
Abstract
Synovial chondromatosis (SC) is a rare, benign neoplastic process involving multiple hyaline cartilaginous nodules in the subsynovial tissue of a joint, tendon sheath or bursa. Primary intraarticular SC (PISC) is an idiopathic and largely monoarticular, involving large joints. Most cases occur at the knee, then the hip, elbow, shoulder and ankle. PISC is rare in the foot.
We present the case of a 38-year-old male with a three-year history of indolent and progressive unilateral right foot swelling and pain with PISC of the right calcaneocuboid joint (CCJ) and review the literature.
A literature review revealed one case of PISC of the CCJ that did not describe radiological features and one case of PISC of the subtalar joint that extended into CCJ.
Introduction
Synovial chondromatosis (SC) is a rare benign proliferative process causing multiple subsynovial hyaline cartilaginous nodules in joints, tendon sheaths and bursae.[1-5] These nodules can enlarge or detach, forming loose cartilaginous or calcified bodies.[5,6] SC is typically self-limited, but may recur; locally malignant transformation is extremely rare.[4,6–8]
First described in 1813, SC has been previously termed synovial osteochondromatosis (reflecting the ossification of the chondral nodules) amongst other terms.[3,4,6,9] Radiologically, distinguishing primary and secondary subtypes and intraarticular and extraarticular origins is most important.[5]
Primary intraarticular SC (PISC ) is an idiopathic condition involving cartilage metaplasia that, over time, can result in articular erosion and mimic osteoarthritis symptoms.[5,10] Secondary SC is more common, resulting from mechanical irritation due to underlying conditions such as osteoarthritis, trauma, rheumatoid arthritis, osteonecrosis, osteochondritis dissecans, neuropathic osteoarthropathy and prior infection or inflammatory arthritis.[3,4,6] It typically affects older patients and is characterised by joint pain and restricted motion.[4,11] The two entities can be distinguished radiologically and pathologically, with secondary SC exhibiting underlying articular disease, fewer and larger chondral bodies of varying size and shape and concentric growth rings on histopathology, suggesting various times of origin.[3–5]
