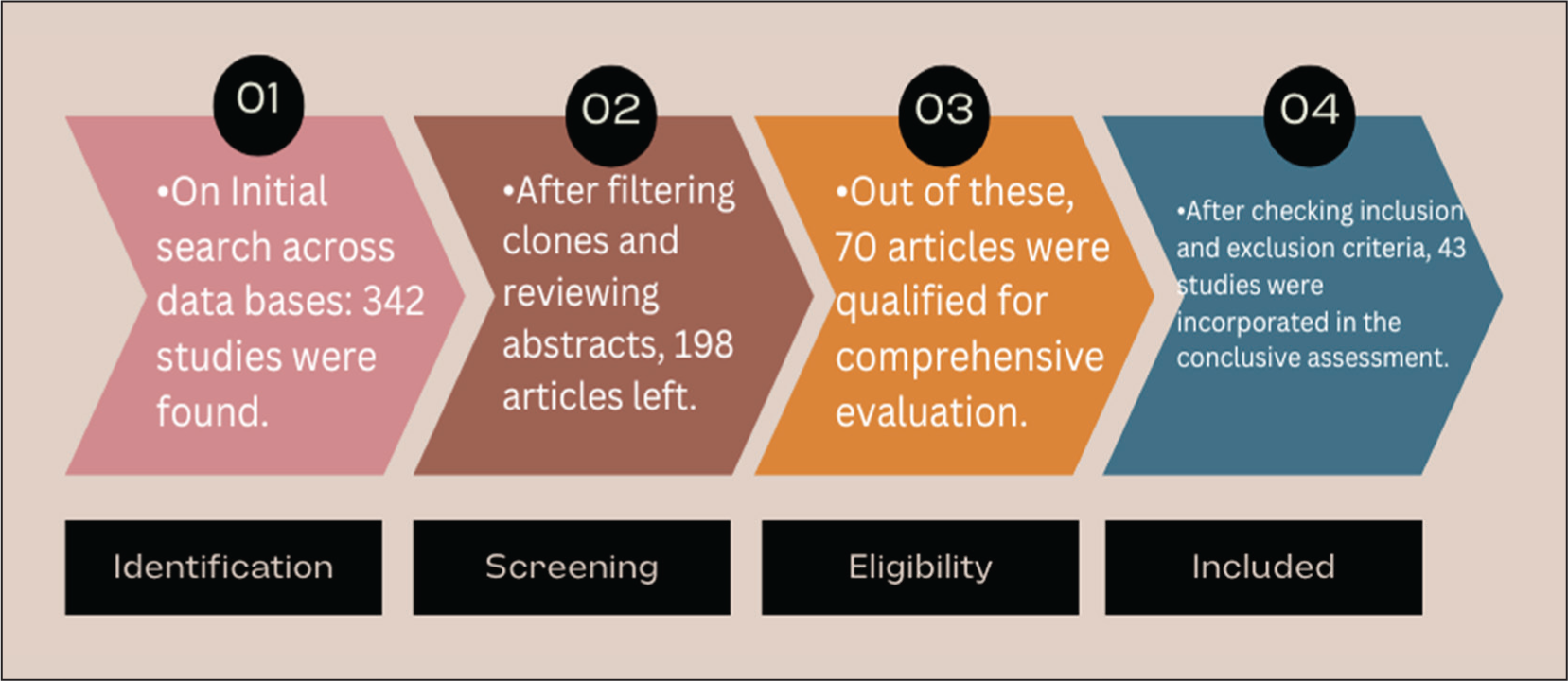
A literature search was conducted from January 2018 to 2025 across PubMed, Scopus, and Web of Science. Initial screening found 342 articles. After filtering clones and reviewing abstracts, 198 articles were left. Out of these, 70 articles were qualified for comprehensive evaluation. After checking the inclusion and exclusion criteria, 43 studies were incorporated into the conclusive assessment. The selection process is illustrated in the flowchart below [Figure 1]:
PRISMA-style flowchart showing the literature search and selection process, including the number of records identified, screened, assessed for eligibility, and included in the final review
Research Objective
The research aims to detect well-established AI models that constitute innovative technologies and novel educational methods. It explores the benefits of developing skills and potential obstacles in implementing these models.
