
Abstract
Whipple surgery, also known as pancreaticoduodenectomy, is a complex surgery used to treat neoplasms involving the pancreas, duodenum and common bile duct (CBD). It is a ‘resection and anastomosis’ surgery involving resection of the pancreatic head and uncinate process, duodenum, CBD and gall bladder with anastomosis of jejunum with remnant pancreas, stomach and common hepatic duct. This procedure is associated with significant distortion of the normal anatomy as well as many post-operative complications. In this article, we aim to understand the basic surgical techniques of pancreaticoduodenectomy, the correct computed tomography (CT) protocol that needs to be employed, the normal findings which may be misinterpreted as post-operative complications and also review the imaging findings of various complications involving the anastomotic sites, like pancreatic fistula, anastomotic strictures, anastomotic leaks and abscesses. The awareness of normal post-operative findings and these complications is necessary to guide appropriate treatment strategies.
Introduction
Whipple surgery is an important surgery used to treat the malignant pathologies affecting the pancreatic head and neck, periampullary region, distal common bile duct (CBD) and duodenum. Despite advancements in the fields of radiation and medical oncology, surgical resection continues to remain the treatment of choice in offering a potential cure to patients with pancreatic adenocarcinoma. Improvements in the surgical procedures and techniques, along with better critical care, have significantly lowered the mortality that was earlier associated with a radical surgery like Whipple surgery. Cross-sectional imaging of the abdomen using computed tomography (CT) plays a pivotal role in post-operative management, helps identify the normal post-operative appearance and also the complications.
The Whipple Surgery or Pancreaticoduodenectomy
The surgical procedure of Whipple surgery can be broadly categorised into two types: The classic Whipple and the pylorus-preserving Whipple surgery. Both the surgical techniques include resection of the pancreatic head, uncinate process and neck; duodenum and proximal jejunum; gall bladder and distal CBD, along with regional lymph nodes resection. In the classic variant, the gastric antrum is also resected, whereas in the pylorus-preserving variant, the gastric antrum and the first part of the duodenum are preserved. It was earlier believed that pylorus-preserving surgery has a lower incidence of bile reflux; however, recent literature confirms no such advantage of pylorus-preserving surgery over the classic Whipple surgery.[1–3] The resection is followed by three anastomoses: pancreaticojejunostomy, hepaticojejunostomy, gastrojejunostomy (GJ) or duodeno-jejunostomy and sometimes an additional anastomosis in the form of jejuno-jejunostomy.
MDCT Scan Protocol
CT is the imaging modality of choice for the evaluation of any post-operative complication occurring after Whipple surgery. It is superior to Magnetic Resonance Imaging (MRI), in being easily available, allowing for faster acquisition time and being less prone to misinterpretation in cases of calcification or air in the biliary tree.
Positive Versus Neutral Enteric Contrast
A routine post-operative CT scan is performed 3–6 months after the surgery in cases where there are no clinical signs or symptoms to suggest any complication. In routine post-operative imaging, water or any neutral contrast is preferred over positive oral contrast material, as streak artefacts resulting from positive oral contrast can lead to sub-optimal evaluation of the pancreatic bed. Moreover, the positive oral contrast interferes with the 3D post-processing and also obscures sites of intestinal haemorrhage.[1]
In immediate post-operative imaging, where anastomotic leaks are suspected, one may prefer positive oral contrast over neutral enteric contrast. Positive oral contrast also helps in better differentiation of bowel loops from any intrabdominal collection.[4] Fistulas are also better demonstrated with the use of positive oral contrast
CT Protocol
Plain scan (using neutral or positive enteric contrast) is performed from diaphragm to pubic symphysis before administration of non-ionic IV contrast injected @3–5ml/sec. A dual-phase scanning protocol is followed, with image acquisition after 30 sec (late arterial /pancreatic parenchymal phase) and 60 sec (portal venous phase) of IV contrast administration in order to achieve optimal pancreatic parenchymal and vascular enhancement [Table 1].
