
Abstract
Paraquat is a widely used herbicide as it is easily available. Accidental ingestion can cause high-case fatality. Even modest amounts of paraquat can be fatal. Poisoning can irritate the mouth, oropharynx and oesophagus. It also results in multiple organ failure. Pulmonary failure is the most common cause of death and lung fibrosis is the main respiratory complication in paraquat poisoning. Here, we report a rare case of paraquat poisoning presented with pulmonary thromboembolism. Our patient was already treated for paraquat poisoning and acute kidney injury with haemodialysis in an outside hospital. After 1 month, he came to our hospital with complaints of haemoptysis and shortness of breath. On further investigations, the patient was found to have a partial thrombus in the right common femoral vein and saddle embolism in the bifurcation of the right pulmonary artery extending into upper, middle and lower lobe branches. After ruling out all other causes, the reason for embolism was considered either due to paraquat poisoning per se or due to catheterisation for haemodialysis. The patient was started on anticoagulants. While treating the patient with paraquat poisoning, complications such as pulmonary thromboembolism due to haemodialysis or paraquat poisoning should also be considered.
Introduction
Pesticide poisoning remains a significant issue in low-income countries. Studies showed that pesticides were the leading cause of poisoning in adults, with a reported frequency of 63% (95% CI, 63%–64%). Pesticide poisoning was most common in North India (79.1%; 95% CI, 78.4%–79.9%), followed by South India (65.9%; 95% CI, 65.3%–66.6%).