
Abstract
Introduction:
Postoperative pain after knee surgery affects the early postoperative joint mobility and rehabilitation of patients. Peripheral nerve block is an effective method to prolong the duration of postoperative analgesia and reduce need of systemic analgesic with less complications. We did the study of single-shot peripheral nerve stimulator (PNS)-guided FNB (femoral nerve block) and PNB (popliteal nerve block) with ropivacaine (0.25% and 0.375%) with an aim to compare the postoperative analgesic efficacy.
Materials and Methods:
Prospective, double blind, randomised comparative study of 50 patients of American Society of Anesthesiologists (ASA) Grade I–III aged 18–70 years posted for knee surgeries under spinal anaesthesia (SA) was done. Postoperatively both groups A and B received FNB (30 mL) and PNB (20 mL) with ropivacaine (0.25%) and (0.375%) respectively. Postoperative visual analogue scale (VAS) score at rest and on movement, total duration of analgesia and number of rescue analgesic required in 24 hours were noted.
Results:
Postoperative VAS score at rest at four hour was significant (5.0 + 1.4) in group A compared to group B (3.44 + 1.1) (P < .05), while VAS on movement at two and four hour was significant (2.16 ± 1.78 and 5.24 ± 1.10) in group A compared to (1.32 ± 1.00 and 4.56 ± 1.1) in group B (P < .05). Mean duration of analgesia was longer in group B (P < .05) and total analgesic consumption in 24 hours was higher in group A (P < .05).
Conclusion:
PNS-guided single-shot FNB and PNB improve quality of analgesia after knee surgery done under SA with ropivacaine 0.375% having longer duration of analgesia compared to 0.25% without much side effects.
Keywords
Introduction
Total knee arthroplasty (TKA) and other knee surgeries involve extensive tissue trauma,[1] contributing to the development of severe postoperative pain.[2] Postoperative pain after knee surgeries remains challenging for an anaesthesiologist as poorly managed acute postoperative pain can lead to the occurrence of chronic pain. Effective postoperative analgesia reduces patient’s anxiety and accelerates recovery. It suppresses the troublesome postoperative stress response and pain induced hypoxia in the early postoperative period. The regular use of nonsteroidal inflammatory drugs (NSAIDs) and opioids does not provide satisfactory analgesia.[3,4]
So, multimodal analgesia to combat postoperative pain after knee surgeries has been commonly utilised. It consists of a combination of oral and/or intravenous (iv) analgesics opioids, epidural analgesics and peripheral nerve blocks. As compared to epidural and iv analgesic, peripheral nerve blocks are associated with less side effects and more haemodynamic stability.
The peripheral nerve blocks are done by various methods like loss of resistance technique, by using nerve stimulator and ultrasonography (USG)-guided blocks. USG-guided blocks are reliable but due to lack of facility of USG at our hospital, we decided to give femoral nerve block (FNB) and popliteal fossa block (PFB) using peripheral nerve stimulator.
Lignocaine and bupivacaine have been the most widely used local anaesthetic because of its fast onset/short duration characteristic, but both of them are associated with a very high incidence of central nervous system (CNS) and cardiovascular system (CVS) toxicity.[5] But ropivacaine is associated with less toxicity and having relatively better sensory and motor block profiles.[6]
So, we decided to do our study with the aim to compare the postoperative analgesic efficacy and safety of PNS-guided single shot FNB and PFB using different concentration (0.25% or 0.375%) of ropivacaine after knee surgeries.
The primary objective was to compare the visual analogue scale (VAS) pain score at rest and on movement. Secondary objectives were to compare total duration of analgesia, number of rescue analgesic required in 24 hours.
