
Abstract
Left ventricular (LV) pseudoaneurysm is a myocardial rupture that has been sealed by pericardium, organised thrombus and fibrosis. A pseudoaneurysm has a 40%–50% risk of progressing to a full rupture, and thus warrants urgent surgical suturing. We present here a case report of a 63 years female who presented with this rare complication of myocardial infarction (MI). About three weeks prior, she had acute coronary syndrome (ACS)-non-ST elevation myocardial infarction (NSTEMI) and had undergone percutaneous transluminal angioplasty (PTCA) with a drug stent to the left anterior descending artery (LAD), and now came with retrosternal chest pain and breathing difficulty. A 2-D Echocardiogram was done, which showed a pseudoaneurysm in the mid left ventricle (LV) at the postero-lateral wall, approximately 3 centimetres (cms) from the mitral annulus, with dimensions of 5 × 8 × 8 cms. Doppler showed bidirectional flow. She underwent a successful surgery for pseudoaneurysmal repair with excision and pledgeted suture application. This case highlights the diagnostic challenges in the emergency department when a patient presents with symptoms of heart failure, along with astute clinical management astute clinical assessment and utility of multiple imaging techniques for imaging for timely intervention in such cases.
Introduction
Left ventricular (LV) pseudoaneurysm (PA) is one of the most challenging complications of myocardial infarction (MI) involving tearing or rupture of the infarcted tissue. The clinical picture varies and depends on the site of rupture, which may involve the free wall of the ventricle, the