
Abstract
Objectives:
This study aimed to analyse the demographic profile, associated factors, treatment approaches, and outcomes of patients with Bell’s palsy (BP), and to compare the therapeutic efficacy of steroid monotherapy against combined steroid-antiviral therapy.
Methods:
Following approval from the institutional ethics committee, this retrospective analysis was carried out in the Department of Otolaryngology between January 2021 and January 2024. Data from 120 patients diagnosed with BP were reviewed. Group 1 (n = 69) received corticosteroids alone, whereas Group 2 (n = 51) received a combination of systemic corticosteroids and antiviral medication. Each group was further subdivided based on the time of treatment initiation—within 72 hours or after 72 hours of symptom onset. All patients were assessed before and after therapy using the House–Brackmann grading system.
Results:
No significant association was found between prognosis and either age or sex. Initiation of treatment within three days of onset was linked to better recovery. Patients treated with a steroid-antiviral combination demonstrated superior outcomes compared to those receiving steroid monotherapy.
Conclusion:
BP is an acute idiopathic lower motor neuron facial paralysis. Early initiation of combined corticosteroid and antiviral therapy, preferably within 72 hours of onset, is associated with improved recovery outcomes.
Keywords
Background
Bell’s palsy (BP) is the predominant cause of acute peripheral facial nerve paralysis and represents the most frequent cranial mononeuropathy. It is characterised by sudden, unilateral weakness or paralysis of the facial muscles due to dysfunction of the seventh cranial nerve. BP accounts for nearly 60%–75% of all cases of acute unilateral facial paralysis.[1]
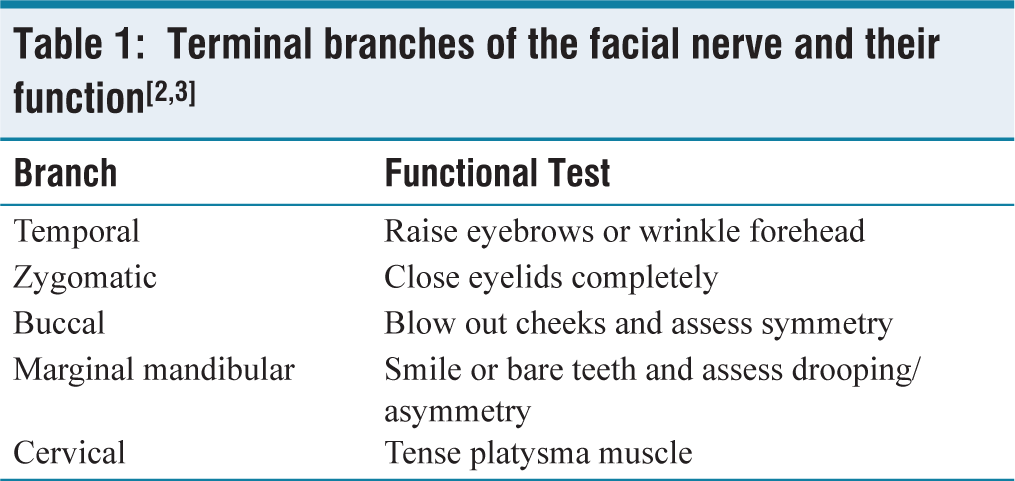
Facial paralysis may be classified as either supranuclear or infranuclear. The neurons innervating the lower face receive upper motor neuron (UMN) input from the contralateral cerebral cortex, while those supplying the upper face receive bilateral cortical input. Consequently, supranuclear (UMN) lesions lead to weakness of the lower facial muscles with forehead sparing. In contrast, infranuclear (lower motor neuron [LMN]) lesions result in paralysis of all muscles of facial expression on the affected side. Depending on the level of nerve involvement [Table 1], patients may present with an unfurrowed forehead, incomplete eye closure, and additional symptoms such as loss of taste or hyperacusis.[2]
Terminal branches of the facial nerve and their function[2,3]
Facial nerve palsy can be either congenital or acquired. Congenital cases may arise from genetic or developmental anomalies, while acquired causes include infectious, inflammatory, traumatic, vascular, or neoplastic conditions. Among acquired forms, idiopathic facial paralysis—BP—remains the most common.[3–5] Notably, the majority of cases of acute facial weakness are attributable to stroke or BP.[6]
The House–Brackmann (HB) grading system and Sunnybrook Facial Grading Scale are widely employed to assess the severity of facial dysfunction.[7,8] Although BP is the most frequent facial palsy encountered in clinical practice, its aetiology remains unclear. The Guideline Development Group (GDG) advises that the diagnosis of BP should be made only after excluding other potential causes of facial paralysis.[9]
This study, therefore, aimed to describe the demographic characteristics, associated conditions, therapeutic interventions, and recovery outcomes in patients diagnosed with BP.