Materials and Methods
We conducted a prospective, double blind, randomised, comparative study of 50 patients of American Society of Anesthesiologists (ASA) Grade I–III aged between 18 and 70 years scheduled for various knee surgeries (total knee arthroplasty [TKR], anterior cruciate ligament [ACL] and posterior cruciate ligament [PCL]) under spinal anaesthesia (SA) after approval from institutional ethics committee, reg.no/IEC/9201/2014. Patients in the age group 18-65 years posted for elective unilateral knee surgeries (TKR, ACL and PCL repair) agreed for participation in study with no contraindication for regional and SA were included in study. Randomisation was done with computer-generated random numbers with sealed envelope.
All patients were randomly divided into two groups.
Group A: FNB (30 mL) + PFB (20 mL) ropivacaine (0.25%)
Group B: FNB (30 mL) + PFB (20 mL) ropivacaine (0.375%)
Sample size was calculated based on previous study by Alpaslan Apan et al.[30] for postoperative analgesic consumption in 24 hours. Considering dropouts, 25 patients were taken in each group.
All patients underwent a preanaesthetic checkup before surgery and all routine investigations were documented. Patients were kept NBM for six hours prior to surgery. In all patients, informed consent for SA as well as for FNB and PFB was obtained. An IV line was secured with 18G/20G IV canula; standard monitors were connected and vitals were recorded.
Under all aseptic and antiseptic precautions, lumbar puncture was performed with 23-gauge Quincke spinal needle in L3-L4 Intervertebral space in the sitting position. Following the free flow of cerebrospinal fluid (CSF), inj. bupivacaine hyperbaric 0.5% (3.5 mL) was injected. Times of completion of surgery were noted and at the end of surgery both nerve blocks were performed using a Braun (Bethlehem, PA) 2 inches Stimuplex Needle and a Braun Stimuplex Dig RC nerve stimulator under all aseptic and antiseptic precautions, starting at 1.5 mA and decreasing to 0.5 mA (2 Hz) until adequate contractions noted quadriceps contractions (patellar dance) in FNB and foot/toe twitch in PFB.
After appropriate twitch response, 30 mL of inj. ropivacaine 0.25% (group A) or 0.375% (group B) in FNB and 20 mL inj. Ropivacaine 0.25% (group A) or 0.375% (group B) in PFB respectively was injected.
The observer and the patient were blinded for the study drug. After that patients were transferred to the post-anaesthesia care unit (PACU). Severity of pain was assessed by an investigator blinded to group allocation at 0 minutes, 30 minutes, 1 hour, 2 hours, 4 hours, 6 hours, 12 hours and 24 hours postoperatively. Pain severity was measured using a VAS at rest and on movement. VAS at rest refers to pain levels when the patient is lying still, without any movement. In contrast, VAS on movement assesses pain when the patient is asked to move the limb, such as bending the knee or performing a slight leg raise.
Duration of analgesia was defined as mean time from the time of block to the first analgesic requirement. Rescue analgesic was given in form of inj Diclofenac sodium 75 mg intramuscular (IM) when VAS≥5. Total duration of analgesia and total amount of analgesic requirements in 24 hours were recorded.
All observations were recorded as mean and standard deviation. All results were analysed statistically with Microsoft Excel and were compared using the students unpaired ‘t’ test; P value ≤ .05 was considered as significant.
Observation and Result
We carried out a prospective, double blind, randomised comparative study of 50 patients with 25 patients in each group. Blocks (FNB and PFB) were given with ropivacaine (0.25%) in group A and ropivacaine (0.375%) in group B after various knee (TKR, ACL/PCL repair) surgeries operated under SA.