interventricular septum, or the papillary muscles. The literature cites that the overall incidence of these complications has decreased owing to the introduction of reperfusion therapy and the widespread adoption of primary percutaneous coronary intervention (PCI).[1]
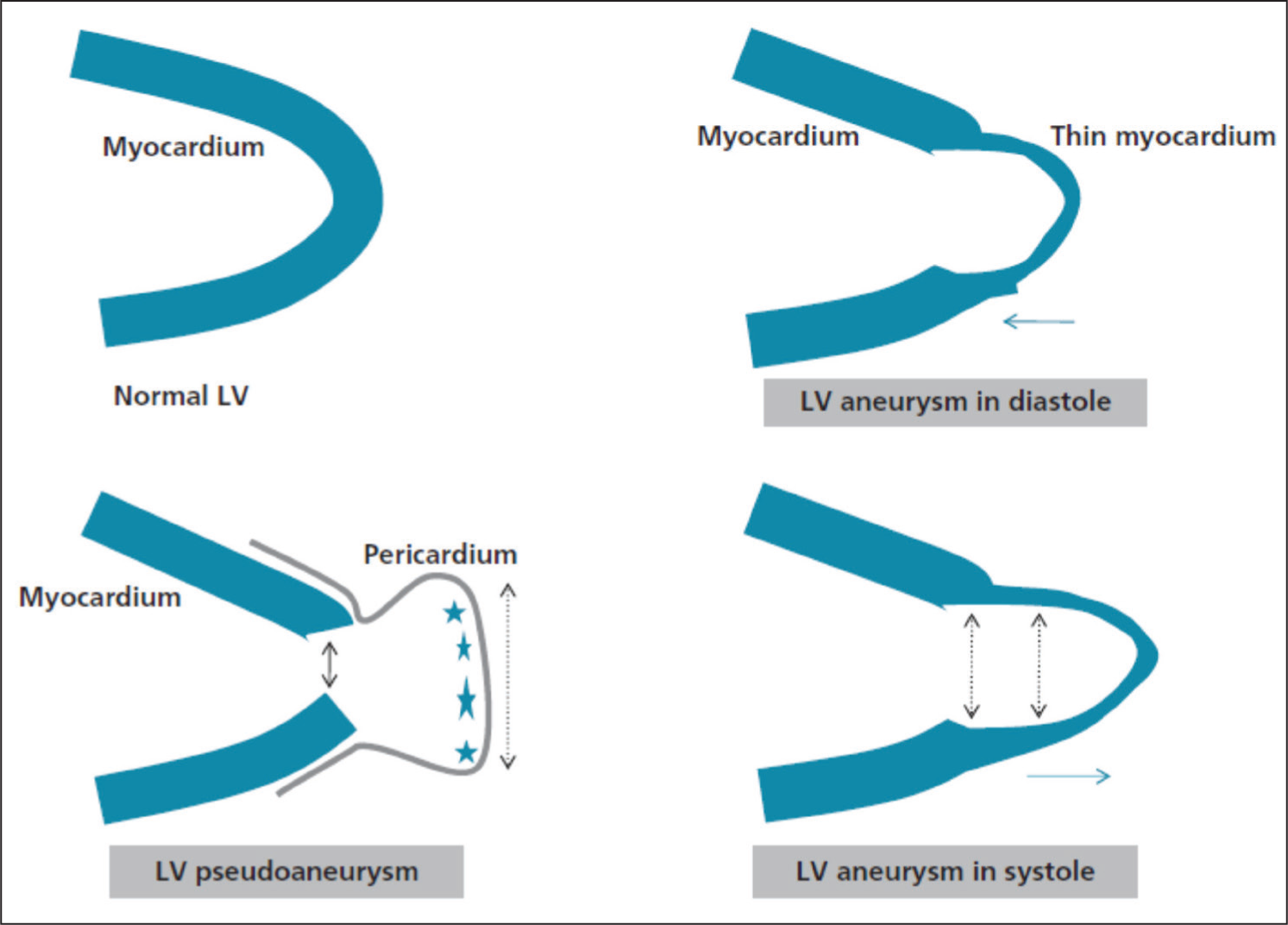
An LVPA is a ventricular free wall tear. Comparing with a true aneurysm, where there is thinning of myocardium but preservation of endocardium and epicardium, a pseudoaneurysm is defined as a disruption in all three layers of the heart, with the contents of the LV locally contained by adhesions and the adjacent pericardium [Figure 1].
A graphic representing the difference between a true aneurysm and a pseudoaneurysm
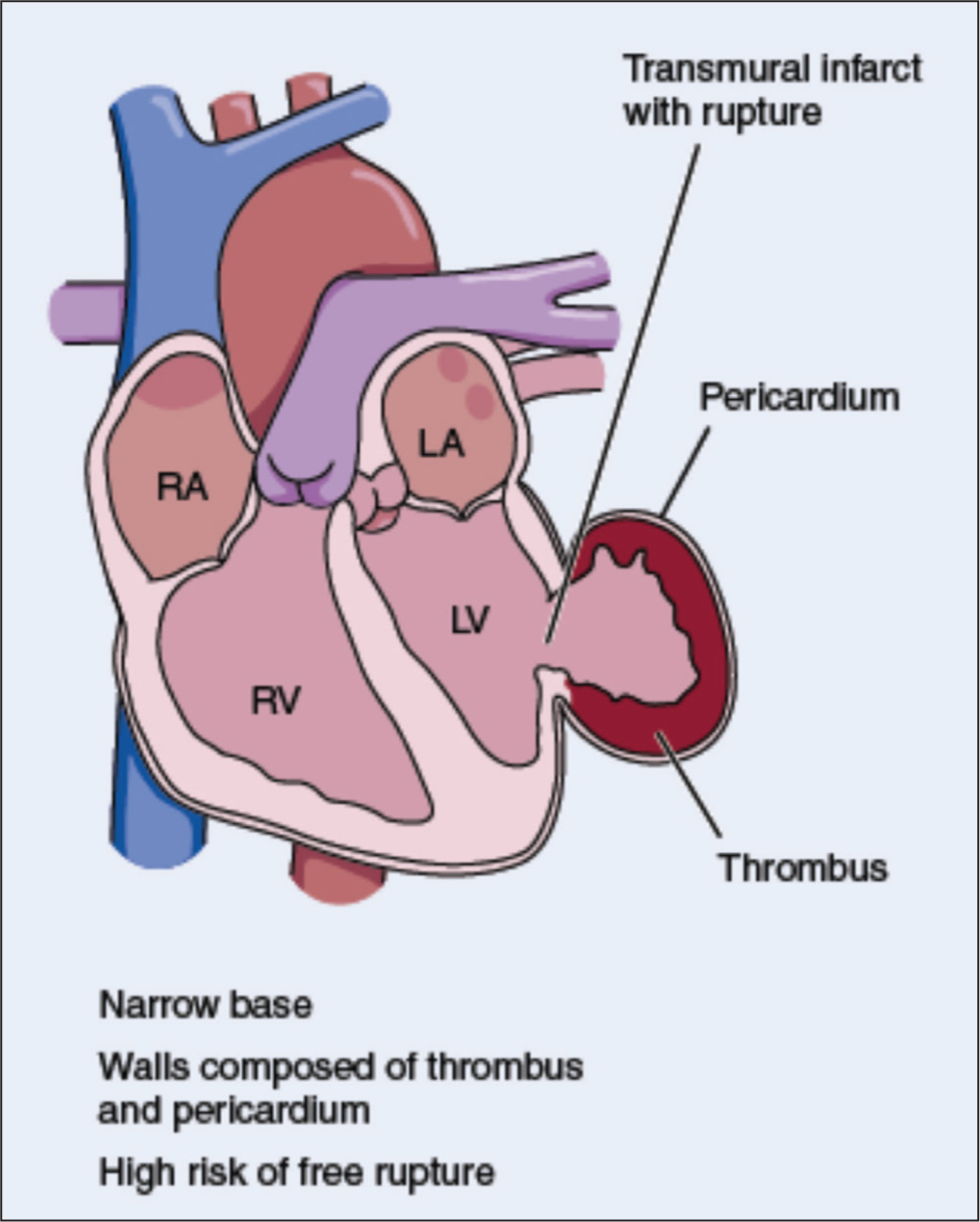
It is a rare mechanical complication of MI and heralds an unfavourable prognosis with a mortality rate of approximately 50% in most cases.[1] Pseudoaneurysms can become quite large and communicate with the LV cavity through a narrow neck [Figure 2]. Echocardiogram is the initial imaging modality of choice because it is readily available, non-invasive and can be done at the bedside. On echocardiography, these are visible as echo-free spaces adjacent to and continuous with the LV cavity. The most frequent site is the basal inferior or inferolateral wall, although they can also arise at the LV apex after anterior wall MI. The hallmark picture on echocardiography shows a narrow neck, less than 50% of the maximum diameter of the aneurysm itself, rough edges with an abrupt transition from normal to thinned walls, and turbulent bidirectional flow by Doppler. Alternatively, considering