
Abstract
Background and Aims:
Prehabilitation aims to enhance a patient’s physiological reserve before surgery, thereby improving postoperative outcomes. Despite the adoption of Enhanced Recovery After Surgery protocols, complications remain prevalent following major abdominal procedures. This prospective observational study evaluates the impact of structured exercise and nutritional support on post-operative outcomes in patients undergoing major abdominal surgery.
Patients and Methods:
A total of 35 patients scheduled for elective major abdominal surgery at a tertiary centre were enrolled between December 2019 and September 2021. The prehabilitation program included individualised aerobic and resistance training, nutritional optimisation and psychological support. Functional capacity was assessed using the 6-minute walk test (6MWT) pre-operatively and 4 weeks post-operatively. Secondary outcomes included complications (Clavien-Dindo classification), length of hospital stay, readmissions, psychological status (HADS) and quality of life (Stark score).
Results:
The mean age was 58.9 years, with 54.3% male participants. Pulmonary complications occurred in 31.4%, with no mortality. Median HADS scores showed significant reductions in both anxiety (P = .041) and depression (P = .046). Quality of life improved post-operatively (P = .032), and 6MWT values improved marginally without statistical significance (P = .64). There was no significant difference in 6MWT based on ASA grade, gender or Clavien-Dindo class.
Conclusion:
A structured multimodal prehabilitation program incorporating physical, nutritional and psychological components is feasible and beneficial in improving mental well-being and preserving functional capacity post-surgery. Although differences in physical recovery were not statistically significant, prehabilitation appears to positively influence overall recovery and patient-reported outcomes. Further large-scale trials are warranted to confirm its efficacy and standardise protocols.
Introduction
Major abdominal surgery is frequently associated with substantial physiological stress, often resulting in a high incidence of post-operative complications, including pulmonary, cardiovascular and infectious events. These complications contribute significantly to prolonged hospitalisation, delayed recovery, increased healthcare costs and reduced quality of life in the post-operative period.[1–3] Furthermore, patients experiencing post-operative complications have demonstrated reduced long-term survival, even in the absence of life-threatening events.[4]
Over the past decade, surgical care has advanced considerably with the introduction of Enhanced Recovery After Surgery (ERAS) protocols, improved anaesthetic techniques and multidisciplinary peri-operative management strategies.[5–7] While these measures have collectively reduced surgical stress and improved outcomes, a considerable proportion of patients still face suboptimal recovery trajectories, particularly those with compromised pre-operative physiological reserves.[8]
One promising strategy that shifts focus from reactive to proactive peri-operative care is prehabilitation. Defined as a process of enhancing a patient’s functional capacity before surgery, prehabilitation involves a structured program of exercise, nutritional optimisation and psychological support aimed at improving resilience to surgical stress.[9–11] The underlying rationale is that improved baseline fitness levels enable patients to better withstand intra-operative challenges and accelerate post-operative recovery.[12]
Prehabilitation programs often leverage the ‘surgical waiting period’—a window between diagnosis and operative intervention—as an opportunity to deliver targeted interventions.[13] This period represents a ‘teachable moment’ where patients are most receptive to behavioural modification and are often in a better physical and psychological state to participate in optimisation efforts.[14] Several studies have shown that structured prehabilitation, particularly when delivered in a multimodal fashion, can reduce post-operative complications, enhance early functional recovery and improve health-related quality of life.[15–17]
Despite encouraging evidence from international literature, the application and evaluation of prehabilitation strategies in the Indian population remains limited. Patient-related barriers such as compliance, awareness, socioeconomic constraints and heterogeneity of interventions pose additional challenges in standardising and scaling prehabilitation efforts.[18–19] Moreover, existing studies are often limited by small sample sizes, methodological inconsistencies and lack of long-term follow-up.[20]
To address these gaps, we conducted a prospective observational study to evaluate the feasibility and impact of a structured prehabilitation program comprising individualised physical exercise, nutritional counselling and psychological support in patients scheduled for major abdominal surgery at a high-volume tertiary care centre in India. The primary objective was to assess changes in functional capacity as measured by the 6-minute walk test (6MWT) before and after surgery. Secondary objectives included evaluating the incidence of post-operative complications, length of hospital stay, psychological well-being and quality of life.