Intra-articular SC is more frequent than extra-articular, the latter affecting bursae or tendon sheaths.[4,6] Most cases are monoarticular and involve large joints, predominantly the knee (in 50%–65% of cases).[4,6,9] Occurrence in smaller joints, including the foot, is exceedingly rare.[3,4,11] The incidence of PISC is about one in 100,000, with the average age range of 20–40 years, twice as common in men.[4–6] Extra-articular SC typically occurs in women over 50 and often affects smaller joints, especially the hands.[4]
This article is the first to describe PISC in the calcaneocuboid joint (CCJ). We present a detailed literature review and discuss the importance of recognising the clinical, radiologic and pathologic features of SC.
Case Report
A 38-year-old male presented with a three-year progressive and indolent history of unilateral right foot swelling, reduced range of motion and pain exacerbated by exercise. There were no signs of malignancy and no contralateral foot issues.
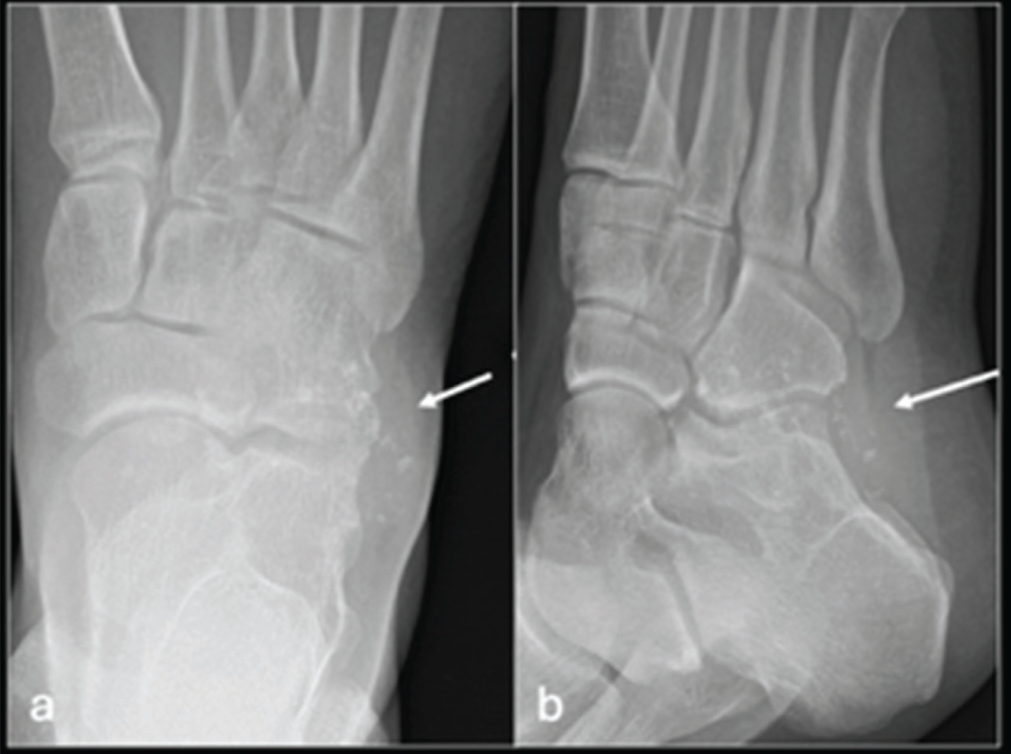
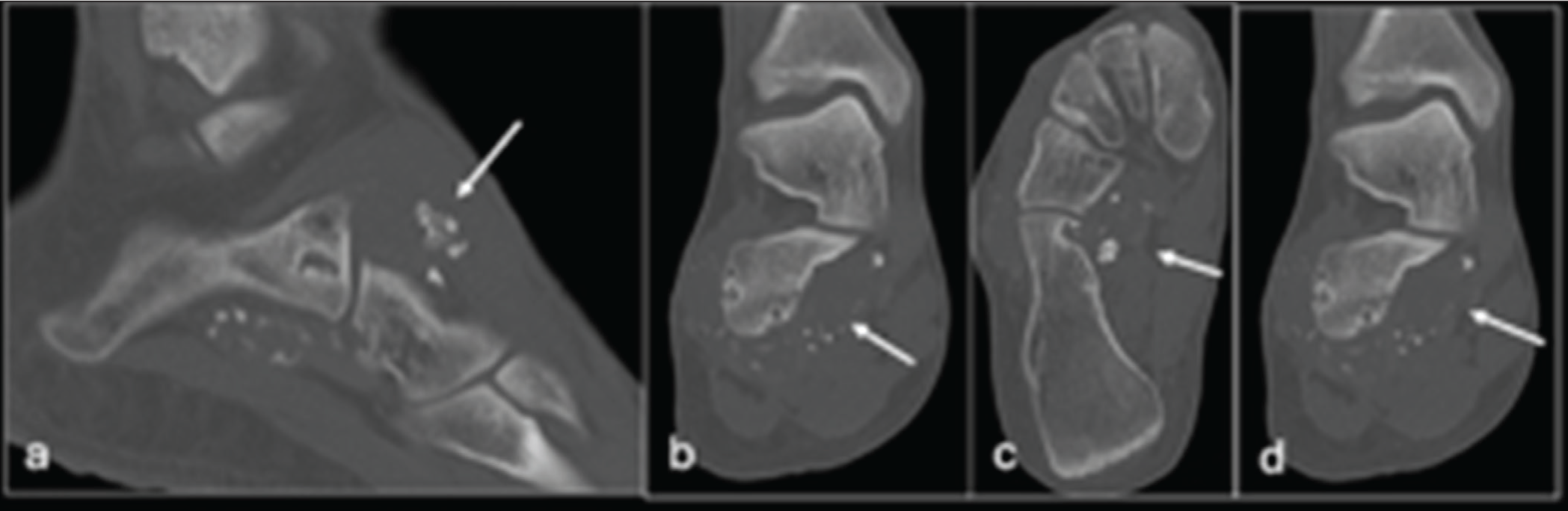
Initial radiographs of the right foot demonstrated soft tissue swelling with small volume calcification at the right CCJ, causing scalloping [Figure 1]. Computed tomography (CT) depicted homogenously-sized nodules (2–3 mm) with ‘ring-and-arc’ chondroid mineralisation within a well-defined area of hypoattenuation at the CCJ [Figure 2]. Some calcified nodules demonstrated endochondral ossification with peripheral cortication and internal hypoattenuation [Figure 2]. Lobulated outer contours were atypical of a joint effusion [Figure 2]. Local well-defined bone erosion was also seen on both sides of the joint [Figure 2b-d]. The joint space was otherwise preserved.