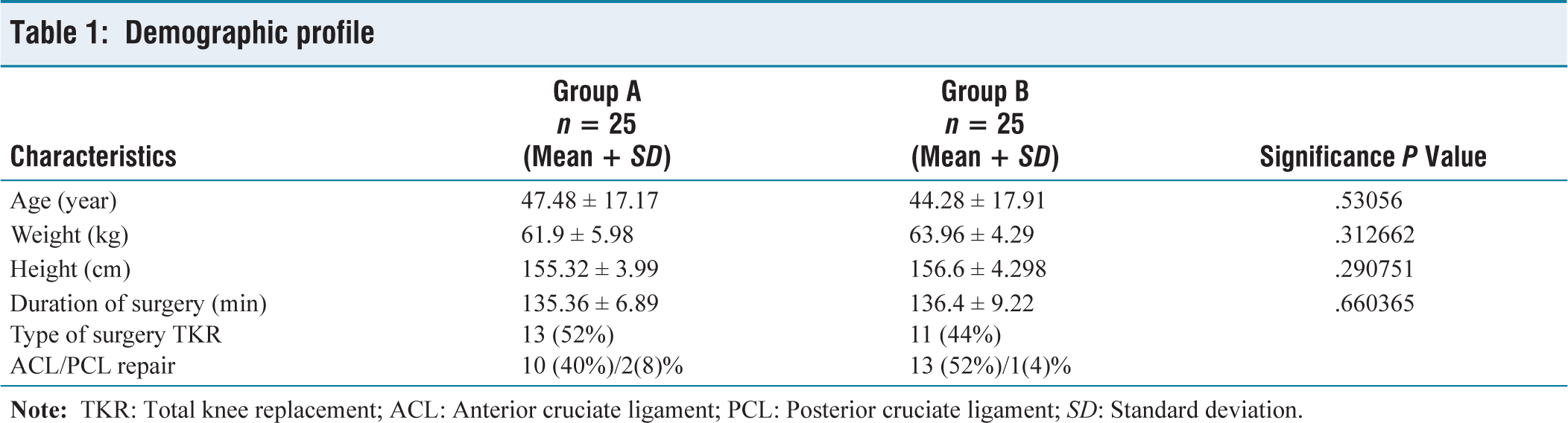
Table 1 shows demographic data were comparable in both groups. The average duration of surgery was comparable between the two groups. In group A average duration of surgery was 135.36 ± 6.89 minutes and in group B was 136.4 ± 9.22 minutes (P = .660), indicating no statistically significant difference.
Demographic profile
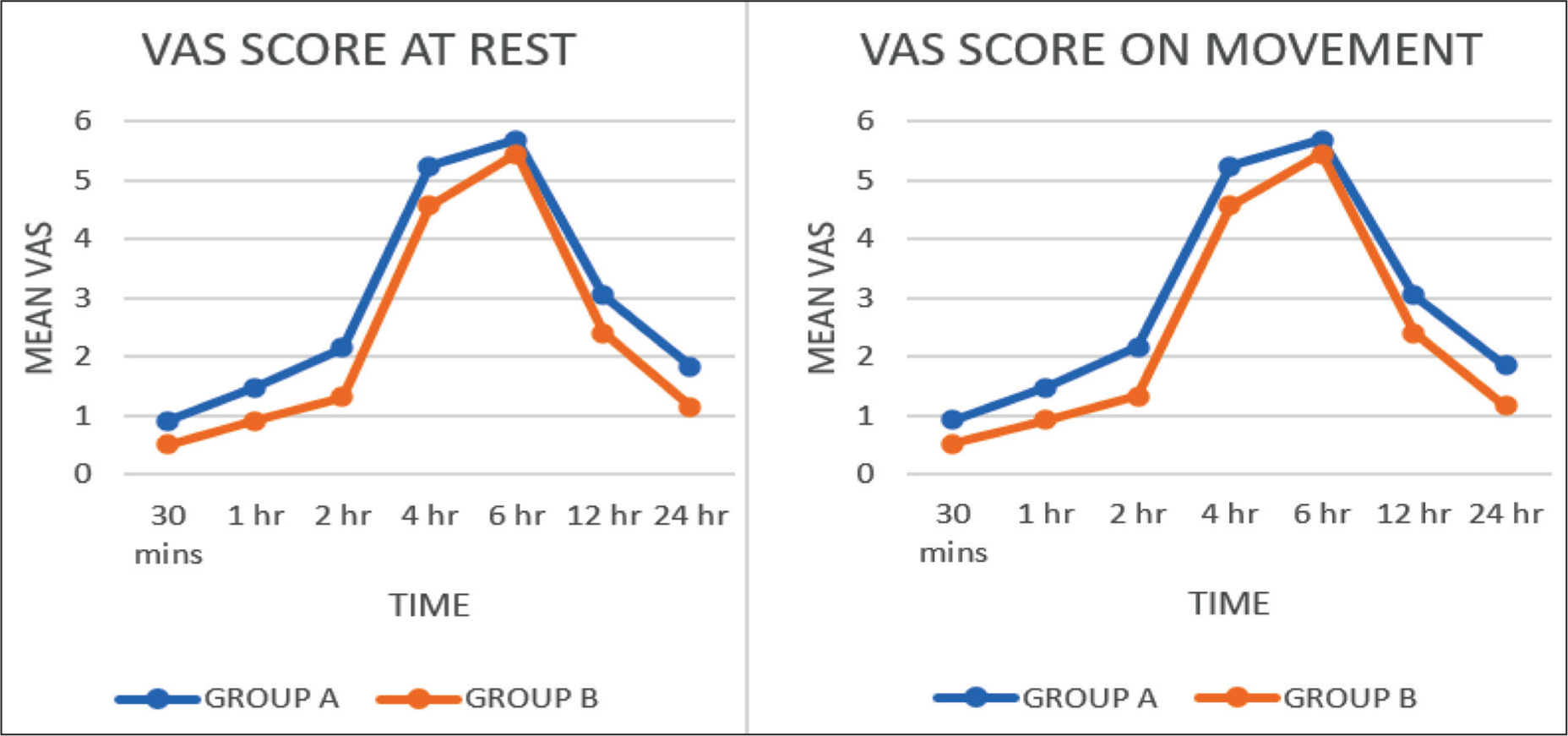
Postoperative VAS score at rest was 5.0 ± 1.4 and 3.44 ± 1.1 in group A and group B respectively (P < .05) which was statistically significant. VAS score on movement at two and four hour was 2.16 ± 1.78 and 5.24 ± 1.10 in group A, while it was 1.32 ± 1.00 and 4.56 ± 1.1 in group B (P < .05) which was significant statistically as shown in Figure 1.
Postoperative vas score at rest was 5.0 ± 1.4 and 3.44 ± 1.1 in group A and group B respectively and on movement was 2.16 ± 1.78 and 5.24 ± 1.10 in group A while it was 1.32 ± 1.00 and 4.56 ± 1.1 in group B which was statistically significant