CT protocol
Normal Post-operative Appearance
Pancreatico-jejunostomy Site (PJ Site)
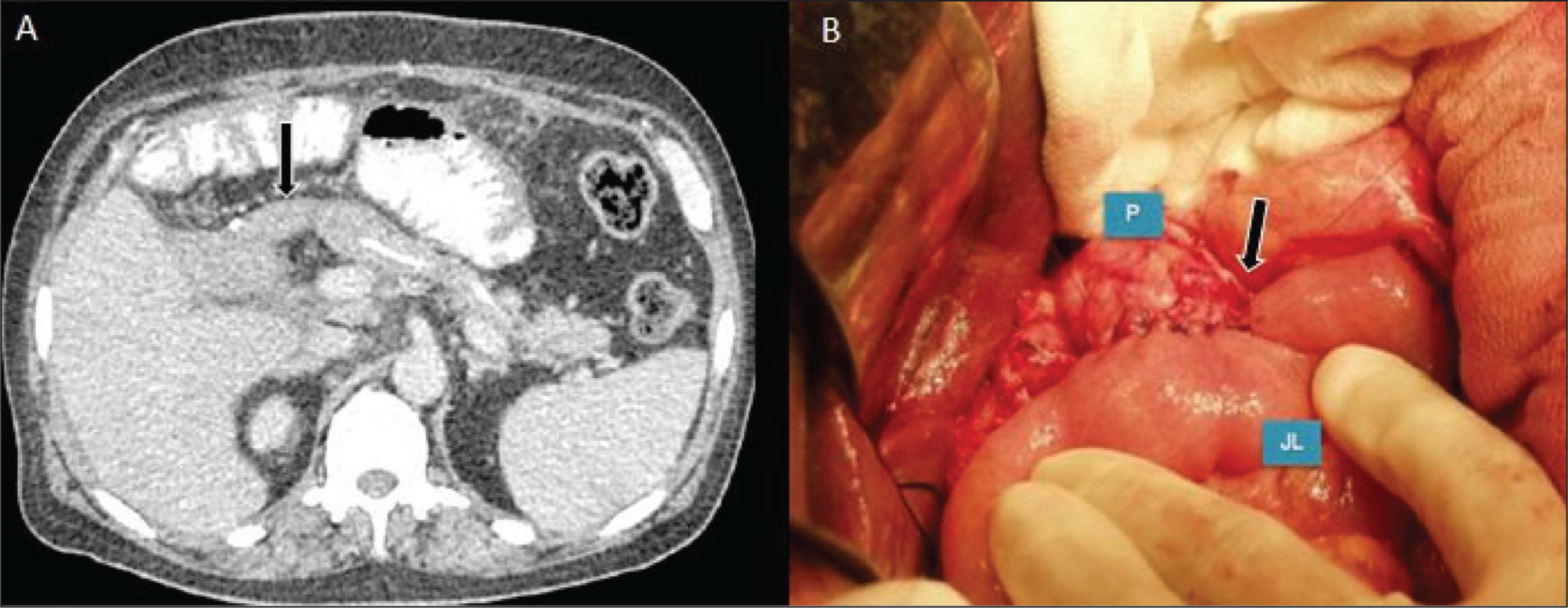
The jejunal loop, which is anastomosed with the pancreatic duct, can often mimic a haematoma or recurrence of tumour, especially in its collapsed state. The appearance and course of the jejunal loop are the two major key factors which help in the identification of the anastomosed jejunal loop on CT. The enhancement of the jejunal loop wall following IV contrast administration, as well as the delineation of folds by the presence of low attenuation intraluminal bowel fluid or the presence of air in the bowel lumen, can help in recognising the jejunal loop. The jejunal loop is anastomosed to the right side of the remnant pancreas, anterior to the superior mesenteric artery. Often, the presence of a surgical drain across the PJ site, seen in the immediate post-operative period, can aid in the identification of the jejunal loop [Figure 1].