Generations of AI Correlating with Development in MSK Medicine
The development of AI through three generations has changed its application to the evolving field of MSK medicine. It has undergone a transition from basic data-led algorithms to advanced neural networks and deep learning.
The First Generation of AI, also known as Symbolic AI, was based on basic algorithms to solve problems. It helped physicians by using logical frameworks to present simulations to teach the data and make decisions. It relied more on predetermined equations and needed more intervention.[5]
Second Generation of AI, also known as Machine learning, works by processing the provided data, recognising patterns with minimal indulgence by physicians.[6] The supervised model needs labelled data with human contribution before its practical application, whereas the unsupervised model works by assessing patterns from data provided. It is used in processing radiology and histopathology images and finding specific disease markers.[7]
The Third Generation of AI, Deep learning, has proved to be revolutionary because it mimics the human brain by creating artificial neural networks that have the capacity to process massive data in the shortest time. Neural networks process input data using hidden layers and the backpropagation technique for training.[8] It has the capability to detect minute changes and can detect conditions like osteoarthritis, bone fractures, and tumours efficiently.[9–11]
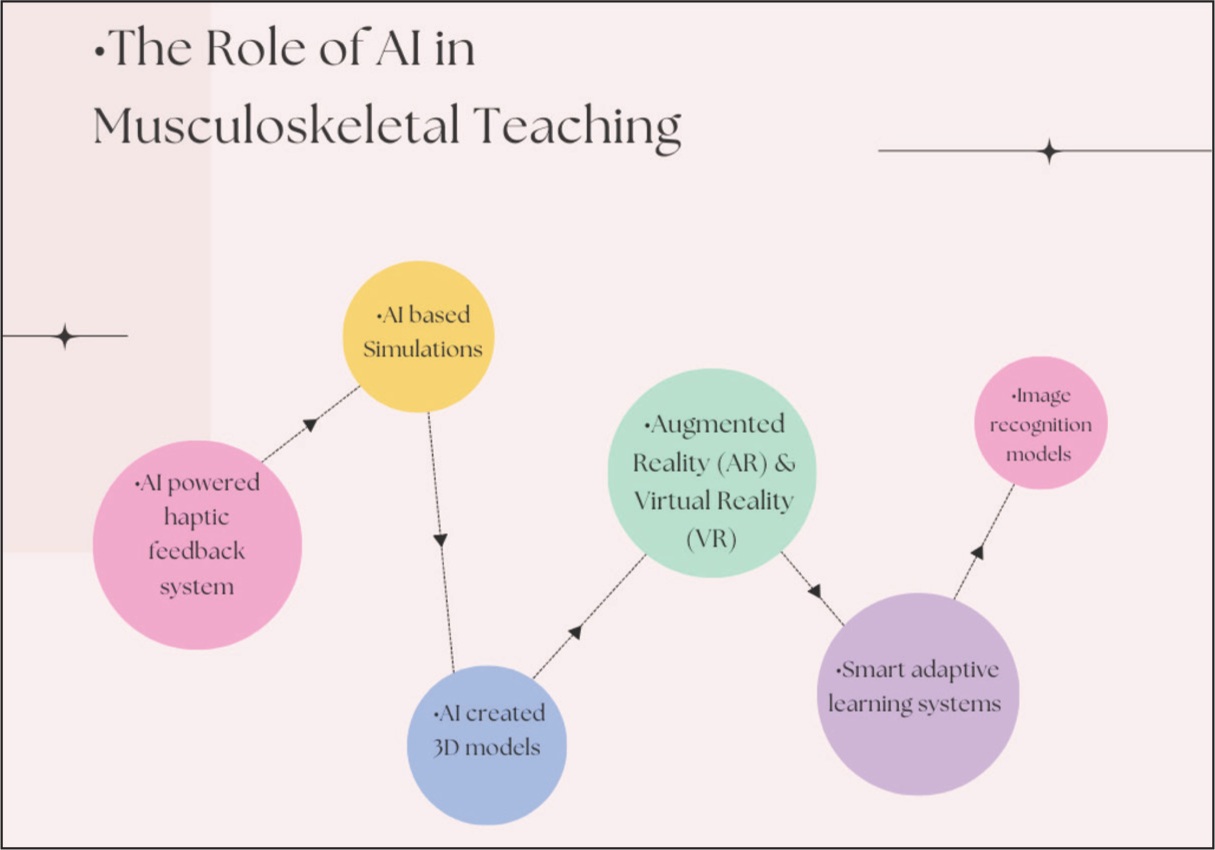
Reinforcement Learning makes decisions on an exploratory hit-and-miss basis, receiving rewards or penalties for enhancing long-term outcomes. It can help to make an individualised rehabilitation plan by analysing patient progress over time. Natural Language Processing, Computer vision and AI-driven data analytics are some of the additional advancing AI tools in MSK education [Figures 2 and 3].[12]
Illustration of the various ways AI can be applied in musculoskeletal education, including 3D modelling, augmented reality (AR), virtual reality (VR), adaptive learning platforms, and AI-assisted diagnostic tools
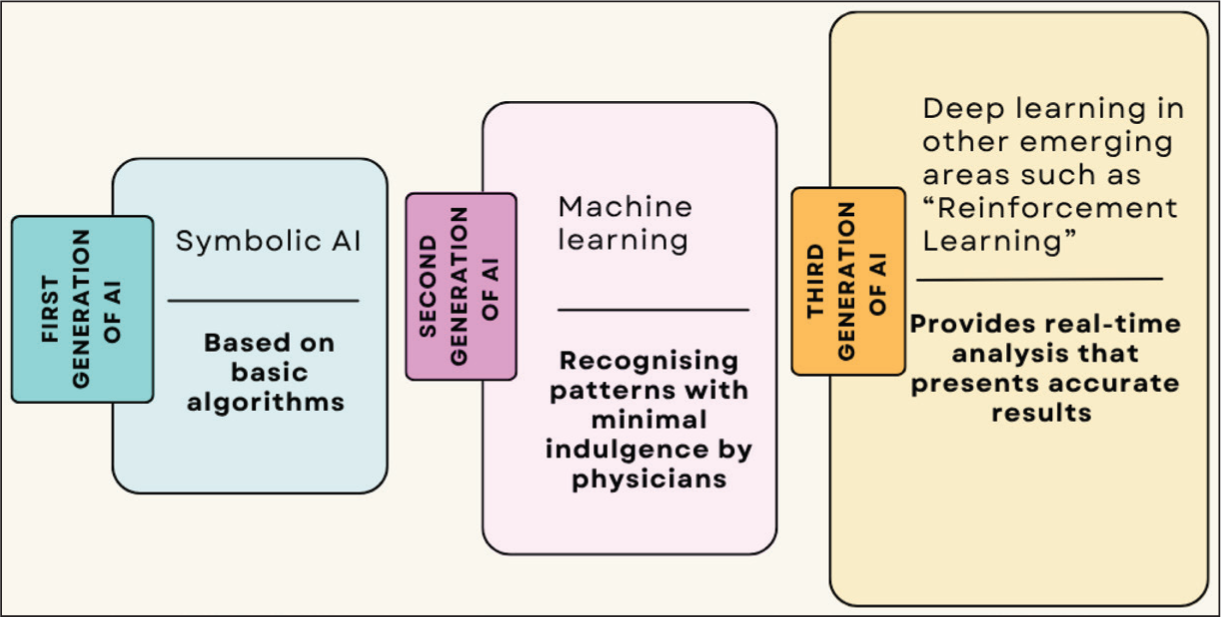
Diagram summarising the three generations of AI (Symbolic AI, Machine Learning and Deep Learning) and their respective applications in musculoskeletal medicine and education
Role of AI in Musculoskeletal Training and Teaching
AI-created 3D models have reduced the dependence on cadaveric teaching by forming high-quality 3D representations of bones, muscles, joints, tendons, and ligaments, providing an immersive learning experience.[13] The Visible Body and Complete Anatomy platforms allow students to handle and dissect anatomical virtual structures. They adjust difficulty levels to tailor the learning experience, allowing progress at one’s own pace and providing personalised feedback, aiding in reinforcing concepts.