the hemodynamic stability of the patient, other investigations can be undertaken when there is doubt about the extent of the pseudoaneurysm. Such modalities of imaging are cardiac magnetic resonance imaging (cMRI), computed tomography (CT) or LV angiography.[2]
A graphic depicting a pseudoaneurysm of the LV
Clinical presentation may include features of congestive heart failure, angina, or ventricular arrhythmia. Pseudoaneurysms that occur a few days after acute MI are quite unstable and prone to rupture. The mean time to diagnosis of a pseudoaneurysm is generally in the range of a few weeks to 3 months after MI. Establishment of the diagnosis should be followed immediately by surgical treatment, which consists of direct closure or a pericardial patch.[3]
Pseudoaneurysms usually occur a few days after acute MI and are quite unstable and prone to rupture; however, in this case, it occurred after three weeks.
Clinical Presentation
A 63-year-old female presented with complaints of shortness of breath, New York Heart Association (NYHA) class III for 1 day and retrosternal pain, Canadian Cardiovascular Society (CCS) for angina class III for the past 3 days.
She had a significant past history of long-standing hypertension controlled on angiotensin II receptor blocker (ARB) and diabetes mellitus Type 2 on oral hypoglycaemic agents. Two years ago, she had an acute coronary syndrome (ACS)-non-ST elevation myocardial infarction (NSTEMI) for which she had undergone percutaneous transluminal coronary angioplasty (PTCA) with a drug-eluting stent to each left anterior descending artery (LAD) and right coronary artery (RCA).
