
Abstract
Background:
Temporomandibular dysfunction (TMD) is a common condition that affects mandible alignment and function, potentially leading to pain and disability during day-to-day activities. Exercise interventions such as Rocabado exercises and muscle energy techniques (METs) may help improve pain, range of motion and function. However, their comparative effectiveness remains unclear.
Aim:
The purpose of this study is to determine the effect of the Rocabado exercise versus METs on pain, mobility and function in individuals with myogenic temporomandibular (TM) dysfunction.
Methods:
A total of 30 individuals were divided into two groups, labelled as Group 1 and Group 2. Group 1 was treated with Rocabado exercises. Group 2 was treated with the MET. Pre and post intervention scores on the numeric pain rating scale (NPRS) linear measurement technique and Fonseca’s questionnaire were taken as outcome measures to check for the pain, range of motion and mobility. analysis was performed by the use of Microsoft Excel and SPSS version 26.
Results:
Both groups demonstrated significant improvements in pain, range of motion and function post-intervention (P < .005 within groups). However, between-group comparisons showed that the Rocabado group had significantly greater improvements in pain (P = .001), range of motion (P = .001) and Fonseca’s questionnaire of functional disability compared to the MET group. This suggests that while both interventions were beneficial, Rocabado exercises were more effective in pain reduction, improving range of motion and function.
Conclusion:
Both Rocabado and MET techniques contribute to improvements in pain reduction, range of motion and function in individuals with temporomandibular joint (TMJ) dysfunction. However, Rocabado exercises provide greater benefits in pain reduction, improve range of motion and overall function of TMJ.
Introduction
The temporomandibular (TM) joint is the articulation between the mandible and temporal bone, allowing movements such as depression, elevation, protrusion, retrusion and lateral excursion essential for mastication, speech and yawning.[1,2] Temporomandibular joint (TMJ) motion involves both rolling and gliding, with mandibular depression requiring 40–50 mm of ROM, while mastication needs about 18 mm.[1,4] Lateral excursion, typically 8–11 mm, involves ipsilateral condylar spinning and contralateral condylar translation.[1,2,3] The lateral pterygoid eccentrically controls disc motion during mandibular movement.[6] Temporomandibular dysfunction (TMD) refers to pain and dysfunction in TMJ and masticatory muscles, often due to muscular or joint pathology.[4,5] Epidemiologically, 75%-90% of people show TMD symptoms in their lifetime, with pain (91%), crepitus (61.2%) and limited ROM (53.3%) being common.[6] TMD is caused by trauma, poor posture, malocclusion, dental procedures, cervical dysfunction and psychological stress.[2,3,5] Forward head posture and upper cervical extension contribute to muscular imbalance and nerve irritation. Inflammatory TMJ conditions such as capsulitis and synovitis cause pain, oedema, limited motion and joint noises.[7,8] Conservative physiotherapy management, interventions are designed to reduce pain, improve jaw function and restore normal movement. The common treatment approach includes patient education, posture correction, manual therapy, dry needling, therapeutic ultrasound and exercises. Physical therapy plays a crucial role in addressing musculoskeletal imbalances, enhancing joint mobility and reducing neuromuscular tension.[9] Recent literature has shown that structured exercise programmes such as the Rocabado 6 × 6 regimen are effective in restoring jaw biomechanics, improving neuromuscular control and alleviating symptoms.[10] The muscle energy technique (MET), on the other hand, is commonly used to treat muscular dysfunction through isometric contractions aimed at mobilising restricted joints and lengthening shortened muscles. Studies suggest myogenic imbalance is more prevalent than articular issues in TMD and responds well to physiotherapy. However, evidence comparing treatment approaches such as Rocabado and MET is limited and requires further exploration for optimal protocols.