Augmented reality (AR) can be used as a way to understand anatomical structures by overlaying anatomical images over the human body. Platforms like Complete Anatomy use AR to allow learners to explore and manipulate these 3D models. The use of 3D spinal images on cadavers has helped trainees to make precise cuts by using probes with accurate assessment.[14]
Cost-effectiveness and Resource Optimisation
Organisations have seen enormous cost savings after incorporating AR-based models as compared to conventional cadaveric labs by eliminating the high acquisition, conservation, and disposal costs. These models provide unlimited access to various anatomical structures without added costs, offering a high return on investment.[13]
Virtual reality (VR) can generate an interactive virtual world that mimics real-life operating experiences, helping learners to perform complex procedures, reducing errors in real-life scenarios.[15] Microsoft HoloLens authorises trainees to have hands-on experience with MSK structures using holographic displays.[16] A randomised controlled trial assessed the effectiveness of VR training in total hip arthroplasty on 24 surgical trainees and found that VR-trained surgeons performed better.[17]
Building Confidence and Decreasing Errors
VR facilitates understanding and retention of spatial orientation. These models respond as real patients in clinical scenarios, requiring trainees to use reasoning for each step.[18]
AI-based on data-driven feedback has upgraded clinical diagnosis and treatment planning by interpreting data quickly.[19] It aids trainees in reviewing MSK cases to understand complex diagnoses and build clinical reasoning. Image recognition models have led to the early detection and automatic categorisation of MSK disorders.
Use of AI in MSK Diagnosis
Cognitive computing platforms, like Qure.ai and Aidoc, facilitate the interpretation of X-ray images, correctly identifying anomalies like fractures, dislocations, and degenerative changes in joints. Advanced AI models can even analyse CT and MRI scans to detect tumours.[20] For example, AI has automated the process of diagnosing and classifying the stage of osteoarthritis. It leverages current standard guidelines, incorporating step-by-step instructions based on expert data, thereby ensuring compliance with established standards.[21] Case-based quizzes can also be used for assessment, as the outcome is tested against proficiency standards.[22]
Adaptive learning systems lay out detailed explanations, reference materials, and techniques to comprehend the task efficiently. They track progress using graphs and charts, motivating students.[23]
One example is Anki AI-enhanced flashcards that are based on spaced repetition methods, focusing on weak areas, and amplifying recall. The addition of the AMBOSS add-on for Anki offers support by providing medical facts, explanations, and images drawn from its own library directly onto the flashcards.[24]
AI can review patient data to create patient-centred pre-operative plans, selecting the correct implants, and weighing risk-to-benefit ratios for surgeries. These systems have made patient information storage easy and data extraction user-friendly.[25]
With the advent of AI-based Simulations, trainees can practice examinations, injections, and surgical procedures in a safe environment. Robotics allow surgeons to focus on the correct position and alignment of the implant. Touch surgery is a popular AI-based surgical simulation model that offers guidance and live feedback.[26]
AI-powered haptic feedback system responds to interventions, producing vibrations and sounds, helping trainees to recognise mistakes and challenge themselves.[27] Mannequins, like SimMans, are designed to respond like a normal human body.[28]
AI can analyse larger databases in a relatively short time, giving an edge to identify the patterns, potential prognosis and suitable management by interpreting relevant factors. It holds predictive value in the progression of osteoarthritis using the given MRI inputs.[29]
Intelligence-led research studies help to find the possible aetiologies for a particular disease based on patient data. This can aid in preventing modifiable risk factors in vulnerable populations.[30] AI models can assimilate data from electronic patient records, wearable devices and genetic information and by reviewing this data, trainees can predict disease progression, length of hospital stay, and need for readmission.[31]
Availability of online lectures, global webinars, and continuous patient monitoring has provided an opportunity to study MSK surgery even for a remote audience.[32] Trainees can sharpen interpersonal skills by practising with Natural Language Processing-based AI voice simulators. Trainees can use accessible technologies like ChatGPT to get information about MSK presentations and summarisations to ease their job. The question arises whether it can be completely relied upon because it has generated false information in some instances.[33] This phenomenon, called ‘hallucinations’, makes its use limited and raises safety concerns.[34]
AI-powered devices can assess gait, predicting the likelihood of possible orthopaedic or MSK disorders.[35]
Integration of AI into MSK training can transcend geographic and resource limitations, making high-quality healthcare education accessible to learners across the globe.[36]
It has decreased the healthcare costs by improving patient outcomes, reducing readmissions, owing to early diagnosis and management.[37] Systematic errors in AI-powered models can result in mishaps. This can be overcome by constantly updating the AI systems with multifaceted and equitable data collection. Therefore, AI should be used in conjunction with human intervention and not as a tool to replace human involvement.[38]
Strengths of the Study
This study is one of the few to specifically examine the role of AI in MSK teaching, making it highly relevant to both clinical and educational practice. It is strengthened by a comprehensive literature search across three major databases with clearly defined inclusion and exclusion criteria, ensuring the quality and relevance of the included studies. The review covers a wide range of AI applications, from 3D modelling, augmented and VR, to adaptive learning platforms and deep learning models, providing a broad yet focused overview. It balances discussion of the benefits—such as cost-effectiveness, scalability, and personalised learning—with challenges like data bias, ethical considerations, and infrastructure needs. By linking technical AI concepts to practical MSK teaching and offering examples of real-world tools, the study not only synthesises current knowledge but also identifies key gaps and future research directions, giving it strong academic and practical value.