Axial MDCT (A) and Intra-operative image (B) showing the anastomosis (black arrow) between pancreas (P) and jejunum (JL)—the pancreaticojejunostomy site
Hepato-jejunostomy/Choledocho-jejunostomy Site (HJ Site)
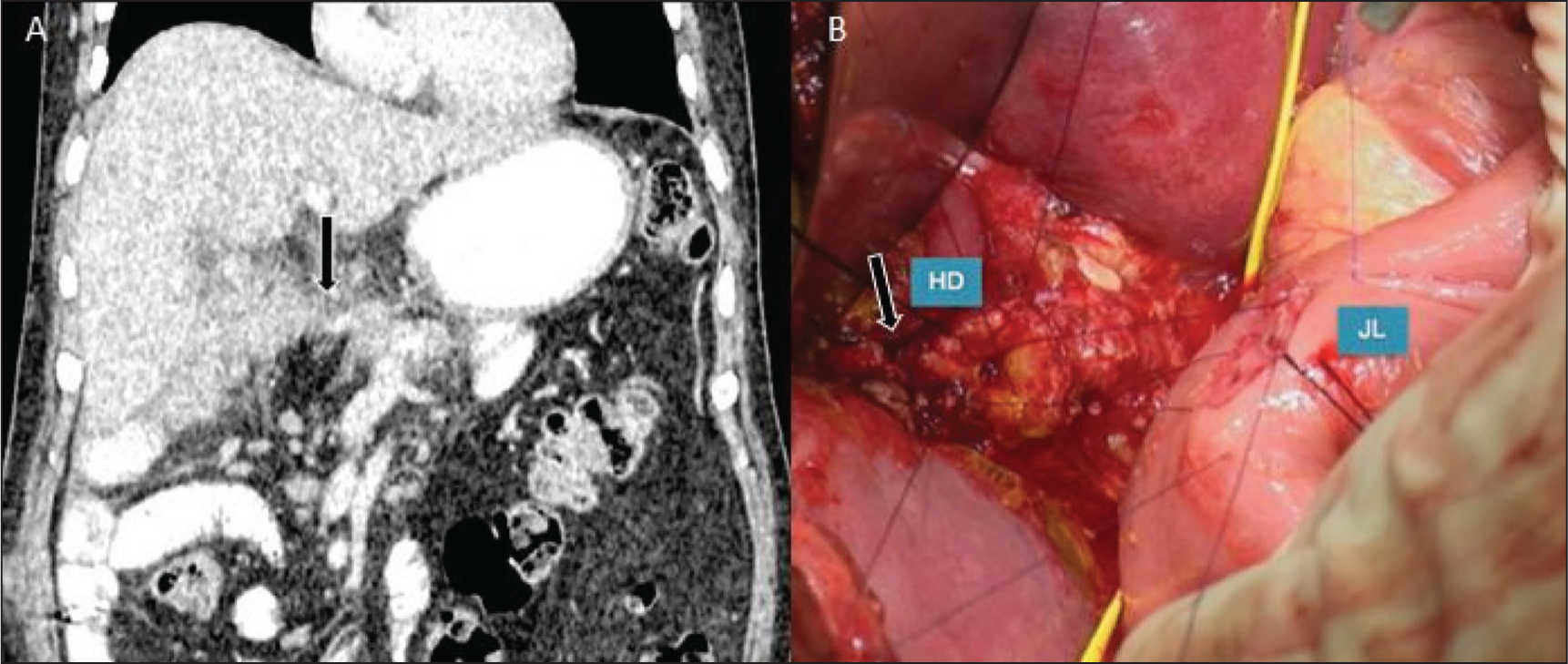
The presence of pneumobilia is the most common finding in the post-operative period.[5] It serves as a valuable tool in locating the site of biliary-enteric anastomosis. The pneumobilia can be traced to reach the jejunal loop anastomosed with the hepatic/CBD. Often, a collapsed jejunal loop can be mistaken for a haematoma or tumour recurrence. Sometimes a radio-opaque stent extending from the jejunum to the hepatic/CBD can enable the radiologist to identify the exact site of biliary-enteric anastomosis [Figure 2]
Coronal MDCT (A) and Intra-operative image (B) showing the anastomosis (black arrow) between hepatic duct (HD) and jejunum (JL)—the hepaticojejunostomy site.