Materials and Methods
Study Design and Setting
This was a prospective observational study conducted between December 2019 and September 2021 in the Department of Surgical Gastroenterology of a Tertiary hospital, New Delhi, a tertiary referral centre for complex gastrointestinal surgeries.
Study Population
A total of 35 adult patients scheduled for elective major abdominal surgery were enrolled. All participants provided written informed consent prior to inclusion.
Inclusion Criteria
Age 18–80 years
Patients undergoing major elective abdominal surgery (including colonic, hepatobiliary or pancreatic resections)
Candidates undergoing neoadjuvant chemotherapy
Availability of at least 2 weeks between scheduling and surgery for the prehabilitation protocol
Exclusion Criteria
Emergency or non-elective surgeries
Hemodynamic instability or critical illness
Unstable cardiopulmonary diseases
Cognitive impairment precluding adherence
Locomotor limitations precluding physical activity
Unwillingness or lack of motivation for participation in prehabilitation
Prehabilitation Protocol
The program comprised structured and supervised aerobic and resistance training, nutritional support and psychological assessment.
Initial Assessment
Conducted in the outpatient setting by a multidisciplinary team comprising a surgeon, physiotherapist and dietitian. Baseline functional status was assessed using the 6MWT, Hospital Anxiety and Depression Scale (HADS) and Stark Quality of Life questionnaire.
Aerobic and Resistance Training
An individualised exercise plan was prescribed based on the patient’s age, comorbidities and baseline functional capacity. Aerobic training (walking) was performed 30 minutes daily; resistance training using Thera Bands was conducted 3–4 times per week. Exercise intensity was monitored using a pedometer, pulse rate monitor and the Borg Scale of perceived exertion.
Nutritional Optimisation
Nutritional counselling was provided as per ESPEN guidelines to ensure a daily protein intake of 1.2 g/kg/day. Dietary patterns were reviewed and protein supplementation was provided where required.
Psychological Support
Psychological status was monitored using HADS. Regular telephonic follow-up and weekly counselling sessions were conducted to reinforce adherence.
Peri-operative and Post-operative Management
Patients were encouraged to continue exercises until 24 hours before surgery. During the hospital stay, post-operative exercises were supervised. Upon discharge, patients followed a structured home-based program for 4 weeks.
At 4 weeks post-operatively, patients returned for follow-up, during which repeat assessments were performed using:
6MWT HADS Stark Quality of Life questionnaire Documentation of post-operative complications using the Clavien-Dindo classification
Outcome Measures
Primary Outcome
Change in functional capacity (measured by 6MWT) between pre-operative baseline and 4 weeks post-surgery
Secondary Outcomes
Post-operative complications (type and severity)
Clavien-Dindo classification of complications
Length of hospital stay
30-day readmission and emergency department visits
Quality of life (Stark score)
Psychological well-being (HADS)
Sample Size Justification
Based on an anticipated standard deviation of 35 m for 6MWT and an expected minimum detectable difference of 25 m, the study required a minimum of 31 participants for 80% power at a 5% significance level.
Sample size formula:

Statistical Analysis
Data were analysed using SPSS version 22.0. Continuous variables were expressed as mean ± standard deviation (SD) or median with interquartile range (IQR) as appropriate. Paired t-tests were used to compare pre- and post-intervention outcomes. A P value <.05 was considered statistically significant.