Magnetic resonance imaging (MRI) [Figure 3] showed non-mineralised components with high water content (hyperintense at T2-weighted imaging / short tau inversion recovery, STIR), correlating with the hypoattenuating areas on CT. Homogeneous T2-hypointense calcified intra-articular nodules correlated with very hyperattenuated foci at prior CT [Figure 3]. MRI demonstrated more non-calcified (T2 iso- to slightly hypo-intense) intra-articular nodules compared to CT [Figure 3]. The nodules were of a similar size and shape [Figure 3]. MRI demonstrated mild osseous oedema adjacent to the juxta-articular joint erosion [Figure 3]. There was no radiologic evidence of marrow invasion, true cortical destruction or periosteal reaction.

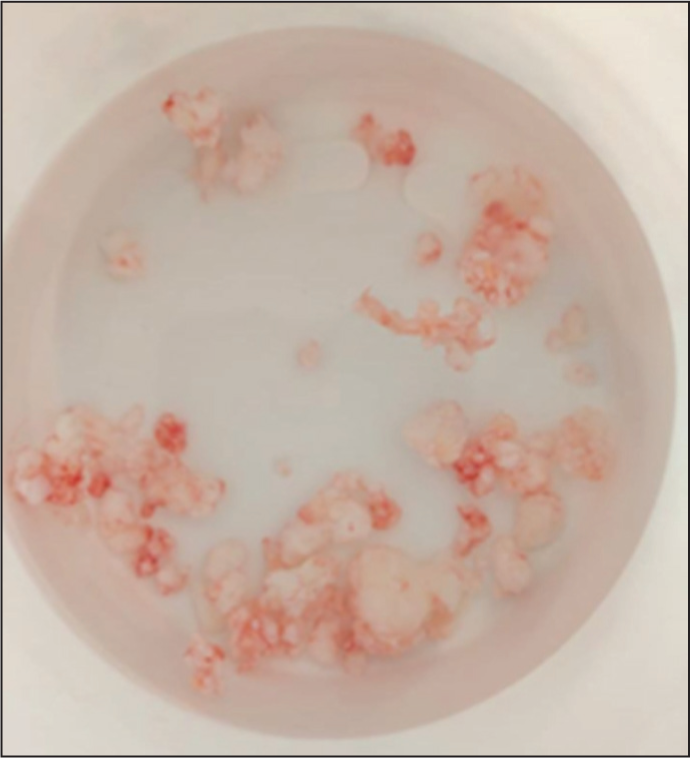
After clinical evaluation and multidisciplinary team discussion, PISC of the CCJ was diagnosed radiologically despite the atypical site. The patient opted for open synovectomy, resulting in symptom resolution. Gross histopathologic analysis demonstrated a cobblestone appearance due to synovial hypertrophy and multiple, similar-sized, multilobulated cartilaginous nodules, some of which ossified and detached from the synovium [Figure 4]. Microscopic histopathologic analysis was consistent with primary SC and there was no malignant transformation. At the six-month post-operative review, the patient remains asymptomatic and has returned to long-distance hiking.
Discussion
Foot involvement in PISC is rare. Of 652 recorded cases of SC at our specialist oncologic orthopaedic referral centre, only six (0.9%) cases occurred in the ankle or foot. Specifically, four were at the ankle and one at the first metatarsophalangeal joint, with the final one being the presented case at the CCJ. Literature review reveals only one previously mentioned case at the CCJ and another at the subtalar joint that extended into the CCJ.[1,2] The presented case represents the first detailed report of PISC.