Gastro-jejunostomy/Duodeno-jejunostomy Site (GJ Site)
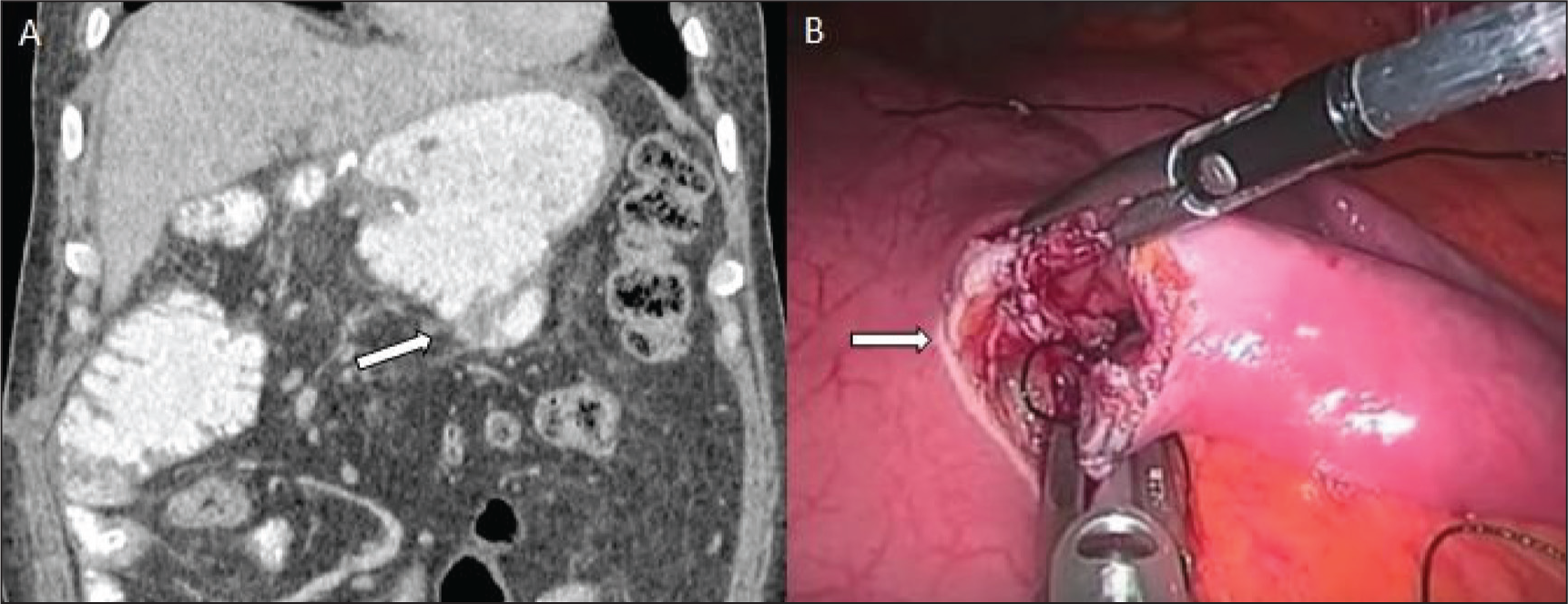
The jejunal loop is anastomosed with the stomach in the classic variant of Whipple surgery and with the first part of the duodenum in the pylorus-preserving variant of Whipple surgery. The site of GJ is seen anterior and to the right of the remnant pancreas, whereas the duodeno-jejunostomy site is usually located in the right upper quadrant of the abdomen. Both these sites of entero-enteric anastomoses can be visualised easily with adequate distension using oral contrast. Many times, the suture line/staple line can be seen as radiopaque linear opacities [Figure 3].
Coronal MDCT (A) and Intra-operative image (B) showing the anastomosis (white arrow) between stomach and jejunum—the gastrojejunostomy site
Jejuno-jejunostomy Site
Jejuno-jejunostomy (JJ) anastomosis involves suturing of two loops of jejunum together, resulting in a combined wider lumen. The site of jejuno-jejunal anastomosis can be easily appreciated after giving oral contrast, which obtains the necessary bowel distension. One must be careful not to mistake the site of jejuno-jejunal anastomosis for a focally dilated bowel loop and hence bowel obstruction.
Acute Post-operative Findings
A number of findings in the immediate post-operative period are a result of surgery, not requiring any aggressive intervention and should not be regarded as complications of surgery. These include pneumoperitoneum, Fluid collections and inflammatory fat stranding in the post-operative bed, oedema at the anastomotic sites, lymphadenopathy, perivascular cuffing, pneumobilia, drainage catheters and feeding jejunostomy tubes. Thin-walled or poorly defined fluid collections can be seen in the early post-operative period in up to 28.5% cases.[6] These rarely require intervention and resolve spontaneously in the majority of cases. Pneumobilia, that is, air in the biliary tree with mild intrahepatic biliary radical dilatation as well as air in pancreatic duct, is seen in up to 67%-80% of cases.[5,6] Thickening and oedema, particularly at the anastomotic sites, can result in varying appearances; oedema at the PJ site may manifest as dilatation of the pancreatic duct, mild dilatation of intrahepatic biliary radicals is often seen due to oedema at the HJ site, and it should not lead to a diagnosis of biliary-enteric stricture. Multiple drainage catheters and feeding tubes are seen in post-operative scans. These need to be assessed for their position and continuity; therefore, one must mention the location of the tip for all catheters/tubes and check for any break or kink in any catheter/tube.