[1] Between 1995 and 2015, pesticides contributed to nearly 440,000 suicides in India, mostly in 11 states, according to NCRB data.[2] Paraquat poisoning is a big issue since it is associated with extremely high mortality (case fatality rates ranging from 50% to 70%) and morbidity.[3] Paraquat (1, 10-dimethyl-4, 40-bipyridinIum dichloride) is a fast-acting, nonselective herbicide that is widely employed since it is affordable.[4] Paraquat is dangerous in even small doses. Poisoning is generally suicidal or accidental. It can lead to oral and oesophageal ulcers, as well as hepatic, renal and pulmonary dysfunction.[5] This is a case of paraquat poisoning with pulmonary thromboembolism. In paraquat poisoning, lung fibrosis is the most common pulmonary complication. Pulmonary thromboembolism is rarely reported in paraquat poisoning.
Case Description
A 30-year-old male presented to the outpatient department with complaints of scanty haemoptysis and shortness of breath, MMRC grade 2 for 2 days. No history of fever, leg swelling, decreased urine output or any other bleeding manifestation. The patient had a history of accidental consumption of paraquat 1 month back, for which he was hospitalised in an outside hospital. He had acute kidney injury and underwent 5 sessions of haemodialysis via a right femoral catheter. The patient’s condition improved, and he was discharged with oral steroids. There is no history of smoking, alcohol consumption or tobacco chewing. The patient has no comorbidities and is not on any medication. There is no history of similar illnesses in the past or among family members.
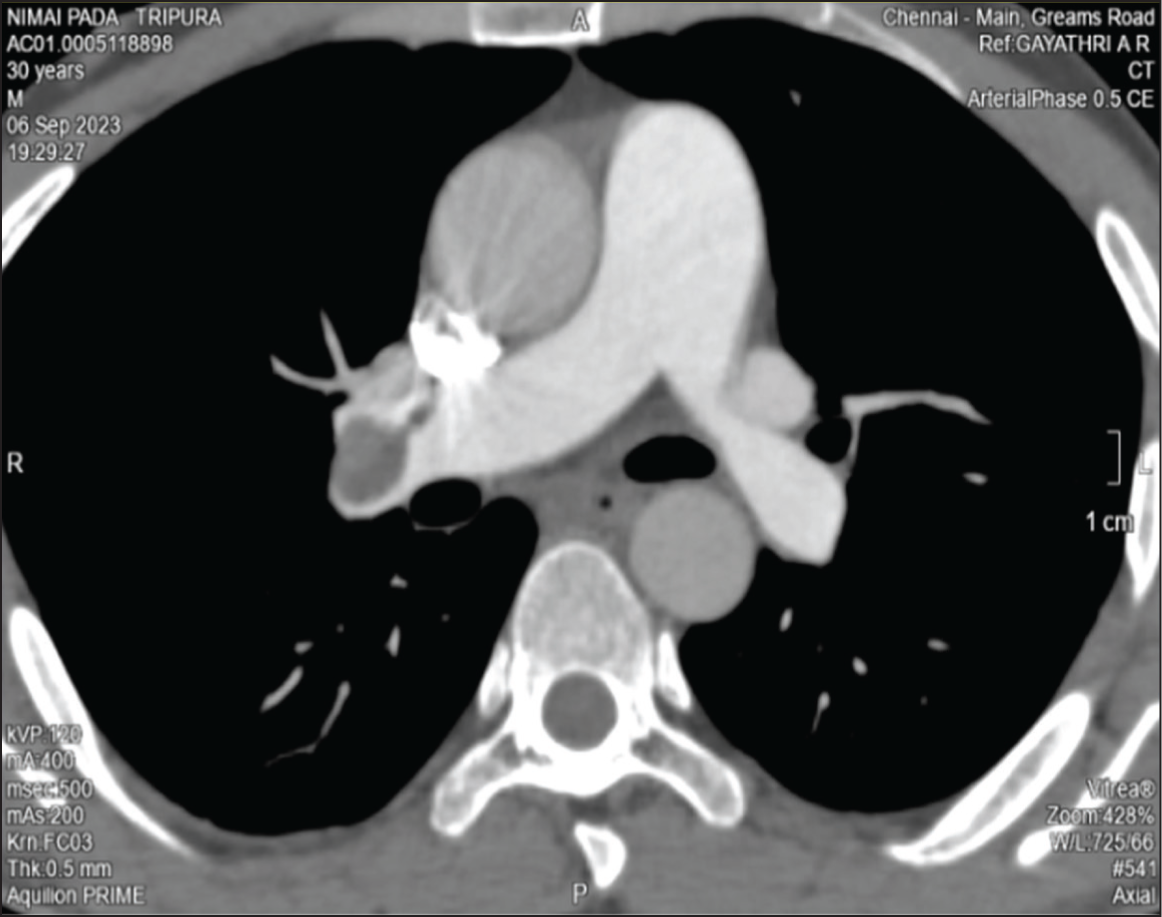
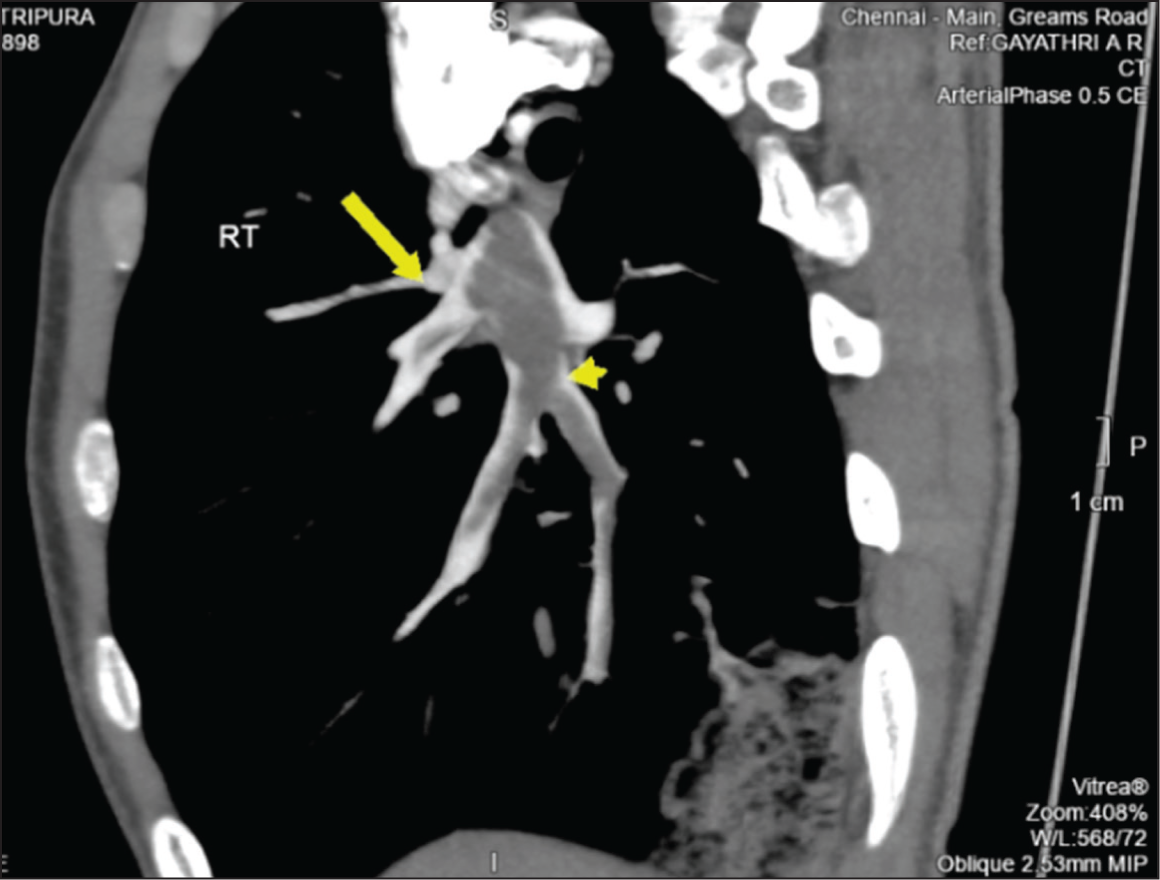
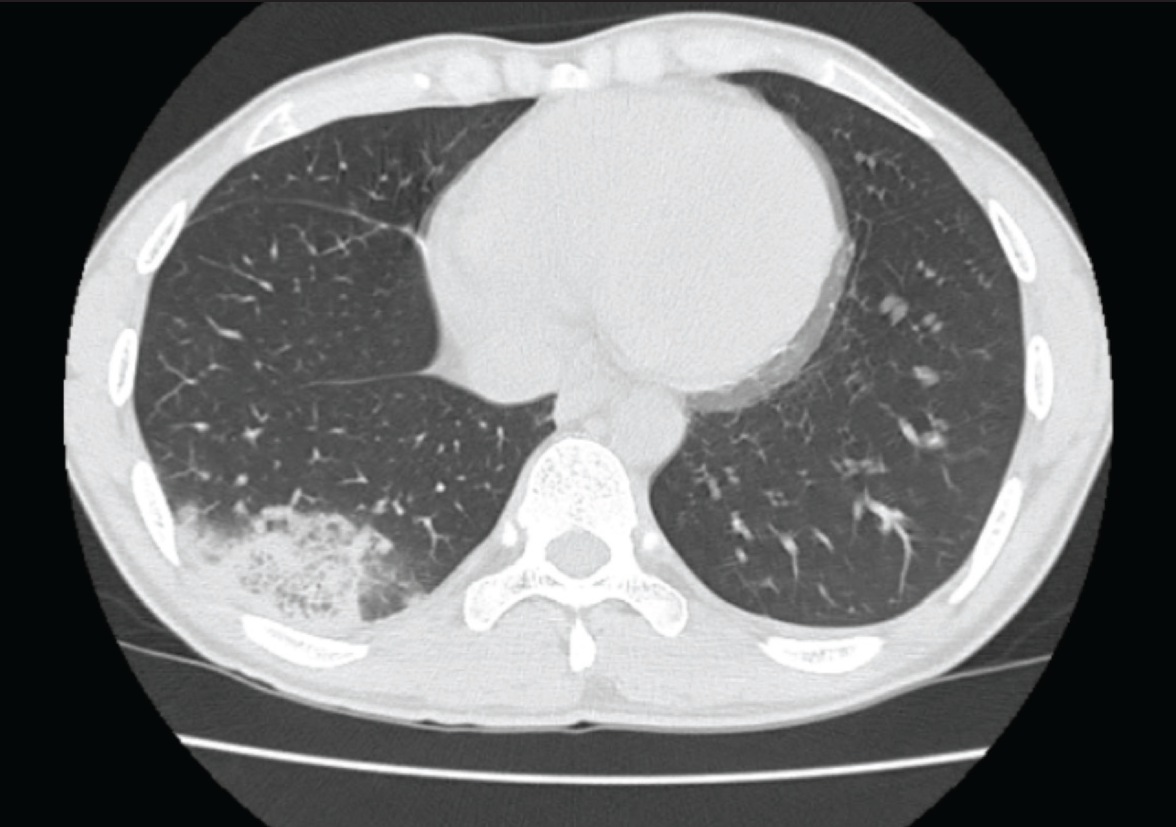