About three weeks prior, she had an ACS-NSTEMI and had undergone PTCA with a drug stent to LAD, followed by dual antiplatelet drugs and high-dose statins.
At the time of this presentation, she was diaphoretic and tachypneic with a heart rate of 110 beats per minute with regular rhythm; blood pressure was 150/70 mmHg, and jugular venous pressure (JVP) was raised. Chest auscultation revealed bilateral rales; S1S2 were normal, S3 was heard, and no rub or added murmur was heard.
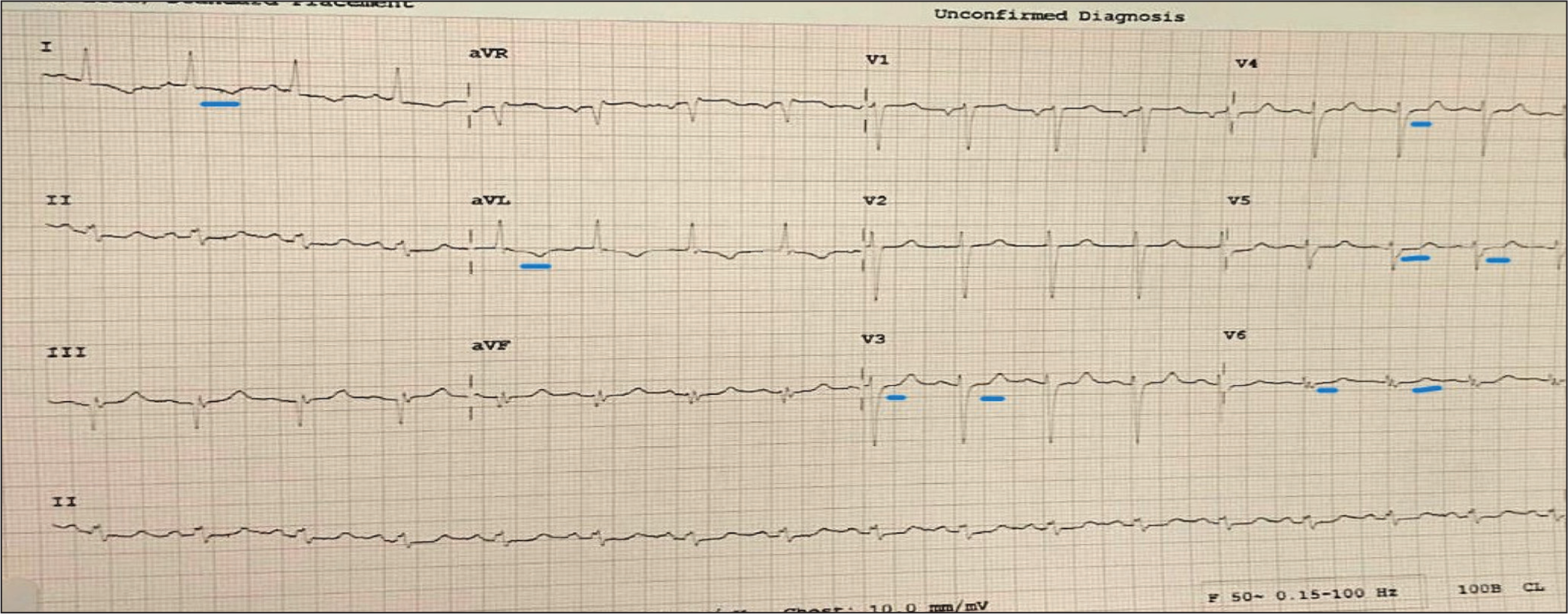
Electrocardiogram (ECG) showed sinus tachycardia with ST-depression in leads I, aVL and V3-V6 [Figure 3].