Chronic Post-operative Findings
Most of the inflammatory changes and oedema tend to resolve by 3–6 months after surgery. There are a few imaging findings which persist longer, and awareness about them is necessary to prevent unnecessary interventions. Thickening around the GJ site is seen to persist, and does not indicate any infection /enteritis. Mild dilatation of the intrahepatic biliary radicals and pancreatic duct can be seen for a long time after surgery and should be considered a normal finding. Only the presence of significant dilatation or progressive dilatation should raise a suspicion of tumour recurrence or stricture at the anastomotic site.
Complications
Pancreatic Fistula
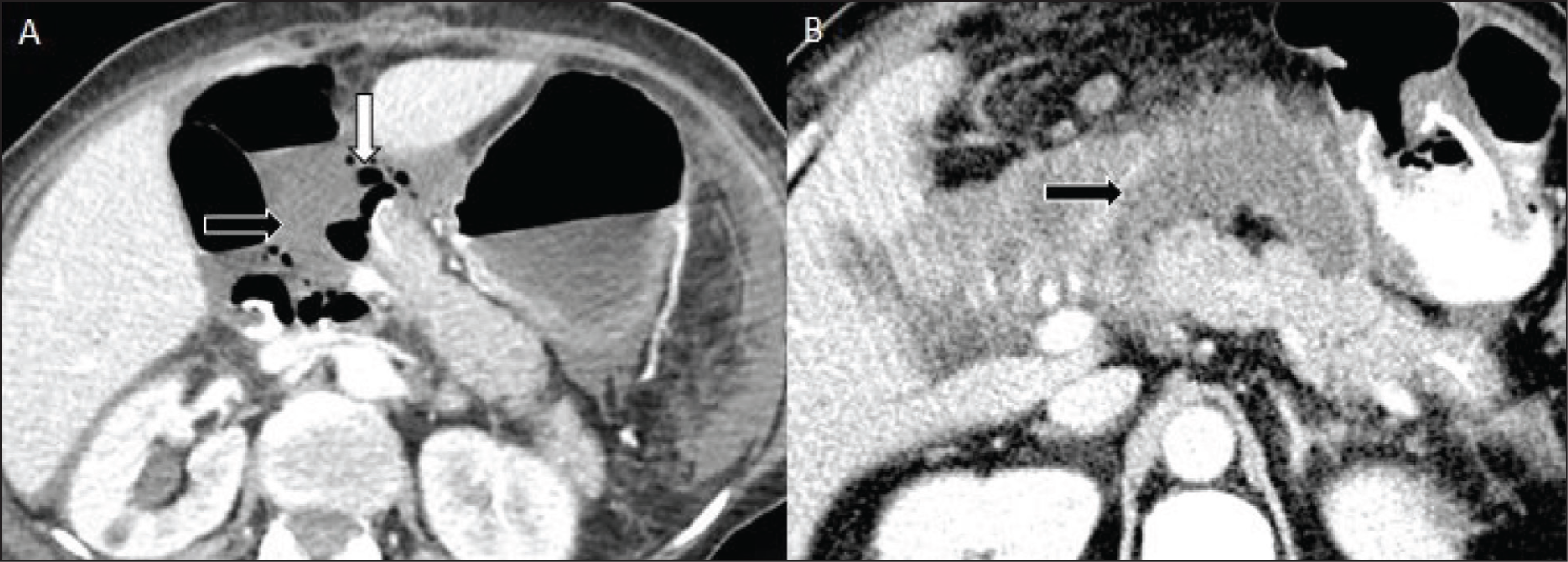
Pancreatic fistula is a frequent complication seen in about 10%-30% of patients who undergo the Whipple procedure.[7] It is one of the leading causes of increased morbidity and mortality in such patients, and therefore, it becomes necessary for a radiologist to identify pancreatic fistula on imaging. Classically, the ISGPF (International Study Group of Pancreatic Fistula) defines a pancreatic fistula as the presence of amylase content greater than three times the upper limit of normal serum value in the drainage fluid on the third post-operative day or later.[8] Various imaging features on CT can help a radiologist raise a possibility of pancreatic fistula, such as fluid collections around the pancreaticojejunostomy site or pancreatic resection margins, particularly in communication with the pancreatic duct or suture line; foci of air in peripancreatic collection and breakdown of the pancreatic anastomosis[1,7] [Figure 4]. Many factors increase the likelihood of pancreatic fistula, notably among them are small-calibre pancreatic duct, soft texture of pancreatic parenchyma and degree of intra-operative blood loss. Early recognition of this complication can significantly improve the patient’s outcome.