Materials and Methods
Study Design and Population
The study received local ethical committee approval. Following approval, the adults aged 25–45 years with diagnosed TM dysfunction have been recruited for the study. Patients with symptoms of locking of jaw, jaw sounds (popping, clicking), presence of pain or limitation of movements due to TM dysfunction, with a history of bruxism (teeth grinding) and teeth clenching, history of myofascial pain, muscle tension or spasm in masticatory muscles or inter-incisal opening of 25–40 mm were included in the study. Patient with severe TM degenerative or inflammatory conditions. Patients with any history of trauma or surgery past six months, any psychological or neurological deficit that affects the facial muscles, pregnant or lactating females were excluded from the study. A total of 30 subjects meeting the selection criteria were randomly allocated into two experimental groups. It was a single-blinded study, where participants remained unaware of their group allocation.
Intervention for Group A: Rocabado 6 × 6 Exercise Protocol
Intervention Protocol:
Group A (Rocabado exercises): Participants performed the Rocabado 6 × 6 protocol, which includes six exercises performed six times daily for six weeks. Exercises included:
Resting tongue position Controlled nasal breathing Rhythmic stabilisation Mandibular controlled opening Head flexion against resistance Shoulder posture correction. Each session lasted approximately 15–20 minutes. Participants were instructed to maintain proper posture and perform exercises in front of a mirror for feedback.
Intervention for Group B: Muscle Energy Technique (MET)
Group B (MET): MET was applied by a trained physiotherapist thrice weekly for six weeks. Each session lasted 20–30 minutes and included:
Isometric contractions of the lateral pterygoid, masseter and temporalis muscles Post-isometric relaxation techniques Gentle mobilisation of the TMJ Stretching of shortened masticatory muscles. Adherence was monitored via weekly logs and therapist check-ins.
All participants were assessed using the assessment format for TM dysfunction. The numeric pain rating scale (NPRS), linear technique and Fonseca’s Anamnestic Index were measured before and after the treatment in both groups.
Statistical Analysis
Normality of the data distribution was assessed using the Shapiro-Wilk test.
Descriptive statistics, including mean ± standard deviation (SD), were calculated for all demographic variables. quantitative data, including scores from Fonseca’s Anamnestic Index, NPRS and Jaw mobility measurements (linear measurement in millimetres), were collected before (pre-treatment) and after (post-treatment) the intervention. The Shapiro-Wilk test was applied to assess the normality of the data distribution. As the data followed a normal distribution, parametric tests were used for statistical analysis. A paired t-test was applied within each group (Group A: Rocabado exercises and Group B: MET) to assess the significance of change between pre- and post-treatment values. An unpaired t-test was used for between-group comparisons to analyse the difference in treatment outcomes between the two groups. The confidence level was set at 95% and a P value < .05 was considered statistically significant for all analyses.
Results
Paired t-tests were used for within-group comparisons and unpaired t-tests were used for between-group comparisons. A P value of < .05 was considered statistically significant. Gender distribution between the groups was measured using the chi-square test. The chi-square value was 0.71, indicating there is no significant difference in the gender distribution between the groups.The gender distribution of participants in the Rocabado and MET groups is provided in Table 1 and illustrated in Figure 1.