Limitations of the Study
This review is limited by its restriction to English-language publications, which may exclude relevant studies in other languages. The search period (2018-2025) may omit earlier but potentially significant work. Publication bias may have influenced the pool of available literature, as studies with negative or inconclusive findings are less likely to be published. Furthermore, heterogeneity among included studies in methodology, AI tools assessed, and outcome measures precluded meta-analysis. Finally, rapid advances in AI mean that some findings may quickly become outdated, highlighting the need for continual updates.
Challenges
While AI has proved to be transformative for MSK teaching, there are certain limitations that need our attention. One of the most concerning issues is patient privacy.[39] AI-based models require substantial financial investments and technological infrastructure, which can be a daunting task in low-income countries. If the data input is limited or biased, the results can show discrepancies leading to skewed educational outcomes.[38,40] Over-reliance on AI can interfere with the development of critical thinking.[41] While the technology has advanced, experienced MSK surgeons have hesitated to adopt these tools, resulting in improper training.[42]
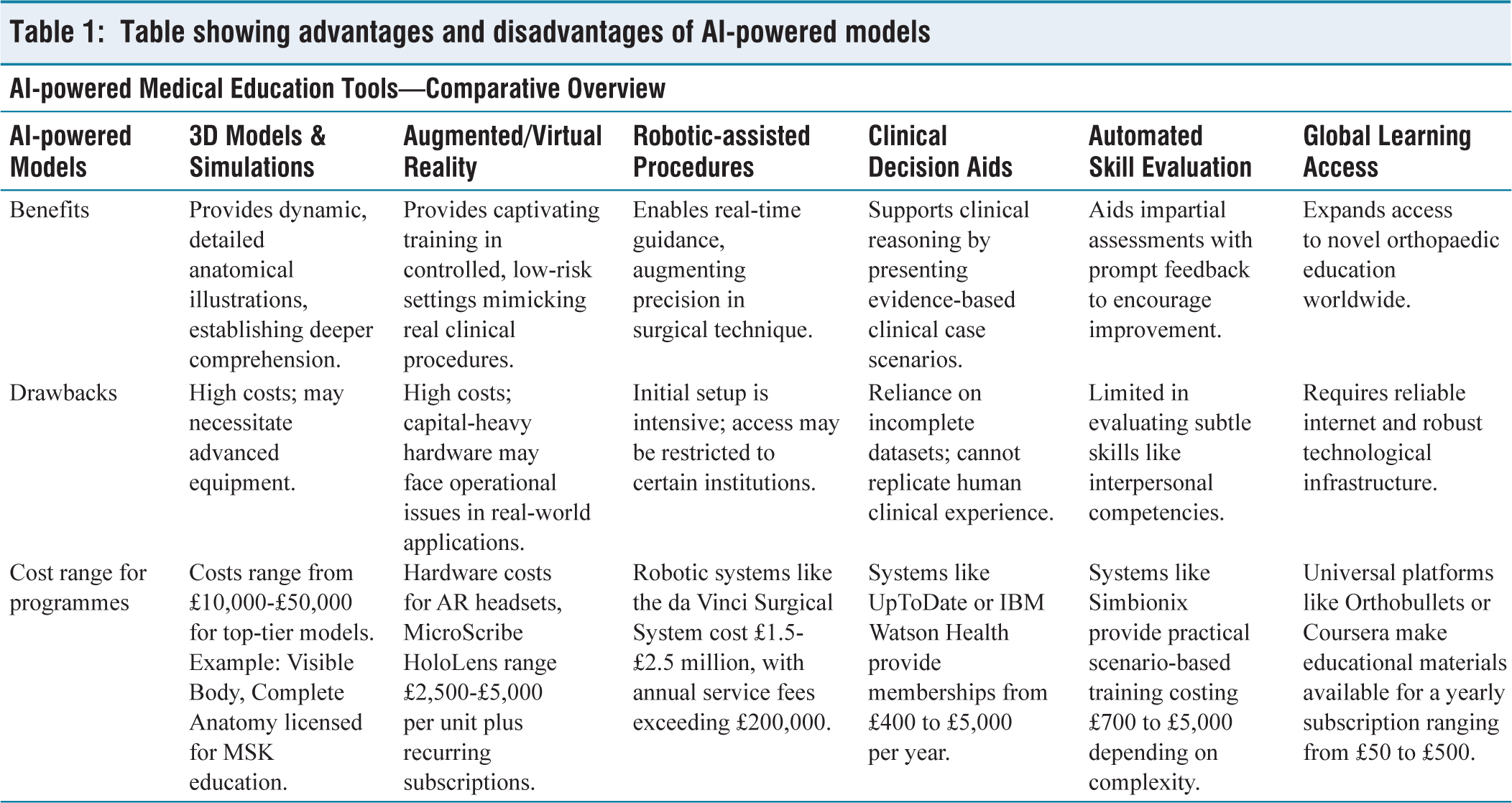
It is essential to arrange specialised funds and to train established surgeons with new AI-based models. Regulatory bodies can provide guidelines and oversee patient confidentiality. The development of error tracking and reporting systems can help in avoiding preventable mistakes. Systematic checks paired with expert feedback from clinicians would mitigate any bias [Table 1].
Table showing advantages and disadvantages of AI-powered models
Conclusion
AI is being deployed in trauma detection, spine anomalies, degenerative diseases, orthopaedic oncology, including both primary and secondary metastasis, estimating bone age, and joint reconstruction. The automation of image analysis and interpreting the results is the most commonly used area of AI in MSK training. These outputs have been widely used by learners to save time and yield high accuracy. One of the drawbacks is the ‘black box’, which means that outcomes generated using AI are intricate and are not easily rendered by learners.