On examination, he was conscious, oriented, hemodynamically stable, afebrile and saturating 98% on room air. Bilateral normal vesicular breath sounds were heard on auscultation. Other system examinations were unremarkable. Routine blood investigation showed mild transaminitis. The echo showed an ejection fraction of 60%, no pulmonary artery hypertension and normal left and right ventricular function. Chest X-ray showed right lower zone heterogeneous opacity. The patient underwent computer tomography of the chest and abdomen with contrast, showing partial thrombus in the right common femoral vein, saddle embolism in the bifurcation of the right pulmonary artery extending into upper, middle and lower lobe branches, and right lower lobe wedge-shaped area of ground glass opacities interspaced with consolidation [Figures 1–3]. Activated partial thromboplastin time, prothrombin time, bleeding time and clotting time were normal. Anti-double-stranded DNA, antineutrophil cytoplasmic antibody and antinuclear antibody test results were negative. To rule out inherited and acquired causes of thrombosis, a thrombophilia package was done, which included antiphospholipid antibody, cardiolipin antibody, factor II and V mutation, antithrombin III, protein S, protein C, Beta 2 glycoprotein, homocysteine level and fibrinogen level. Immunoglobulins M and G were normal. The pulmonary function test was normal. The diffusion capacity of the lung for carbon monoxide was mildly reduced. Bilateral lower limb venous Doppler was normal. Since the patient’s renal function was normal and he refused to be admitted, parenteral treatment or comply with prothrombin time monitoring if warfarin or acitrom were started, a direct oral anticoagulant, that is, rivaroxaban, was started.