Axial (A, B) MDCT images showing a fluid collection (black arrow) adjacent to the pancreaticojejunostomy site with a few air foci (white arrow) within s/o pancreatic fistula
Leak at anastomotic site:
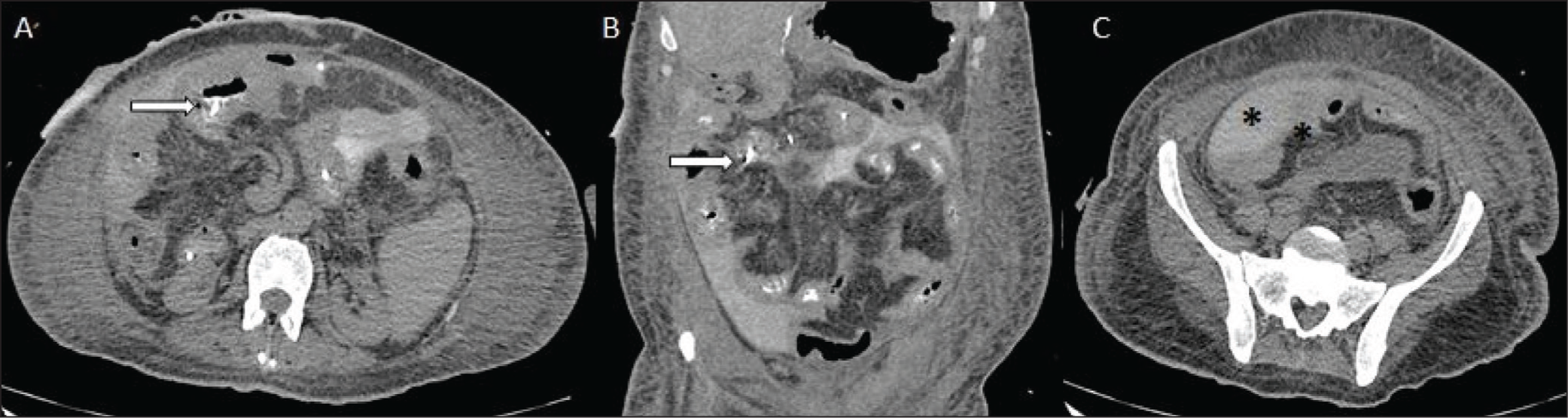
At the GJ/JJ site: Leaks at the GJ/JJ site are rare complications after the Whipple procedure. However, the occurrence of anastomotic leaks can result in adverse patient outcomes. Several factors contribute to anastomotic leaks, the most important being faulty surgical technique by the surgeon and compromised blood flow to the anastomotic site. On CT, when using neutral oral contrast, one can find fluid collections adjacent to GJ or JJ sites. Positive oral contrast is superior to neutral oral contrast in diagnosing anastomotic leaks, which are seen as direct extravasation of oral contrast from the site of anastomosis [Figure 5]. At the biliary-enteric anastomotic leaks are rare in comparison to GJ leaks. Most often, they present as collections around the biliary-enteric anastomotic site; however, the close proximity of the PJ and GJ anastomosis can pose a problem, and one may not be able to determine the definitive site of the leak. An important clue to the diagnosis of