Gender distribution in MET and Rocabado group

Gender distribution of MET and Rocabado group
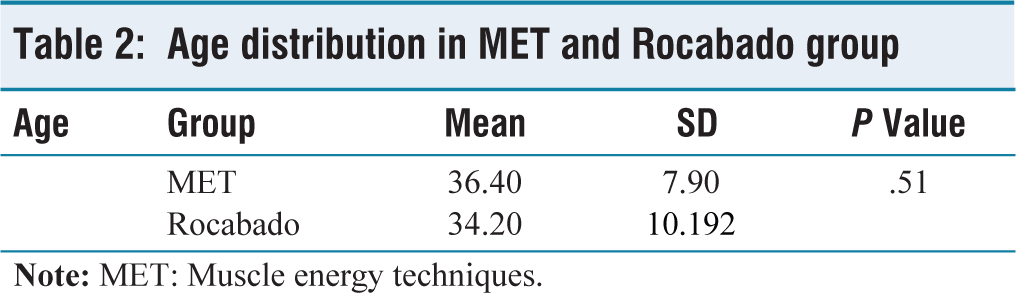
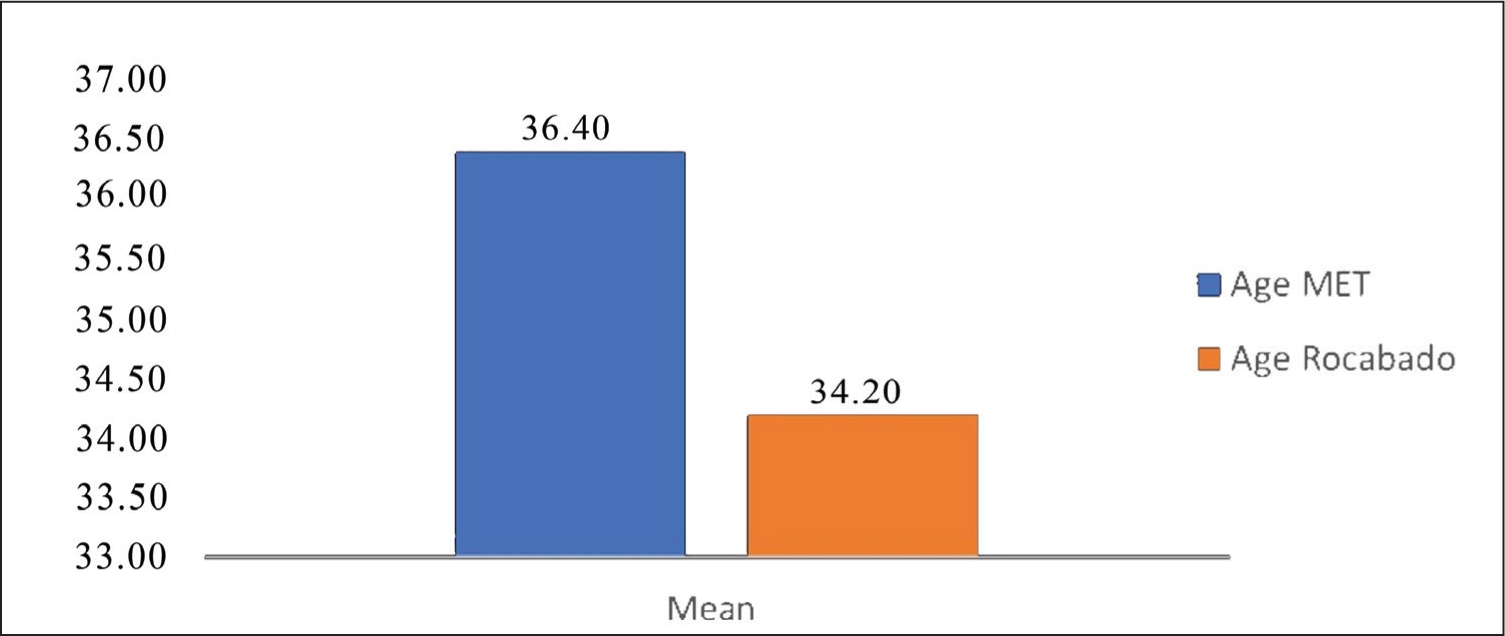
An unpaired t-test was used to find the difference in age distribution between both groups P value of .51 suggests there was no significant difference in age distribution between the groups. The age distribution of participants in both groups is provided in in Table 2 and illustrated in Figure 2.