Results
Demographic Profile
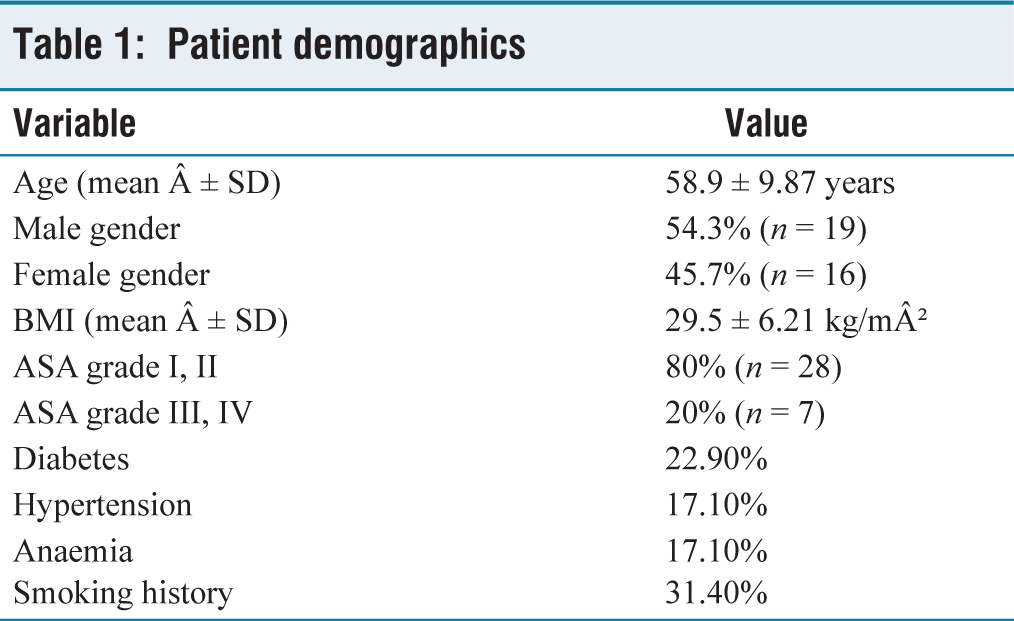
A total of 35 patients were included in the study. The mean age was 58.9 ± 9.87 years, with the majority (60%) in the 50- to 60-year age group. Male patients comprised 54.3% of the cohort (n = 19), while 45.7% were female (n = 16). The baseline characteristics of the study population are shown in Table 1.
Patient demographics
ASA Grade and Comorbidity Burden
Most patients were classified as ASA Grade I-II (80%), with the remainder (20%) under ASA Grade III-IV. The median Charlson Comorbidity Score was 3 (IQR: 2–4). The most prevalent comorbidities included diabetes (22.9%), hypertension (17.1%) and anaemia (17.1%). Smoking history was present in 31.4% of the patients.
Nutritional and Functional Baseline
The mean BMI was 29.5 ± 6.21 kg/m² and the mean lean body mass was 46.6 ± 7.92 kg. Baseline haemoglobin was 11.89 ± 2.46 g/dL, and serum albumin was 3.86 ± 0.41 g/dL. The mean baseline 6MWT distance was 318.76 ± 107.37 m.
Intra-operative Parameters
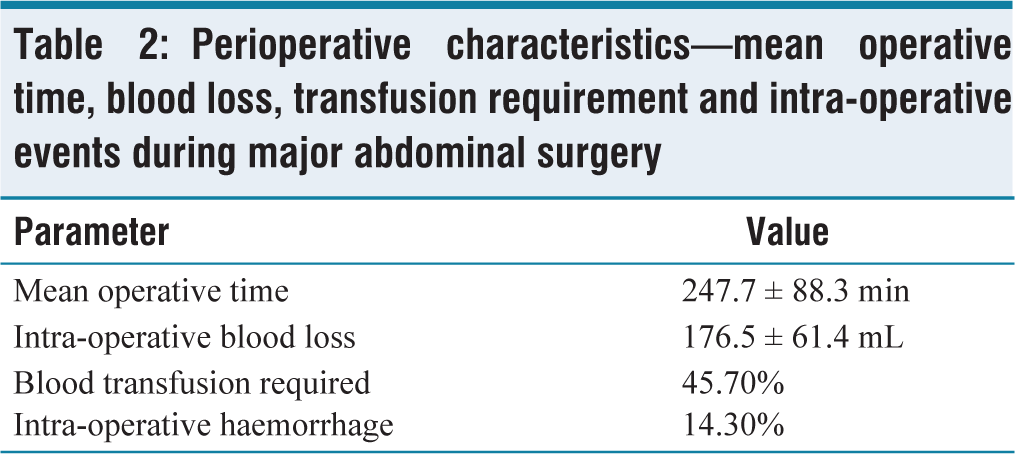
The mean operative time was 247.7 ± 88.3 minutes, and the mean intra-operative blood loss was 176.5 ± 61.4 mL. Blood transfusion was required in 45.7% of patients, and haemorrhage occurred in 14.3%. The mean operative time, blood loss, and intra-operative events are detailed in Table 2.