Mean duration of analgesia was 368.8 ± 53.16 minutes in group B and 262 ± 117.4 minutes in group A. It was longer in group B compared to group A which was statically significant (P < .05) as shown in Figure 2.
Duration of analgesia, mean duration of analgesia was 368.8 ± 53.16 minutes in group B and 262 ± 117.4 minutes in group A. It was longer in group B compared to group A which was statistically significant (P < .05)
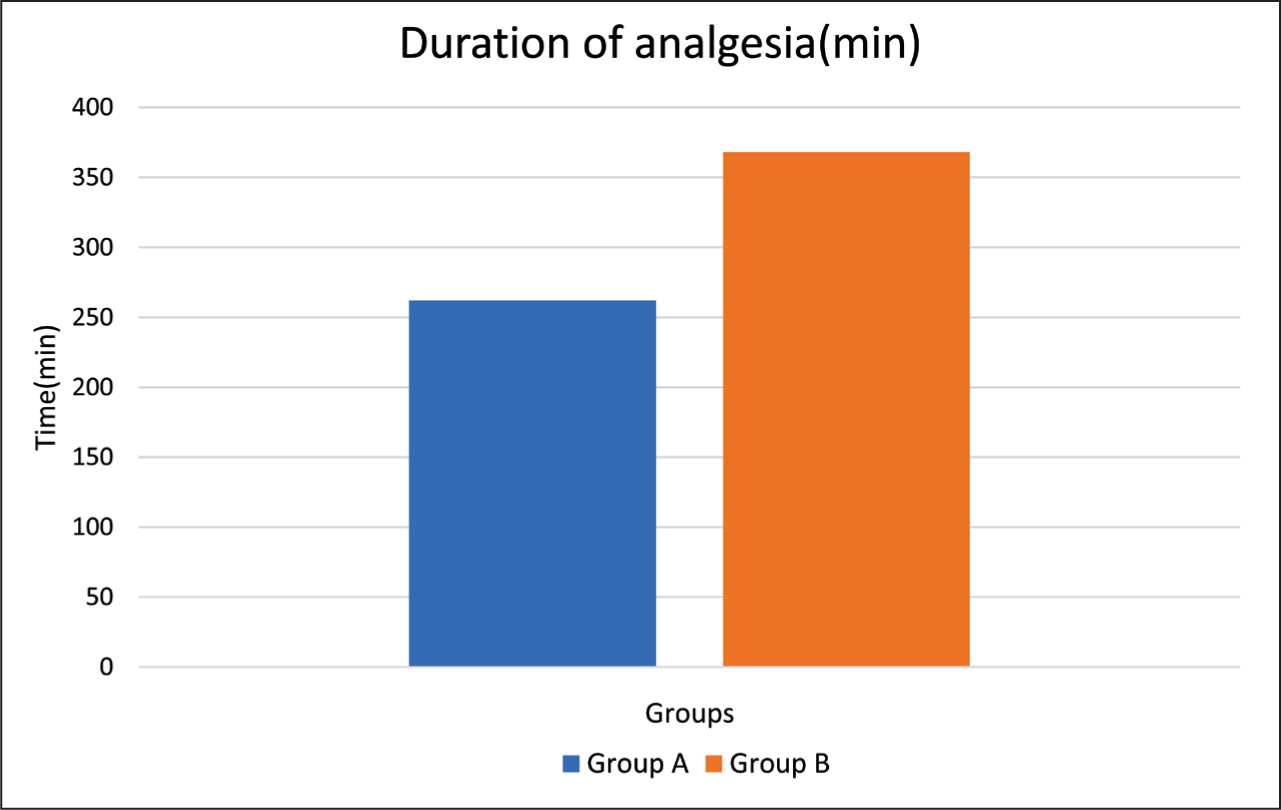
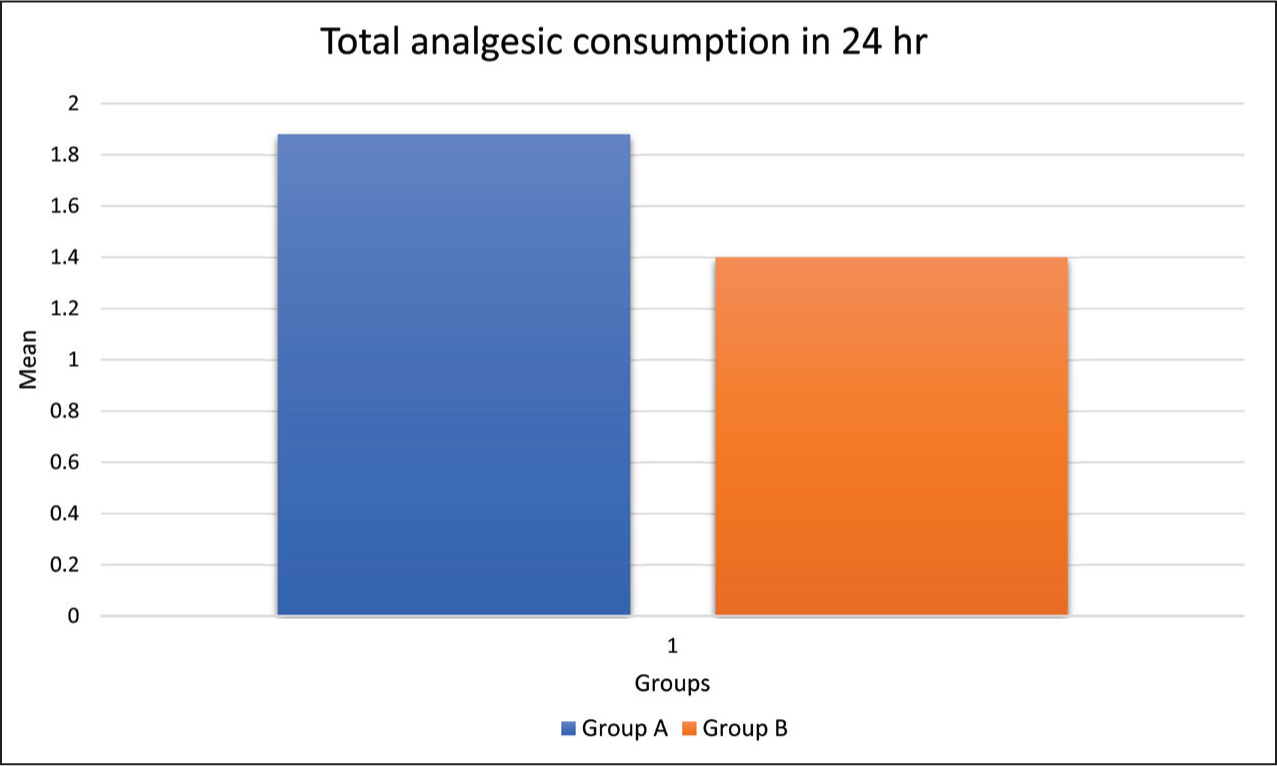
Figure 3 shows total analgesic consumption in 24 hours was higher in group A (1.88 ± 0.65) compared to group B (1.4 ± 0.5) which was statistically significant (P < .05).
Total analgesic consumption in 24 hours was higher in group A (1.88 ± 0.65) compared to group B (1.4 ± 0.5) which was statistically significant (P < .05)
In our study, there were no any complication during the performance of FNB and PFB in both the groups. Five patients (20%) in group A and one (4%) patient in group B developed nausea and vomiting, two patients (8%) in group A developed hypotension, one patient (4%) in both the group A and B developed shivering and one patient (4%) in group developed bradycardia.
Discussion
Postoperative pain after TKR, ACL, PCL repair and other knee surgeries remains challenging. Postoperative pain in the TKR surgery and other knee surgeries is so severe; hence, effective postoperative analgesia[7,8] is essential for early physical rehabilitation to prevent joint adhesion following knee replacement, to suppress the troublesome postoperative stress response and pain induced hypoxia in the early postoperative period. Postoperative pain relief can be achieved by IV analgesia, intrathecal opiods[9] and epidural analgesia. Regional technique provides better pain relief and faster postoperative knee rehabilitation than IV. Compared with epidural anaesthesia, peripheral nerve block is associated with fewer side effects and is an effective regional component of multimodal analgesic strategy after TKR surgery.[10] So, we decided to do the study of femoral and PFB using peripheral nerve stimulator at the end of surgery done under SA.
However, studies have shown that FNB in knee surgery patients results in significant reduction in overall postoperative analgesic requirement for the first 24 to 48 hours following surgery.[11–16] However, the FNB provides analgesia to anterior portion of the knee and many patients who undergo an extensive surgical procedure to the knee have complain of pain in posterior portion as well, thereby necessitating supplemental analgesia to achieve postoperative comfort.[17–19] using PFB.
The effectiveness of femoral nerve block (FNB) alone in knee surgeries remains controversial, as the sciatic nerve may also contribute to the postoperative pain. So, several studies done by Abdallah et al.,[20] Raul Cervalho et al.,[21] Zugliani et al.[22] have combined sciatic nerve block with FNB to improve postoperative analgesia after knee surgeries. We did the study of femoral and popliteal FNB after knee surgeries.