ECG showing sinus tachycardia with ST-depression in leads I, aVL and V3-V6 (blue lines)
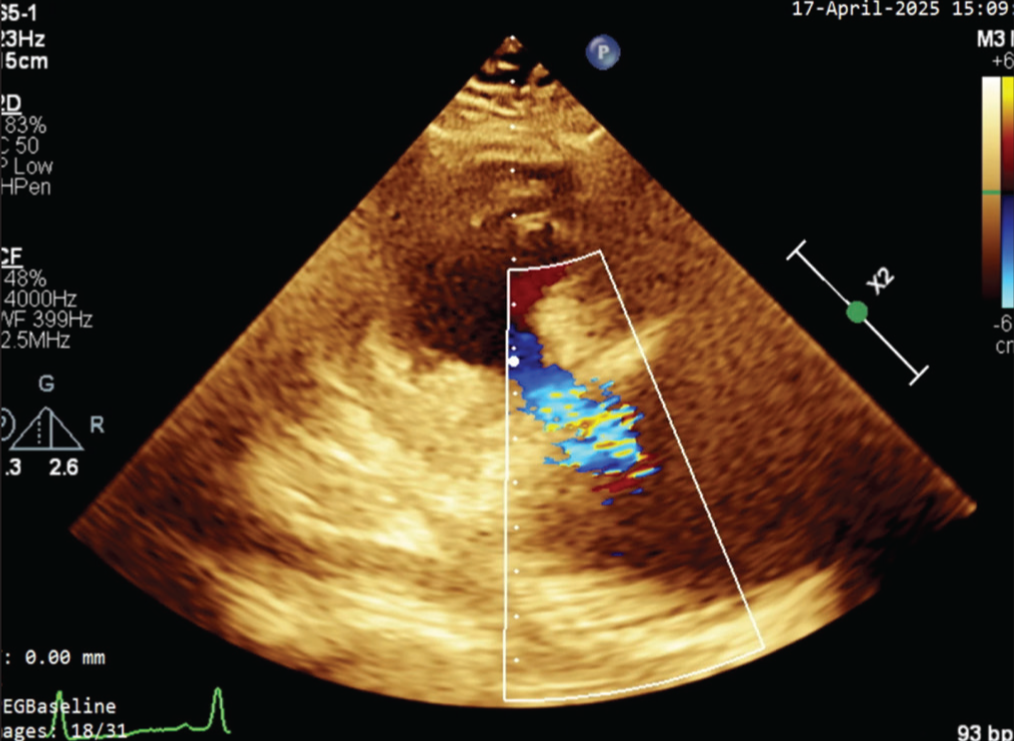
2-D Echocardiography was done, which showed a pseudoaneurysm in mid LV at the postero-lateral wall, approximately 3 cms from the mitral annulus with dimensions of 5 × 8 × 8 cms. Colour Doppler showed bidirectional flow. LV ejection fraction (LVEF) was 45%. Mild mitral regurgitation. Mild tricuspid regurgitation with pulmonary artery systolic pressure (PASP) of 45 mmHg. No intracardiac thrombus or pericardial effusion was noted [Figures 4–6].