Perioperative characteristics—mean operative time, blood loss, transfusion requirement and intra-operative events during major abdominal surgery
Post-operative Complications and Recovery
Post-operative complications were observed in 42.9% of patients, with pulmonary complications (e.g., atelectasis, effusion, consolidation) accounting for 31.4%. Post-operative pneumonia was seen in 5.7%, and there were no mortalities. The mean hospital stay was 11.14 ± 10.43 days. The 30-day readmission rate was 5.7%, and emergency department visits occurred in 8.6%.
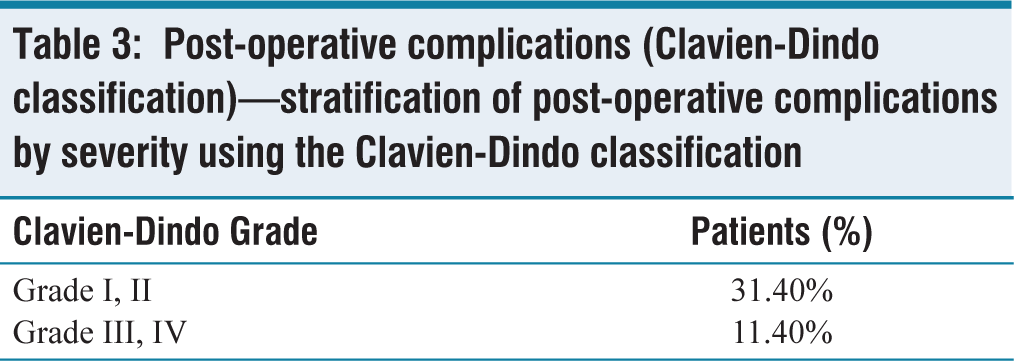
Based on Clavien-Dindo classification, Grade I-II complications were recorded in 31.4%, while Grade III-IV complications were reported in 11.4% of cases. The distribution of post-operative complications according to Clavien-Dindo classification is presented in Table 3.
Post-operative complications (Clavien-Dindo classification)—stratification of post-operative complications by severity using the Clavien-Dindo classification
Functional and Psychological Outcomes
There was a modest increase in the 6MWT score post-operatively (324.51 ± 89.78 m) compared with baseline, though not statistically significant (P = .64).
Subgroup analyses showed:
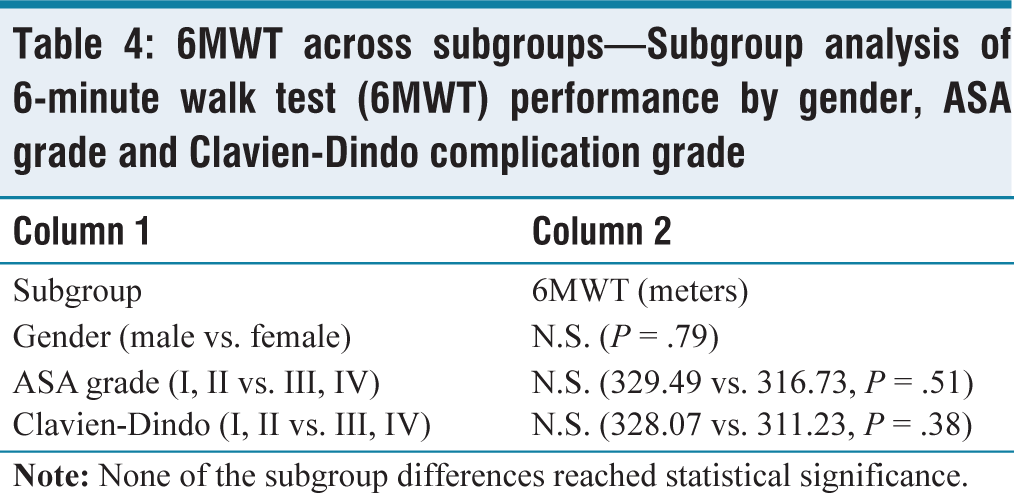
No significant difference in 6MWT between genders (P = .79) Higher, though non-significant, 6MWT in ASA I-II compared with III-IV (329.49 vs. 316.73 m; P = .51) Higher 6MWT scores in patients with Clavien-Dindo Grade I-II compared with III-IV (328.07 vs. 311.23 m; P = .38). Subgroup analysis of 6MWT across gender, ASA grade, and complication severity is summarised in Table 4.