Methods
Study Design and Setting
Following ethical approval from the institutional review board, this retrospective study was conducted in the Department of Otolaryngology and Head & Neck Surgery between January 2021 and January 2024.
Study Population
A total of 120 patients diagnosed with idiopathic facial nerve palsy were included. Participants were divided into two treatment groups:
Group 1 (n = 69): received corticosteroids alone.
Group 2 (n = 51): received combined corticosteroid and antiviral therapy.
Each group was further stratified based on the timing of treatment initiation—within 72 hours or after 72 hours from the onset of facial weakness.
Clinical Assessment
Diagnosis of facial palsy was primarily clinical. Patients underwent a focused neurological examination, including:
Observation of forehead wrinkling, Eye closure, Cheek inflation, Display of teeth, and Eversion of the lower lip.
Individuals with suspected central lesions were referred to the Department of Medicine, whereas those with peripheral involvement were evaluated for the integrity of each terminal facial nerve branch.
Investigations: Patients with peripheral facial palsy underwent additional investigations to exclude secondary causes. Laboratory tests were performed to rule out infectious or inflammatory aetiologies. High-resolution computed tomography (HRCT) of the temporal bone was done for patients with a trauma history to exclude fractures. Magnetic resonance imaging (MRI) was used to identify possible compressive or structural lesions along the facial nerve pathway.
Inclusion Criteria
Patients presenting with idiopathic (unknown-cause) peripheral facial palsy were included.
Exclusion Criteria
Patients were excluded if facial palsy was associated with: Identified infectious, vascular, or neoplastic causes, central nervous system pathology, or temporal bone disease.
Clinical Evaluation and Data Collection
Comprehensive clinical history and neurological examination were performed for each patient. Data were collected regarding demographics, comorbidities, presenting features, duration and chronology of symptoms, treatment type and timing, and recovery status.
Facial Nerve Function Grading
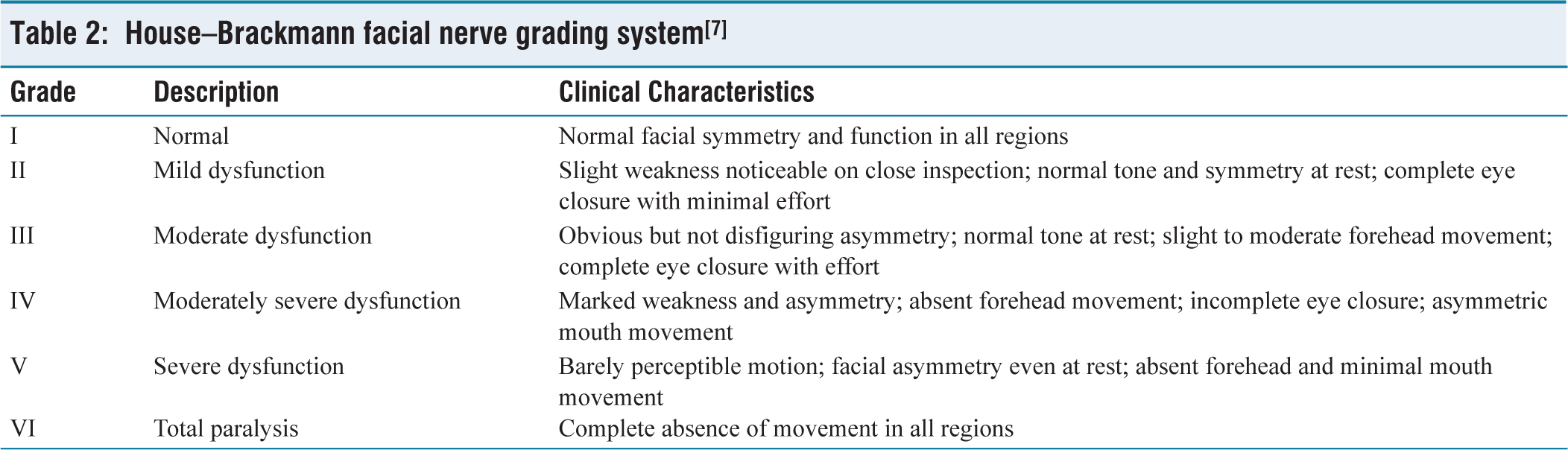
Facial function was assessed using the HB facial nerve grading system, a six-point scale ranging from Grade I (normal) to Grade VI (total paralysis), as shown in Table 2.[7] Grading was performed at presentation and at follow-up assessments.