Discussion
Paraquat toxicity is primarily caused by the production of reactive oxygen species (ROS), which damage cells through mechanisms such as mitochondrial toxicity, lipid peroxidation, oxidation of nicotinamide adenine dinucleotide phosphate, activation of nuclear factor kappa B and apoptosis.[6] It affects both type I and II pneumocytes in the lung, resulting in acute alveolitis. The alveolitis is followed by a ‘proliferative’ or ‘cellular’ phase, resulting in lung fibrosis.[7] Paraquat can also cause renal and liver injury, leading to the requirement of haemodialysis.[8] Early signs of paraquat poisoning include mucosal ulcers in the mouth and tongue, also known as ‘paraquat tongue’. There is no particular antidote for this overdose and limited evidence-based therapeutic options.[8]
Management is primarily supportive. Activated charcoal is advised for gastric cleansing within 1–2 hours of consumption. However, stomach lavage is not recommended due to paraquat’s corrosive nature. Supplemental oxygen is not indicated for individuals with mild-to-moderate hypoxia because it can enhance the generation of ROS, causing increased damage. Paraquat toxicity has been treated with immunosuppressive medications such as cyclophosphamide, methylprednisolone and dexamethasone, as well as antioxidants such as N-acetylcysteine.[9] The interaction between nitric oxide and superoxide generates peroxynitrite, which causes oxidative endothelium damage. The thrombus formation mechanism can be explained by Virchow’s triad, that is, hypercoagulability, venous stasis or turbulence, and endothelial damage. Daisey H et al. have published a case report of a patient with paraquat poisoning showing diffuse microthrombi, specifically thrombotic microangiopathy within terminal arterioles and alveolar capillaries in the lung autopsy.