6MWT across subgroups—Subgroup analysis of 6-minute walk test (6MWT) performance by gender, ASA grade and Clavien-Dindo complication grade
Quality of Life and Psychological Impact
Significant improvements were observed in:
Hospital Anxiety and Depression Scale
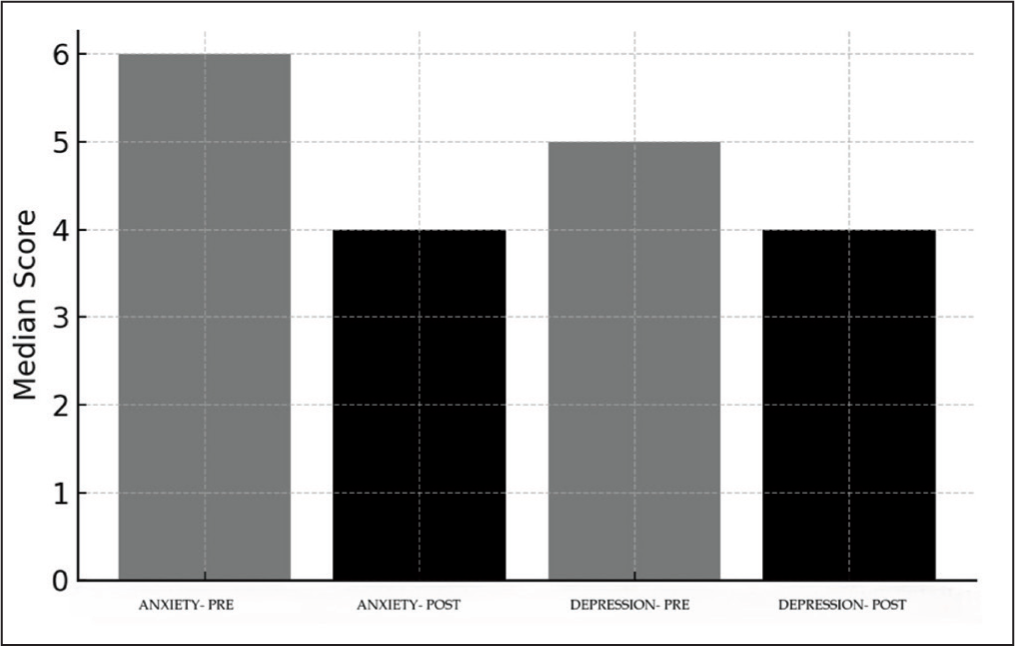
Depression: median decreased from 5 (IQR 3–8) to 4 (IQR 2–5.5) (P = .046)
Anxiety: median reduced from 6 (IQR 4–9) to 4 (IQR 2–5) (P = .041). Figure 1 illustrates the statistically significant reduction in anxiety and depression scores.
HADS scores pre versus post—change in hospital anxiety and depression scale (HADS) scores before and 4 weeks after surgery. Both anxiety and depression scores showed statistically significant improvement
Stark Quality of Life Score
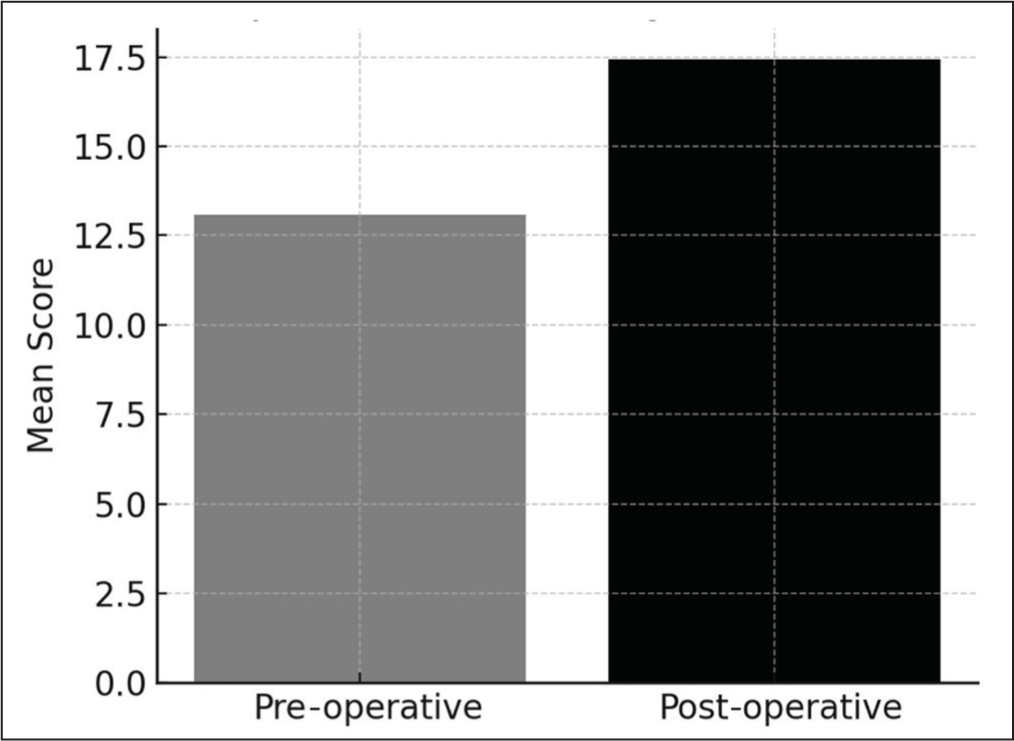
Improved significantly from 13.09 ± 3.58 at baseline to 17.42 ± 4.21 at 4 weeks (P = .032). As shown in Figure 2, Stark quality of life scores improved significantly following prehabilitation.