[42] There is a need to train datasets to restrain potential systematic inefficiencies. Patients and trainees should be informed about the role of AI in care plans, promoting transparency. AI-based simulation should be followed by a performance on cadavers as a run test before performing procedures on real patients. Periodic assessments using adaptive learning systems can facilitate knowledge retention in the long run.[43] Ecological sustainability should be considered to offset the high computing power required to run these systems [Box 1].
Ten key learning points
1. AI enhances MSK education with immersive tools like 3D models, AR/VR, and simulations, reducing reliance on cadavers.
2. Deep learning and neural networks enable precise diagnosis of fractures, tumours, and joint disorders from imaging.
3. Smart adaptive platforms (e.g., Anki, Complete Anatomy) personalise learning with instant feedback and progress tracking.
4. AI-based simulators and robotics provide safe, realistic training for procedures like arthroscopy and fracture management.
5. Cognitive AI tools (e.g., Qure.ai, Aidoc) assist in radiological interpretation and decision-making for MSK conditions.
6. AI enables cost-effective training by eliminating cadaver-related expenses and allowing scalable learning access.
7. Pre-op planning support: AI reviews patient data to create tailored surgical plans, improving clinical preparedness.
8. Remote learning & global access: AI makes quality MSK education available to trainees in underserved regions.
9. Challenges include data bias, ethical concerns, infrastructure needs, and risk of over-reliance on AI.
10. Human oversight remains crucial—AI should enhance, not replace, critical thinking and patient-centred care.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Not applicable.
Patient consent
Patient consent was not required as no patient data were used.
Credit author statement
Damanjit Kaur: Conceptualisation, Methodology, Writing - Original Draft, Literature Review.
Saavi Reddy Pellakuru: Formal Analysis, Data Curation, Writing - Review & Editing.
Nethra Aryan: Investigation, Literature Review, Writing - Review & Editing.
Jyotika Yerraguntla: Writing - Review & Editing, Visualisation.
Kevin Quinlan: Methodology, Supervision, Writing - Review & Editing.
Vijay Ram Kumar Papineni: Conceptualisation, Supervision, Writing - Review & Editing, Final Approval.
Data availability
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Use of artificial intelligence
No AI tools were used in the preparation of this manuscript.