In our study, postoperative analgesia was assessed by VAS (pain) score. We recorded VAS at rest and VAS on movement postoperatively. And we found that VAS at four hour was significant statistically. Mean VAS on movement at two and four hour was statistically significant. At two and four hour after giving block pain score was assessed which was higher in group-A compared to group-B which may be due to the difference in concentration of Ropivacaine used for block (In Group-A 0.25% Ropivacaine and in Group-B 0.375% Ropivacaine).
Mehmet et al.[23] did the study to compare effect of preoperative three in one FNB (0.375% ropivacaine) and use of morphine for postoperative pain in TKR surgery. Both the groups received general anaesthesia and postoperatively had patient-controlled analgesia (PCA) to deliver morphine. They concluded that preoperative FNB provides better VAS score.
In our study, we compared two different concentrations of ropivacaine (0.25% and 0.375%) in FNB and PNB given postoperatively after knee surgeries.
Ng et al.[24] did the study of patients undergoing unilateral TKR under general anaesthesia using femoral nerve block with ropivacaine 0.25%, ropivacaine 0.5% and bupivacaine 0.25% and found that there were no significant differences in pain scores among the three local anesthetic groups. They found visual pain score (VPS) was significantly lower in ropivacaine group (0.25% and 0.5%) compared to bupivacaine group postoperatively (P < .05). We did the study of femoral nerve block and popliteal fossa block with two different (0.25% & 0.375%) concentration of ropivacaine after knee surgeries done under spinal anaesthesia and found that VAS score was higher in 0.25% ropivacaine compared to 0.375% ropivacaine.
De Lima E Souza et al.[25] did the study of single injection femoral nerve block with 0.25% bupivacaine (Group-B) and 0.25% ropivacaine (Group-R) and control group (Group-C) for postoperative pain relief after knee surgeries and concluded that both the groups (Group-B and Group-R) are having effective postoperative analgesia after TKR and ACL surgery. And found VAS was significant lower in ropivacaine group.
Essving et al.[26] compared local infiltration analgesia (ropivacaine, ketorolac and epinephrine) with intrathecal morphine for postoperative analgesia after TKR. They found that local infiltration analgesia technique provide better postoperative analgesia and early mobilization than intrathecal morphine after TKR. They concluded this prolonged effect might be due to mixture of all three drugs used for local infiltration.
Beaulieu et al.[27] compared effect of bupivacaine (0.5%) and ropivacaine (0.5%) in combined sciatic and FNB in patients posted for total knee arthroplasty and found that overall pain scores and morphine consumption were similar.
Paauwe et al.[28] compared different concentration of ropivacaine 0.1%, 0.05% or 0.025% on patient’s postoperative rehabilitation and analgesia. And they found no advantage associated with ropivacaine concentration less than 0.1%.
Our study compared effectiveness of different concentration of ropivacaine 0.25% and 0.375% for postoperative analgesia after knee surgeries. Study by Alpaslan Apan et al.[30] compared postoperative analgesia of single shot ‘3-in-1’ FNB using 0.25% or 0.375% levobupivacaine in combination with spinal anaesthesia for unilateral TKR surgery and observed no statistically significant difference in pain scores assessed with VAS during passive movement.
Mean duration of analgesia was calculated as the mean time from end of the surgery to first analgesic requirement was longer in group B ropivacaine (0.375%) 368.8 ± 53.16 minutes (6.1 hours) compared to group A ropivacaine (0.25%) 262 ± 117.4 minutes (4.36 hours) which was statistically significant (P < .0002).
Jansen et al.[29] compared femoral sciatic nerve block (FSB) with FNB only and found that mean duration of analgesia was 496.5 + 241.6 minutes in FSB group and 366.1 + 138.34 minutes in FNB group which was statistically significant (P = .016), while our study we compared ropivacaine (0.25% and 0.375%) in femoral and PNB after knee surgery.