Age distribution in MET and Rocabado group
Mean graph of age
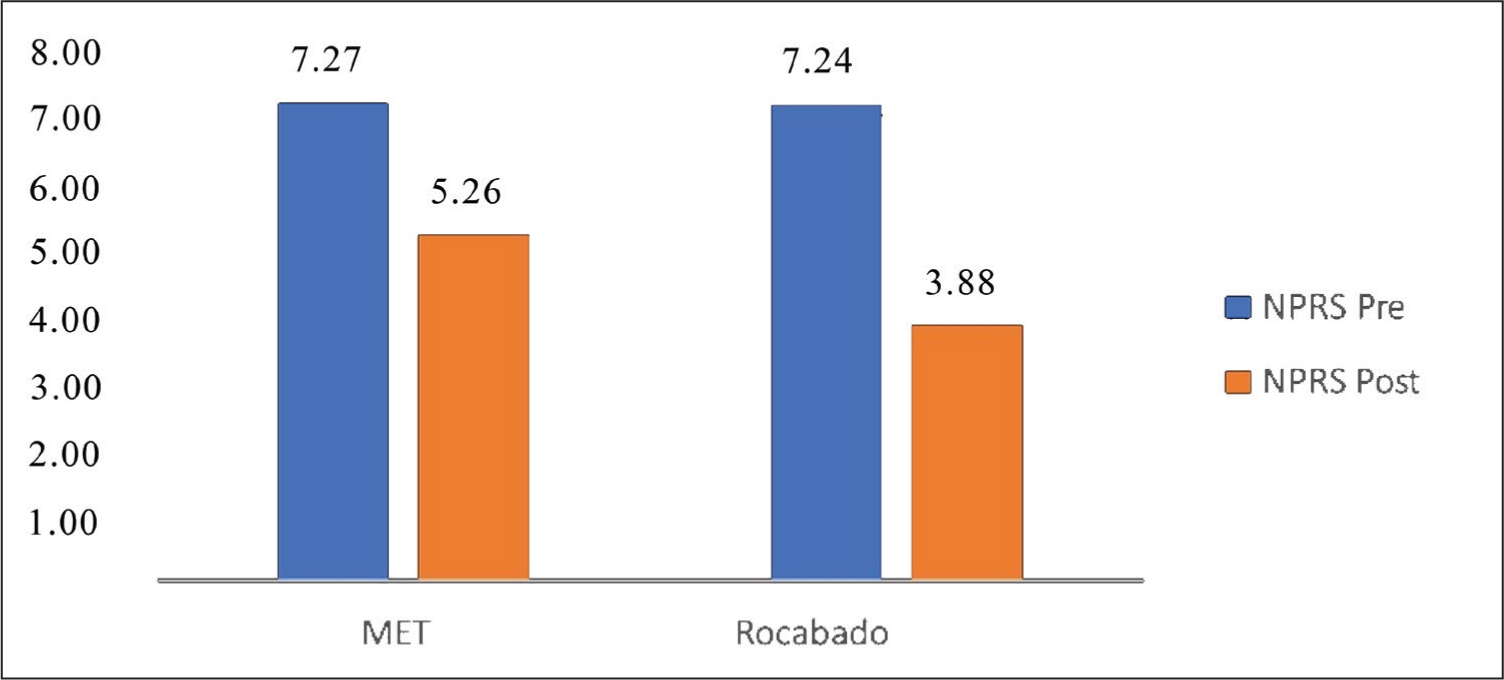
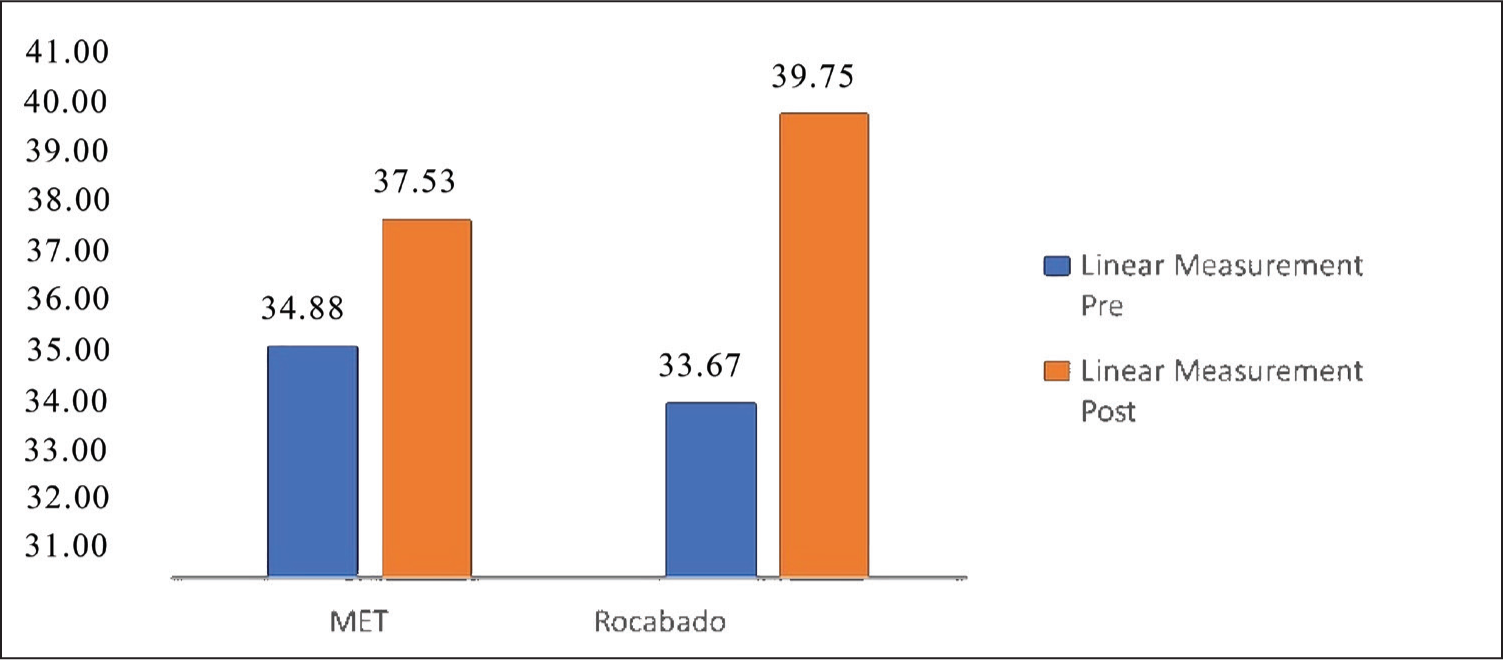
Mean value of pre- and post-test of all the outcome measures, such as NPRS, linear measurement of mouth opening and Fonseca questionnaire of Rocabado exercise group and MET group were analysed by paired t-test. P value is found < .001, which indicates a statistically significant difference was found in the individual group after treatment. The outcomes are presented in Tables 3 and 4. The mean pre- and post-treatment NPRS scores for the MET and Rocabado groups are illustrated in Figure 3, while the mean linear mouth-opening measurements for both groups are depicted in Figure 4.