biliary leak is the presence of elevated bilirubin levels compared to serum levels in the surgical drain during the early post-operative period. Apart from CT, the use of hepatobiliary scintigraphy and MRI with hepatocyte-specific agents can aid in the definitive diagnosis of biliary-enteric anastomotic leak.[1]
Axial (A, C) and coronal (B) Non-contrast images show nasogastric tube tip outside the jejuno-jejunostomy site (white arrow) with extravasation of oral positive contrast from the anastomotic site seen as dense contrast material (black star) in the pelvis s/o anastomotic leak
Anastomotic Stricture
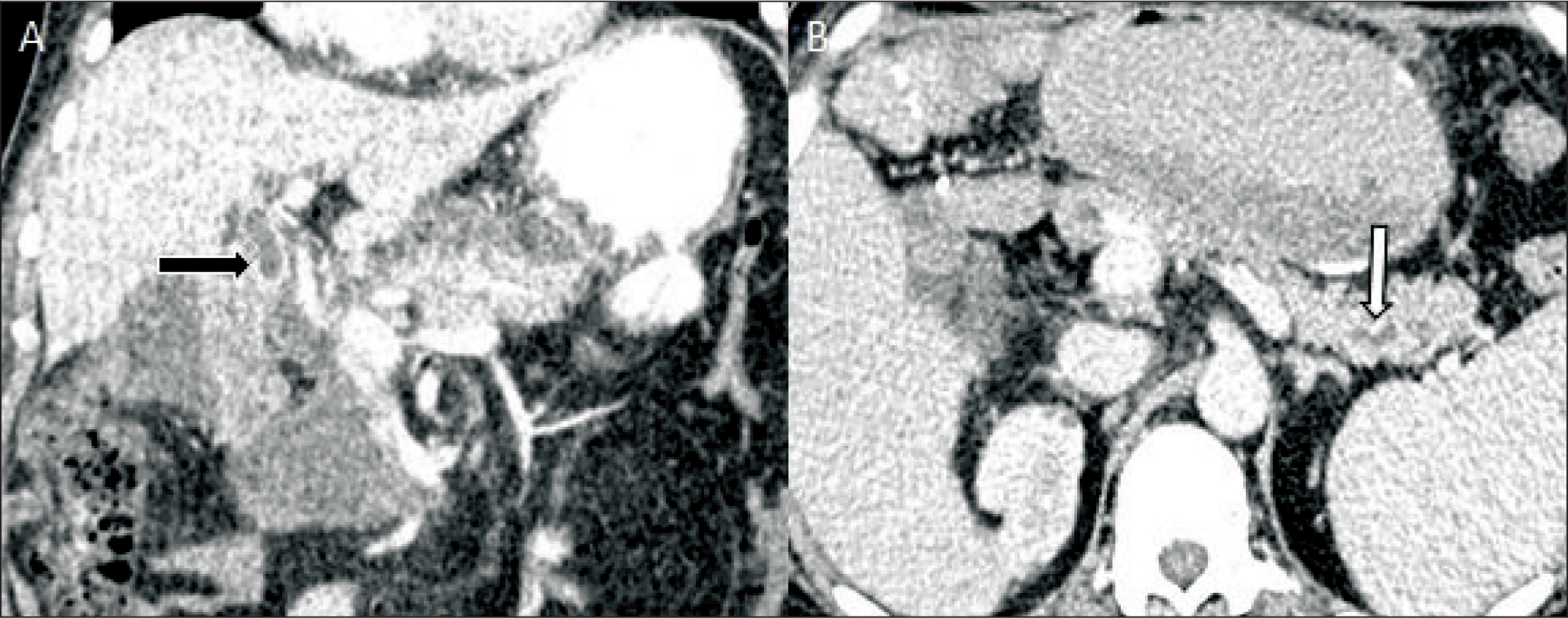
Anastomotic strictures at hepaticojejunostomy and pancreaticojejunostomy sites are late complications, which usually occur 2–5 years after the Whipple procedure.[1] On imaging, progressive dilatation of intrahepatic biliary radicals and the pancreatic duct is the single most important clue to diagnose anastomotic site stricture [Figure 6]. However, apart from anastomotic strictures, progressive dilatation of intrahepatic radicals and pancreatic duct can result from tumour recurrence in the post-operative bed, and one must rule it out before diagnosing a stricture.