[10] Paraquat poisoning with acute kidney injury requiring venous catheterisation and haemodialysis can also lead to pulmonary thromboembolism, as femoral and central vein catheterisation causes endothelial injury and pulmonary thromboembolism. Chao et al. published a case report detailing a patient with paraquat poisoning who developed a pulmonary embolism related to dialysis catheters. In contrast to our case, the patient was hypoxemic during admission and was started on an anticoagulant and discharged. Patient was evaluated for pulmonary embolism and the possible aetiology of pulmonary embolism was considered due to catheterisation for haemodialysis.[9]
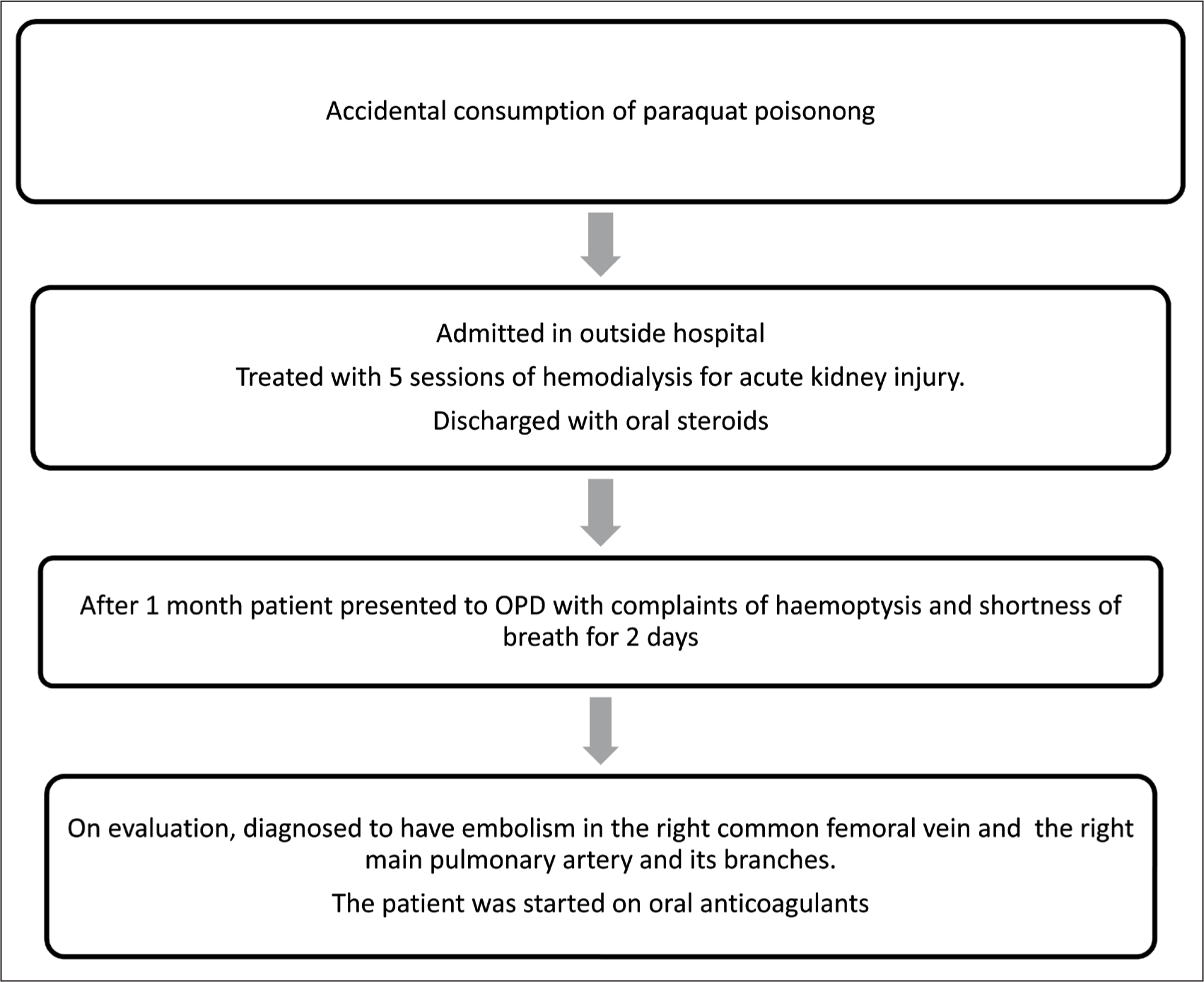
Our patient has been evaluated for embolism, and all thrombophilic factors were ruled out. Venous Doppler was also done to rule out deep venous thrombosis due to hospitalisation and immobilisation, which was normal. The patient had undergone haemodialysis via a femoral catheter outside the hospital. In our case [Figure 4], the possible aetiology of pulmonary embolism was considered either due to paraquat poisoning or catheterisation for haemodialysis.
Flowchart showing the sequence of events leading to diagnosis and treatment
Conclusion
Paraquat poisoning causes respiratory failure mainly due to pulmonary fibrosis. While treating the patient with paraquat poisoning, complications such as pulmonary thromboembolism due to haemodialysis or paraquat poisoning should also be considered.
Footnotes
Acknowledgements
To Dr Shivashankari, Research Assistant and Mr Logesh, Biostatistician, Research Department, Apollo Hospital, Chennai.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
The article is a case report and no specific ethical committee approval is required.
Informed consent
Informed consent has been obtained from all the patients who met the eligibility criteria.
Credit author statement
NKK participated in data acquisition, literature search, investigations, data analysis, and manuscript preparation.
GDAR participated in conceptualisation, investigation, supervision, validation and manuscript editing.
Both authors reviewed and approved the manuscript.
Patient consent
This article is a Case report and no specific patient consent is required. Patient consent obtained as per standard policy of Apollo Hospitals, Chennai.
Data availability
Data presenting the study’s findings is available from the corresponding author.
Use of artificial intelligence
NIL.