Affonso et al.[22] compared FNB in group A with 0.5% ropivacaine, while in group B femoral plus sciatic nerve block was given after TKR under spinal anaesthesia. They found the mean length of time of postoperative analgesia M1 was 110 minutes (minimum 50 maximum 645 minutes) in group A and 1285 minutes (minimum 990- maximum 1510) in group B and this difference was statistically significant (P = .0001). Duration of analgesia was longer in this study than our study result this might be due to higher concentration (0.5%) of ropivacaine used in combined sciatic and FNBs.
Alpaslan Apan et al.[30] study compared postoperative analgesia of single shot 3-in-1 FNB using 0.25% or 0.375% levobupivacaine in combination with spinal anaesthesia for TKR and they found VAS and analgesic consumption for 24 hours were similar in both groups.
In our study, total consumption of analgesic injection diclofenac sodium in mg was less 105 ± 37.5 mg in group B than 141 ± 48.75 mg in group A which was statistically significant (P = .0006). Similar results reported by Mehmet et al.5 found that there was a statistically significant difference in terms of morphine consumption between two groups at the 12th, 18th, 24th and 48th hours (P < .001) with lower values in group R.
Ng et al.[24] compared the analgesic efficacy of ropivacaine (0.25%, 0.5%) and bupivacaine (0.25%) in FNB in patients posted for TKR. They found that pain score and morphine requirement were significantly lower in group R1 (ropivacaine 0.25%), group R2 (ropivacaine 0.5%) and with group B (bupivacaine 0.25%) compared to the control group up to 48 hours postoperatively (P < .05).
Alpaslan Apan et al.[30] observed total analgesia required in 24 hours in form of morphine consumption for 24 hours was 19.7 ± 9.2 in group 1 and 20.6 ± 12.1 mg in group 2 had no statistically significant difference for 0.25% or 0.375% levobupivacaine in preceding with spinal anaesthesia for unilateral TKR.
In our study, there were no any complication during the performance of FNB and PFB in both the groups. Five patients (20%) in group A and one (4%) patient in group B developed nausea and vomiting, two patients (8%) in group A developed hypotension, one patient (4%) in both the group A and B developed shivering and one patient (4%) in group developed bradycardia. All these side effect occurs intraoperative probably due to spinal anaesthesia. None of the patient had any other complications.
Mehmet et al.[23] had observed no complication during 3-in-1 FNB. In morphine group, eight, six and three patients had developed nausea, vomiting and hypotension respectively, while in ropivacaine group four patients had developed nausea.
Conclusion
We concluded that use of single shot PNS-guided FNB and PFB with equal volume (30 + 20 mL) of either 0.25% or 0.375% ropivacaine improves quality of analgesia after knee surgeries done under spinal anaesthesia. About 0.375% ropivacaine group has a longer duration of analgesia compared to 0.25% ropivacaine without much side effects. PNS-guided block is faster and easier to perform with less chances of failure of block.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
reg.no/IEC/9201/2014.
Informed consent
Informed Consent was obtained prior to spinal anaesthesia as well as FNB and PFB as mentioned in material and method.
Credit author statement
Khatija Dalvani and Jigisha Badheka were involved in conceptualisation, designing, definition of intellectual content, literature search, clinical studies, experimental studies, data acquisition, data analysis, statistical analysis and manuscript preparation, editing and review.
Shraddha Mehta helped in literature search, clinical studies, experimental studies, data analysis and manuscript preparation, editing and review.
Rakhi Goyal helped in literature search, clinical studies, experimental studies, data acquisition, data analysis, statistical analysis and manuscript preparation, editing and review.
Shahin C was involved in clinical studies, experimental studies, data acquisition and manuscript preparation, editing and review.
Anand Bhalodiya was involved in clinical studies, experimental studies and manuscript editing and review.
Khatija Dalvani and Jigisha Badheka have provided guarantee for this study.
Data availability
Data is available in our department.
Use of artificial intelligence
No artificial intelligence tools were used in the preparation of this manuscript.