Apical chamber view showing the outpouch with rent seen in the LV lateral wall having a narrow neck. Colour Doppler shows bidirectional turbulent flow
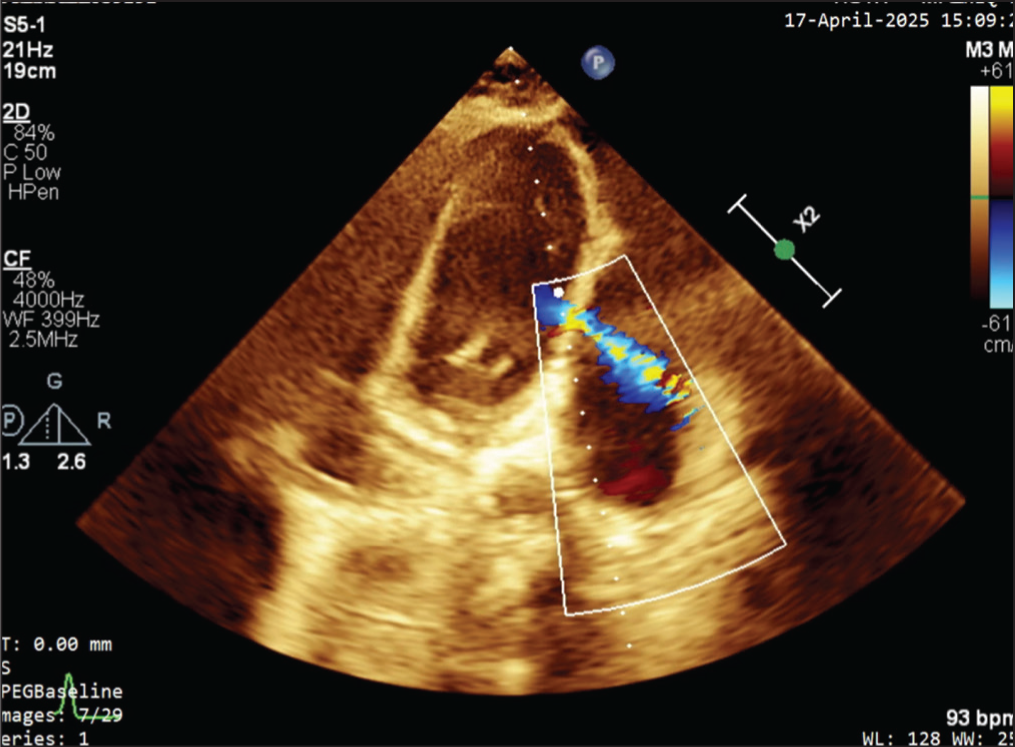
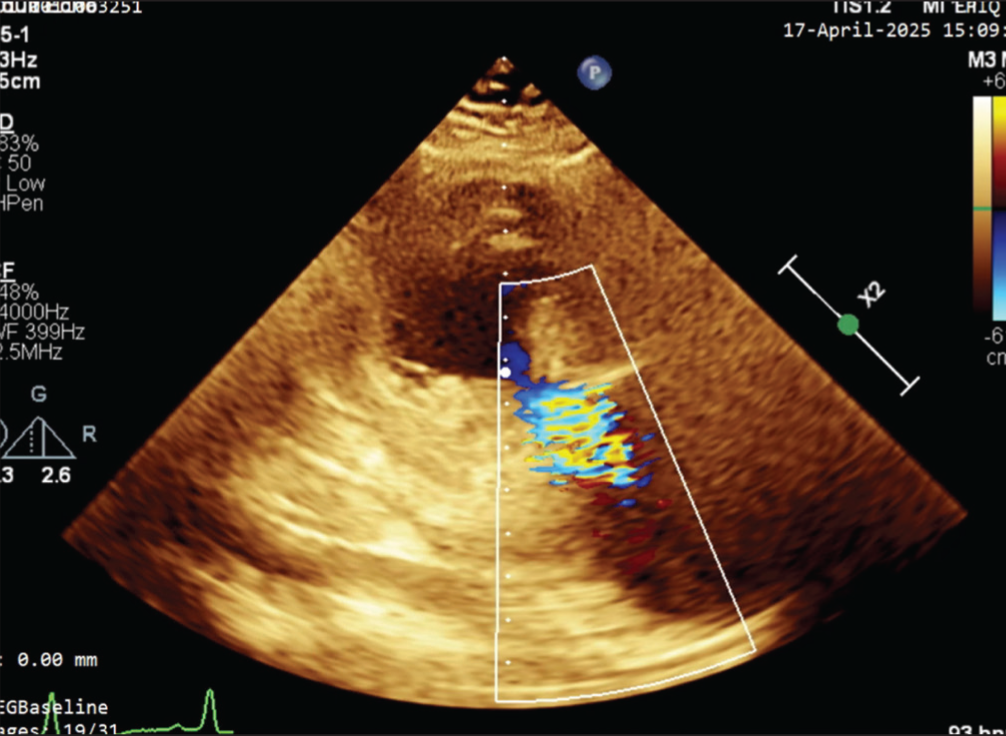
Short-axis view at papillary level, showing pseudoaneurysm. Colour Doppler shows bidirectional turbulent flow
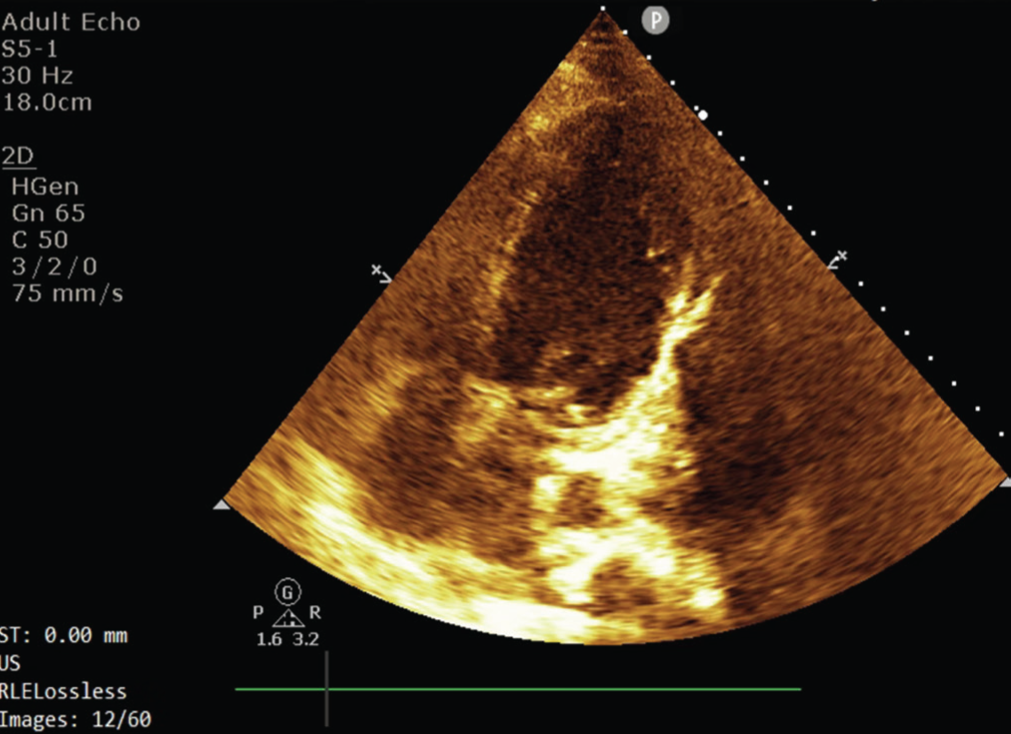
Short-axis view at mid LV level, showing pseudoaneurysm
Her other biochemical parameters (namely, complete blood count, kidney function tests) were within normal ranges.
After initial evaluation, she was treated with diuretics, antiplatelet drugs and other guideline-directed therapy. A coronary angiogram (CAG) was planned to assess and define the coronary anatomy. It revealed a patent stent in proximal LAD with a distal diffusely diseased vessel; left circumflex (LCx) was non-dominant and had 100% proximal chronic occlusion. RCA was the dominant vessel, and the proximal segment had a patent stent, whereas the mid-segment showed 60% tubular stenosis and 80% discrete stenosis just before the crux. The posterior descending artery (PDA) was normal, and the posterior left ventricular (PLV) artery was thin and narrow.
After a multidisciplinary team meeting and shared decision-making, the surgical option was preferred vis-à-vis transcatheter closure. She underwent successful surgery for pseudoaneurysmal repair with excision and pledgeted suture application. Post-procedure echocardiography revealed normal LV with no evidence of flow across the LV wall at the site of pseudoaneurysm [Figure 7]. Her peri- and postoperative course was uneventful. She remained in the critical care unit for three days with inotropes and anticoagulants. After seven days of an uneventful course in hospital, she was discharged in a stable condition.