House–Brackmann facial nerve grading system[ 7 ]
Treatment Protocol
Participants were randomly assigned using a simple randomisation technique.
Group 1 received systemic corticosteroids alone, while Group 2 received a combination of corticosteroids and antiviral medication (Acyclovir).
Both groups were further divided based on whether therapy was initiated within or beyond 72 hours of symptom onset.
Follow-up and Outcome Measurement
All patients were followed up for three months after initiation of treatment. Facial nerve recovery was evaluated at each visit using the HB grading system.
Statistical Analysis
Data were tabulated in Microsoft Excel and analysed using appropriate statistical tests. Categorical variables were expressed as frequencies and percentages, and analysed using Chi-square or Fisher’s exact test. Continuous variables were presented as means ± standard deviation and compared using the two-sample t-test. A P < .05 was considered statistically significant.
Results
Demographic Characteristics
Among the 120 patients included, 69 received corticosteroid monotherapy (Group 1) and 51 received combined corticosteroid-antiviral therapy (Group 2).
In Group 1, the largest proportion of patients (approximately 78%) were aged between 20 and 40 years, with a mean age of 29.0 ± 9.1 years. Females constituted 62.3% (n = 43), while 37.7% (n = 26) were males, giving a male-to-female ratio of 1:1.6.
In Group 2, the majority also fell within the 20–40 year age range, with a mean age of 33.5 ± 8.1 years. Females accounted for 64.7% (n = 33) and males 35.3% (n = 18), yielding a male-to-female ratio of 1:1.8.
Although BP was observed more frequently among females, there was no statistically significant difference between the two groups regarding age (P = .41) or gender (P = .44). The highest incidence was noted in the 18–30 year age group.
Comorbid Conditions
In Group 1, 19 patients (27.5%) had one or more comorbidities, including diabetes mellitus, hypertension, or dyslipidaemia. In Group 2, 11 patients (21.4%) exhibited similar comorbidities.
There were no statistically significant differences in recovery outcomes between:
Groups 1 and 2 (P = .23). Patients with and without comorbidities (P = .41 and P = .10, respectively).
Treatment Timing and Recovery
The effect of treatment timing on recovery was assessed within each therapeutic group.
Steroid Monotherapy (Group 1):
Of the 69 patients, 53 (78.5%) began treatment within 72 hours of onset. These individuals achieved a mean HB score of 2.35 ± 0.11, compared with 16 patients (23.1%) who started therapy after 72 hours and had a mean HB score of 3.01 ± 0.20.
The difference between the early and delayed treatment subgroups was statistically significant (P = .04).
Combination Therapy (Group 2):
Among 51 patients, 42 (82.3%) initiated treatment within 3 days, showing a mean HB score of 1.61 ± 0.11 after 2 months, whereas 9 (17.7%) began treatment after 3 days, with a mean score of 1.56 ± 0.23.
Although the earlier treatment group demonstrated better improvement, the difference was not statistically significant (P = .40).
Comparison between both therapeutic approaches revealed superior HB scores in Group 2 (combined therapy), with a significant difference (P < .005). Likewise, early initiation of therapy, regardless of regimen, produced significantly better outcomes (P < .05).
Overall Recovery
At the 2-month follow-up, the mean HB grade was 1.64 ± 0.51 for patients in Group 1 and 1.28 ± 0.40 for Group 2. Although Group 2 exhibited a trend toward improved outcomes, the intergroup difference did not reach statistical significance (P = .09).