Diagnostic Features of SC
Diagnosis of SC combines clinical, radiological and (if required) histopathological assessments.[6] Typically, articular erosion presents with progressive pain, swelling and restricted movement.[4,5,10,12–14] Clinical signs include joint swelling, tenderness, crepitus and muscle atrophy.[4,12–14] However, extra-articular SC usually presents with a painless mass or mild tenderness.[4,12–14]
Radiography is normal in 5%–30% of cases, but can show pathognomic, similar-sized intra-articular calcifications, implying synchronous origin.[3,4,6,9,15] The nodules demonstrate ‘ring-and-arc’ or punctate chondroid mineralisation, which increases in number and size over time.[4]
Radiographically occult cases can be seen on CT as calcified chondral bodies and local extrinsic bone joint erosion.[4,9] Further features, such as bursal extension and non-calculated components, further benefit from MRI, although[4,16] variability is greater than CT, with 77% of cases showing non-mineralised cartilage components.[4,17]
The Milgram classification radiologically details SC progression.[4,15,17] Phase 1 (approximately 20% of cases) features intrasynovial chondroid metaplasia and active synovitis without chondral fragments or calcification.[4,15,17] Phase 2 (33%–77%) shows transitional lesions with active intrasynovial proliferation and variably-calcified chondral nodules and fragments.[4,17] Calcification causes hyperattenuation on CT and hypointensity on all MRI pulse sequences with blooming artefact.[4,17] Phase 3 (around 40%) demonstrates multiple loose calcified bodies, which can amalgamate, but synovitis will have resolved.[4,15] Endochondral ossification occurs over time, radiographically showing a targetoid appearance with a solitary peripheral calcified rim and central focal trabecular bone.[3,4,17] Although radiographically useful, there is minimal bearing on treatment from these three phases.[4,15]
As in our case, bony erosion in PISC is usually on both sides of the joint and due to mechanical pressure, particularly in less capacious joints.[4] Although extrinsic erosion can be deep, true marrow invasion is not a feature of SC and its presence signifies malignancy.[4,7]
Although not necessary for diagnosis, as in this case, other imaging methods can be used. If contrast administration is performed, enhancement involves the peripheral vascularised synovium and internal septae around non-enhancing hyaline cartilage nodules.[4] Ultrasound shows a heterogeneous mass containing hyperechoic foci representing chondral fragments with mobility of loose bodies and acoustic shadowing from calcifications.[4] Bone scintigraphy shows radionucleotide uptake, reflecting increased osteoblastic activity.[4,13] Similarly, low-level fluorodeoxyglucose avidity on positron emission tomography/CT.[18]
Gross histopathology reveals a ‘cobblestone’ appearance due to synovial hypertrophy and multilobulated cartilaginous nodules, which can detach and lie in intrasynovial and extrasynovial soft tissues and cause bony erosion.[4] Ossification is present in 45% of cases.[4,8] Histopathologically, extra-articular SC is indistinguishable from intra-articular SC.[4] Microscopy shows subsynovial cartilage neoplasia with lobules of hyaline cartilage surrounded by synovium with varying degrees of hyperplasia.[4] Compared to normal cartilage, SC shows a greater density of chondrocytes haphazardly arranged in clusters or sheets within a hyaline matrix.[6,9]
Differential Diagnoses
Differential diagnoses of PISC include trauma, neoplastic and inflammatory conditions.[3–5,19] Neoplastic conditions mimicking PISC include secondary SC, osteochondroma, soft tissue chondroma, synovial chondrosarcoma and intra-osseous low-grade chondrosarcoma with joint extension.[3–5,19] Inflammatory joint diseases mimicking PISC include crystal arthropathies, rheumatoid arthritis, infection, tuberculosis and synovial proliferative disorders.[3–5,19]
Malignant transformation into synovial chondrosarcoma is rare and involves 5% of SC cases, typically those with long-standing disease and frequent recurrences.[4,8] Key distinguishing features include the clinical course with chondrosarcoma showing rapidly increasing lesion size.[4,7,8] Most synovial chondrosarcomas are low-grade lesions, with 20% being grade 1% and 70% being grade 2 chondrosarcomas.[4,7,8] Distinguishing chondrosarcoma from SC is critical for appropriate treatment, as malignant transformation often necessitates amputation and is associated with a high risk of post-surgical mortality.[4,7,8] Distinguishing malignant histopathologic features of chondrosarcoma include bone invasion, marrow permeation, spindle cell proliferation and tumour necrosis as well as loss of the chondrocyte clustering seen in SC.[4,20]
However, histologic atypia means SC can easily be mistaken for chondrosarcoma, rendering imaging correlation important.[4] Radiology can also be challenging due to overlapping features. Malignant radiologic characteristics include marrow invasion and true cortical destruction, with or without an associated periosteal reaction, which is best assessed through a combination of CT and MRI imaging.[4,7] Lung metastasis is a definitive diagnostic indicator of malignancy.[4]
Conclusion
PISC is rare in the foot and extremely rare at the CCJ, with this being the first described instance in existing literature. Our review highlights the radiologic features of SC that can be pathognomonic, as well as differential diagnosis and management. We have emphasised the importance of considering PISC as a differential for calcification and soft tissue swelling at the CCJ and highlighted methods to distinguish it from other differential diagnoses, especially chondrosarcoma, to prevent mistreatment.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Not applicable
Informed consent
Informed consent obtained.
Credit author statement
All authors contributed to the article.
Data Availability
No data was used in this manuscript that requires citation.
Use of artificial intelligence
No AI was used.