Pre–post analysis of all outcome measures in the MET and Rocabado groups
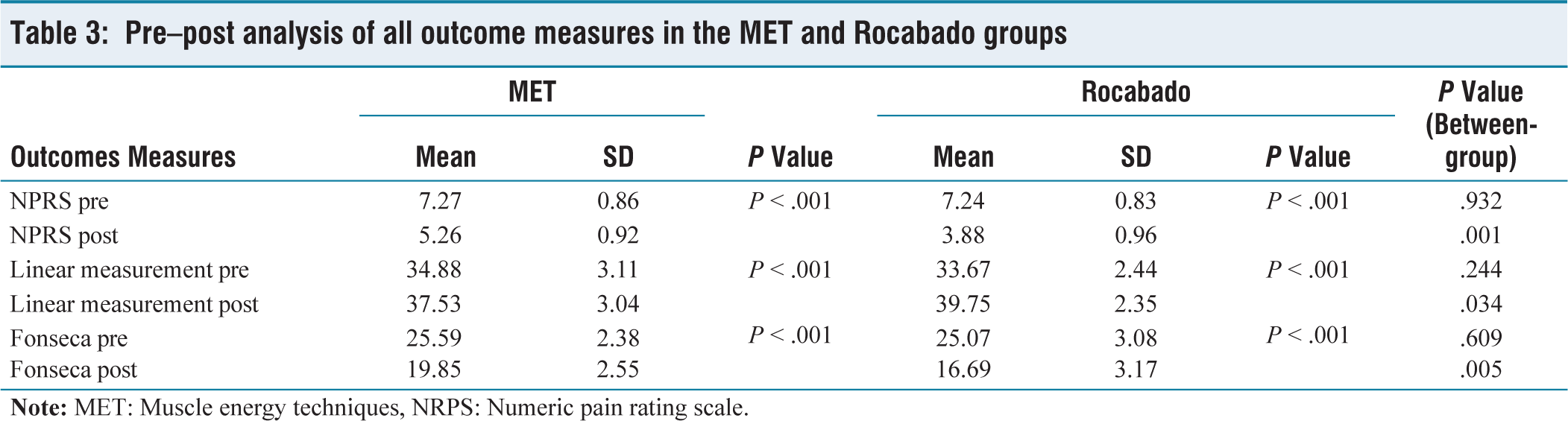
Table showing comparison between MET and Rocabado groups

Mean graph of pre- and post-NPRS of the MET and Rocabado group
Mean graph of pre- and post-linear measurement of MET and the Rocabado group
Mean value of each outcome measure of pretests of both groups was analysed using an unpaired t-test, showing P > .05, indicating there was no statistically significant difference between groups before implementation of exercises. Mean value of each outcome measure of the post-test of both groups was analysed using an unpaired t-test, showing P value < .05, indicating a statistically significant difference between both groups post-treatment, so both the treatment methods are effective, but the Rocabado exercises were more effective than the MET exercise.
Discussion
TMD is a multifactorial condition that affects the TM joint, masticatory muscles and associated structures. This study was designed to compare the effects of two conservative therapeutic approaches, MET and Rocabado exercises, on patients with TMD. The effectiveness of these interventions was assessed using three outcome measures: NPRS, linear measurement of jaw opening for mobility and Fonseca’s questionnaire score of TMD.
Based on the data analysed through SPSS 26, both interventions showed statistically significant improvement in all outcome measures. However, the Rocabado exercises demonstrated superior effectiveness compared to MET. The findings of this study are consistent with previous literature that emphasises the efficacy of neuromuscular and postural correction strategies in managing TMD symptoms. Pain is a primary complaint among TMD patients. In this study, the mean NPRS score for the MET group reduced from 7.27 to 5.26, a 38.15% improvement, whereas in the Rocabado group, it decreased from 7.24 to 3.88, showing an 86.60% improvement. This indicates that both techniques alleviate pain, but the Rocabado exercises provide a more significant reduction. Rocabado’s protocol includes six therapeutic movements aimed at enhancing posture, correcting cranio-cervical alignment and relieving masticatory muscle tension, which may explain its superior outcomes.[11]
Jaw mobility, measured by the linear distance of mouth opening, showed improvement in both groups. MET improved mobility from 34.88 mm to 37.53 mm (7.05% increase), while Rocabado exercises increased it from 33.67 mm to 39.75 mm (15.30% increase). The enhanced mobility in the Rocabado group may be attributed to its targeted approach in restoring muscle balance and joint mechanics through repetitive, structured movements. These findings align with the research by Molina et al. who found Rocabado exercises superior to passive mobilisation in improving TMJ function.[12]
Similarly, Fonseca’s questionnaire score, which measures functional disability, showed improvement in both groups. The MET group’s score reduced from 25.59 to 19.85 (28.91% improvement), while the Rocabado group showed a more substantial improvement from 25.07 to 16.69 (50.26% improvement). The results suggest that functional disability due to TMD can be more effectively managed with neuromuscular re-education as provided by the Rocabado protocol.