Discussion
The aetiology of BP remains uncertain, though viral reactivation has been widely proposed. Evidence suggests that herpes simplex virus (HSV) reactivation within the geniculate ganglion may trigger inflammation and oedema of the facial nerve, leading to compression within the fallopian canal.[10] Viral DNA has been identified in the facial nerve and posterior auricular muscle of affected patients.[11] However, HSV DNA has also been detected in individuals without any clinical history of facial paralysis, implying that viral presence alone does not fully explain the disease mechanism.[12]
Professional societies, including the American Academy of Neurology (AAN) and the American Academy of Otolaryngology-Head and Neck Surgery Foundation (AAO-HNSF), emphasise corticosteroids as the cornerstone of treatment. These guidelines advocate oral steroid therapy within 72 hours of onset, typically prednisone 50–60 mg daily, followed by tapering.[13] Routine antiviral monotherapy is not recommended, although combined antiviral-steroid therapy may be beneficial in selected cases.[14–16] The theoretical rationale for antivirals lies in the potential role of HSV-1 and zoster sine herpete (herpes zoster reactivation without rash).[17]
Demographic Patterns
In this study, BP was more frequent among females and young adults aged 18–30 years, aligning with existing epidemiological reports. The lack of statistical significance between age and gender and disease prognosis concurs with prior findings by Flifel et al., who observed no correlation between recovery outcomes and these demographic factors.[18] Similarly, studies by Takashi et al. and Happe et al. found age and sex to have minimal prognostic influence.[19–21] In contrast, Ikeda et al. suggested that advanced age and male gender might adversely affect recovery.[22]
Comorbidities
The current findings revealed no significant relationship between recovery and the presence of diabetes, hypertension, or dyslipidaemia, paralleling earlier reports.[22–25] Kudoh et al. similarly observed no direct association between BP and diabetes or hypertension, although patients with both conditions tended to recover more slowly.[26]
Associated Features
In our cohort, approximately 40% of patients experienced otalgia or post-auricular pain, frequently during colder weather, suggesting a seasonal association. Mustafa et al. also noted post-auricular pain in around 50% of their patients,[27] while Pietersen et al. found this symptom correlated with poorer prognosis.[28] Katusic et al. further demonstrated that non-auricular pain was linked to delayed recovery.[29]
Taste disturbances were not commonly reported in our series, differing from earlier studies by Mustafa et al. and El-Ebiary et al., who documented taste alteration in 13%–14% of cases.[30,31] Pietersen et al. observed a much higher incidence (83%), implying potential geographical or methodological differences.[28]
While some earlier authors postulated that cold exposure predisposes individuals to BP, others, including Danielides et al., refuted this ‘refrigeration theory’, reporting no significant link between low temperature and disease onset.[31]
Recovery and Prognostic Factors
After two months, patients receiving combined corticosteroid-antiviral therapy showed better functional recovery (mean HB grade 1.28) than those treated with steroids alone (mean HB grade 1.64). Although the difference was not statistically significant, this trend aligns with results from Engström et al., who demonstrated that higher HB grades at presentation predict poorer prognosis.[32] Similarly, Gordana et al. reported that incomplete paralysis at onset typically recovers fully, whereas complete paralysis is associated with residual weakness.[33]
The present study found that early treatment initiation—within 72 hours—was associated with more favourable outcomes, consistent with multiple prior trials.[34,35] For instance, Hato et al. documented a 100% recovery rate when combined therapy was initiated within three days, compared with 86.2% for delayed treatment.[35] Yeo et al. also reported better outcomes in early-treated cases, although the difference was not statistically significant.[35] Conversely, Flifel et al. did not observe a significant effect of early initiation on recovery.[18]
The therapeutic advantage of antivirals may be attributed to their mechanism of action, wherein acyclovir inhibits HSV DNA polymerase, preventing viral replication.[36,37] Studies evaluating valacyclovir in combination with corticosteroids have reported recovery rates exceeding 96%, compared to approximately 89% with steroids alone.[34]
However, not all research supports the additional use of antivirals. Sullivan et al. found no significant improvement when acyclovir was combined with prednisolone.[38] Yet, subsequent Cochrane reviews indicated that combined treatment modestly reduces long-term sequelae compared with corticosteroids alone.[39–41]
Conclusion
This study highlights that BP is an acute, idiopathic, LMN facial paralysis with no statistically significant association with age or gender. The findings reinforce that early intervention, particularly within 72 hours of symptom onset, leads to improved recovery outcomes. The combination of corticosteroids and antiviral agents produced superior recovery trends compared to steroid monotherapy, suggesting that antivirals play a supportive role in treatment when initiated promptly. Although the present work was retrospective and based on a single-centre experience with a limited sample size, its results align with the growing consensus that combined therapy, when started early, can enhance functional recovery and minimise residual deficits. Predictors of incomplete recovery include severe paralysis at presentation, delayed treatment initiation, slow onset of improvement, and persistent pain. Further prospective multicentric studies with larger cohorts are recommended to consolidate these findings and establish a unified treatment protocol for BP.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Approval was obtained from the ethics committee of SKIMS MCH. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Informed consent
Written informed consent was obtained from all participants prior to inclusion in the study.
Credit author statement
All authors contributed to the study’s conception and design.
Material preparation, data analysis and the first draft of the manuscript were prepared by FD.
BM helped in data collection.
MM helped with data analysis.
AW supervised and commented on previous versions of the manuscript.
All authors read and approved the final manuscript.
Data availability
The datasets during and/or analysed during the current study are available from the corresponding author upon reasonable request.
Use of artificial intelligence
No use of artificial intelligence.