Coronal (A) and axial (B) MDCT images showing dilatation of biliary radicals (black arrow) and remnant pancreatic duct (white arrow) s/o anastomotic stricture at HJ and PJ anastomosis
Abscesses
Intra-abdominal abscesses in post-Whipple patients can be attributed to various causes, secondary to superinfection in an existing post-operative collection or hepatic infarct; pancreatic fistula; leak from hepaticojejunostomy, gastrojejunostomy or jejunojenjunostomy anastomotic site. The overall incidence of post-operative abscess is estimated to be around 6%.[1,6,9] On CT, abscesses are seen as peripherally enhancing thick-walled collections with or without the presence of air foci within.
Conclusion
Whipple procedure is a complex surgery associated with three major anastomoses, namely pancreaticojejunostomy, hepaticojejunostomy and gastrojejunostomy. A large number of complications which occur in the post-operative period involve these anastomotic sites. Cross-sectional imaging using an optimal scanning protocol plays a pivotal role in identifying these complications and offers optimal treatment options. Knowledge about the normal post-operative anatomy and normal post-operative appearance is necessary to avoid misinterpretations and unnecessary interventions.
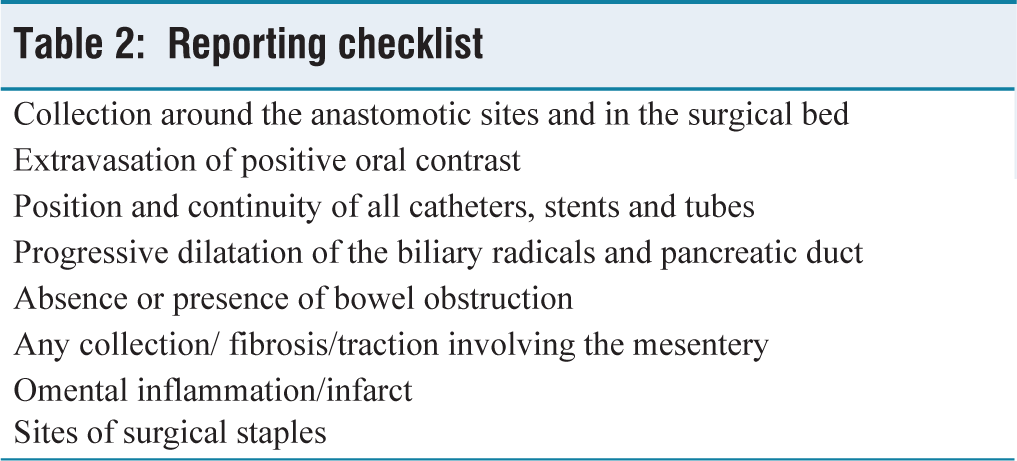
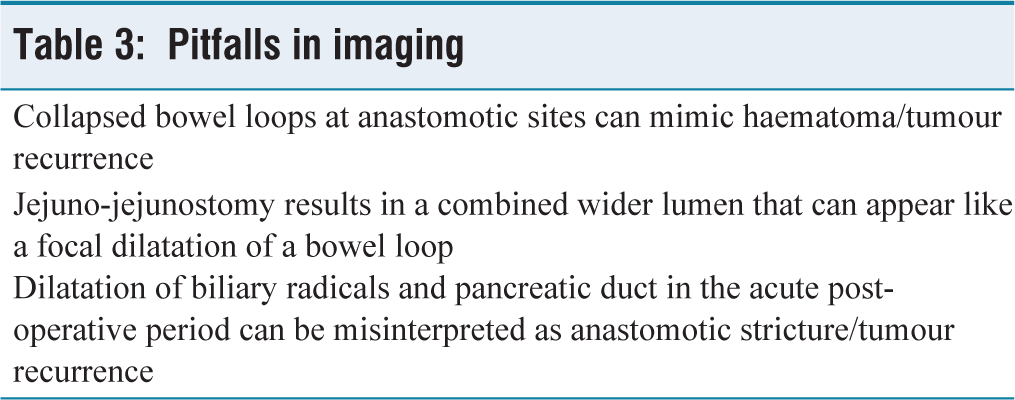
The imaging checklist [Table 2] and common pitfalls on imaging [Table 3] are tabulated at the end.
Reporting checklist
Pitfalls in imaging
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
N/A.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Credit author statement
Data availability
The data is confidential or available upon request. The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Use of artificial intelligence
No AI tools were used in the preparation of this manuscript.