Apical chamber view showing repaired LV lateral with no flow across it
The patient was educated about watchful monitoring of his condition and the importance of a regular follow-up with echocardiography.
Discussion
Mechanical complications after MI are rare in contemporary times, mostly due to advancements in reperfusion therapy. However, clinicians seldom encounter these in clinical practice, hence it is important to keep abreast with differential diagnoses, availability of newer imaging modalities and latest technologies of repair. One such complication of MI is a pseudoaneurysm. Pathologically, it is the sequelae of myocardial rupture with haemorrhage into the pericardial space, which then becomes locally compressive. Because of its poor structural integrity, it is at a high risk of spontaneous rupture, causing mortality [Figure 2].
The clinical presentation of LVPA is varied. In a couple of papers cited here, one systematic literature review found that 10% (n = 290) of cases were completely asymptomatic,[1] whereas in another case series from Mayo Clinic, 48% (n = 52) of cases were asymptomatic.[4] Nevertheless, the common symptoms were chest pain and dyspnoea. Sudden cardiac arrest, congestive cardiac failure, acute MI, syncope, tamponade, and embolism were other notable clinical presentations in these studies. Of the patients in whom LVPA was incidentally discovered, physical examination revealed a murmur. Similarly, positive findings on chest radiographs were observed in 50% of the cases. Ninety-five percent of patients had nonspecific changes on ECG, with 20% having ST-segment elevations.[5]
In such cases, early diagnosis is of paramount importance in the management. Before the advent of newer imaging techniques, contrast ventriculography was and still is the gold standard, but it is seldom used now. Non-invasive techniques such as Transthoracic echocardiography, transesophageal echocardiography, and CMRI have been utilised in the diagnosis and differentiation of these lesions. Transthoracic echocardiography and transesophageal echocardiography are 26% and 75% effective in making a definitive diagnosis, respectively.[6] CMRI helps in differentiating LVPA from true aneurysms, and the literature reports a sensitivity of 100% and a specificity of 83%, but it is underutilised due to cost and availability issues. Nonetheless, CMRI helps in anatomic demarcation and curating a surgical plan for the patient.[7]
Previously, conservative treatment was suggested for patients with an incidental finding of LVPA and also for those having a higher surgical risk. Recent data suggests, preference for medical therapy in chronic cases, especially for lesions less than 3 mm in size, which underlines the main therapeutic objective of decreasing pseudoaneurysm enlargement.[3] This objective also emphasises the importance of decreasing ventricular wall stress by decreasing afterload and decreasing the risk of thromboembolism. With high surgical mortality (23% in the systematic review of 290 patients[1] and 28% in a recent case series of 30 patients[6]), a multidisciplinary team approach and shared making is advocated.[8]
In the contemporary era of transcutaneous therapeutic options, transcatheter approaches can be utilised for smaller pseudoaneurysms, which further reduces the risks of periprocedural complications, namely rupture, thromboembolism, pulmonary oedema and cardiac arrest. Septal occluder devices have been used in repair via the percutaneous approach. In high-risk surgery patients and those requiring a redo of cardiovascular surgery, percutaneous device closure of LVPA is preferable.[9]
Finally, the surgical management is carried out with a patch closure, which is a highly recommended choice. Post-MI LVPA benefit the most from the surgical closure of the pseudoaneurysms if the surgical intervention is performed within two to three months of the episode.[10]
Conclusion
This case report highlights the importance of high clinical suspicion of complications of MI in patients with angina with a recent history of ACS. It is prudent to mention the role of imaging in such scenarios where a quick, bedside, non-invasive and reproducible imaging modality helps in early diagnosis and decision-making for formulating a management plan.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
N/A.
Informed consent
Yes.
Credit author statement
Saurabh Bhardwaj: Research and writing
Varun Agarwal: Data collection
PK Ghosh: Echocardiography
SK Gupta: Supervised and provided critical feedback
Data availability
Data is confidential in hospital records.
Use of artificial intelligence
None.