Statistical significance was evident in all post-treatment comparisons using two-sample t-tests (P < .05), favouring the Rocabado group. The within-group analyses using paired t-tests also confirmed significant improvements for both interventions (P < .001), validating the effectiveness of both therapies. The statistical analysis further reinforced that although both techniques work, Rocabado’s structured rehabilitative exercises deliver more consistent and pronounced results. The therapeutic rationale behind MET lies in its ability to restore musculoskeletal function through autogenic or reciprocal inhibition, effectively lengthening shortened muscles and improving joint mobility. MET is particularly beneficial in addressing muscle tightness and joint stiffness in the TM region. However, its focus is predominantly on the soft tissues and lacks a comprehensive neuromuscular retraining component, which might explain the comparatively lesser improvement noted.
Rocabado’s protocol, on the other hand, incorporates a ‘six-by-six’ routine, which includes exercises such as controlled tongue positioning, nasal breathing and controlled mandibular movements. These exercises not only address muscular and articular components but also focus on postural re-education, which plays a crucial role in reducing recurrence and improving long-term outcomes. According to Rocabado et al. postural alignment is critical for optimal TM joint function and their six exercises are designed to simultaneously address factors.[13]
The outcomes of this research are consistent with previous studies. Clark et al. reported that postural correction strategies, including the Rocabado approach, lead to a significant reduction in TMD symptoms within six weeks.[14] Similarly, research by Kothari et al. emphasised the role of combined postural and mandibular exercises in improving functional scores in TMD patients.[15]
Further validate the superiority of Rocabado exercises in reducing pain, improving mobility and enhancing jaw function. Despite these positive findings, this study is not without limitations. The sample size was limited to 30 participants, which might affect the generalisability of the results. Additionally, the short duration of intervention and lack of long-term follow-up restrict our understanding of the sustainability of the therapeutic outcomes.
Despite these promising findings, the study has limitations. The sample size was limited to 30 participants, which may affect the generalisability of the results. The short duration of intervention and absence of long-term follow-up restrict conclusions regarding the sustainability of therapeutic benefits. Additionally, the lack of a placebo or control group prevents comparison with natural recovery. Although participant blinding was maintained, the absence of assessor blinding may introduce bias. Final, reliance on clinical and subjective outcome measures could be strengthened in future studies by incorporating objective assessments such as imaging or biomechanical analysis.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Approval was obtained from the local ethics committee (Approval No: APC-IEC/2023/Physio/015). The research was conducted in accordance with the Declaration of Helsinki.
Informed consent
Signed consent forms from all the participants were taken.
Credit author statement
Dr Gaurav Patel, Dr Pooja Vora, Rajesh Botchu: Conception and design or acquisition of data or analysis and interpretation of data.
Dr Gaurav Patel, Dr Pooja Vora, Ms Ridhdhi Panchal, Ms Riya Jani: Design or acquisition of data or analysis and interpretation of data.
Dr Gaurav Patel, Dr Pooja Vora, Ms Ridhdhi Panchal, Ms Riya Jani, Yogesh Parmar, Rajesh Botchu: Drafting the article or revising it critically for important intellectual content.
Dr Gaurav Patel, Dr Pooja Vora, Ms Ridhdhi Panchal, Ms Riya Jani, Yogesh Parmar, Rajesh Botchu: Final approval of the version to be published.
Informed consent
Signed consent form were taken from all the participants.
Data availability
Data is available to share on request.
Use of artificial intelligence
No AI was used.