Stark quality of life score—comparison of mean stark quality of life scores pre- and post-operatively, demonstrating significant enhancement post-intervention
Perceived Exertion: Borg Scale
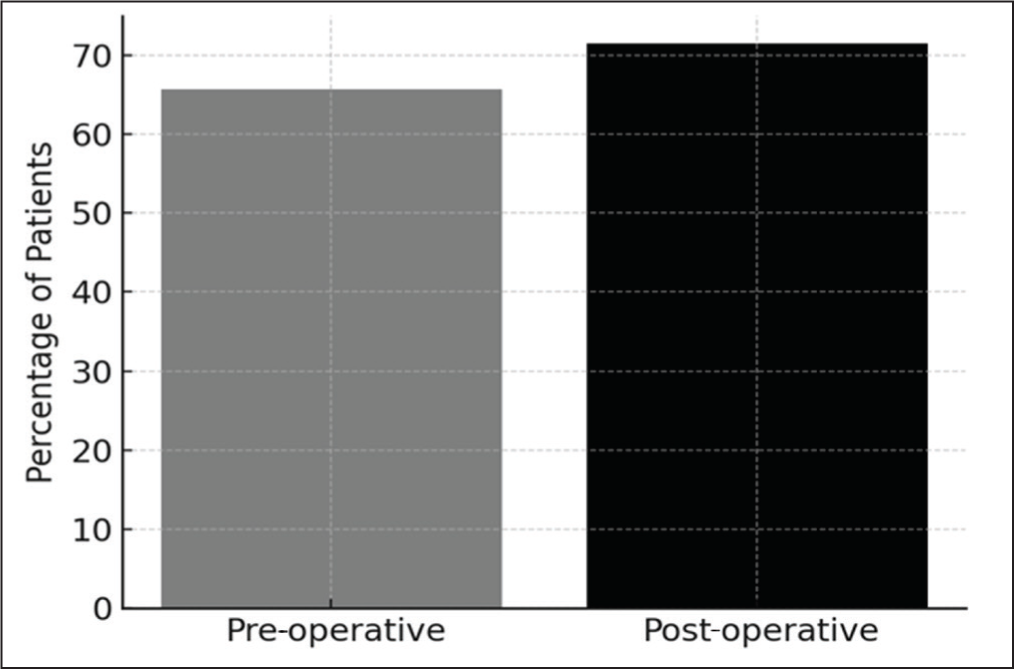
At baseline, 65.7% of patients reported mild exertion (Borg score 0–2). After 4 weeks, this increased to 71.4%, although the difference was not statistically significant (P = .78). Figure 3 demonstrates the trend toward improved perceived exertion on the Borg scale.
Borg scale—mild exertion (%)—Percentage of patients reporting mild exertion (Borg score 0–2) before and after surgery. A trend toward improved subjective exertion was observed
Discussion
This prospective observational study evaluated the impact of a structured, multimodal prehabilitation program—comprising exercise, nutrition and psychological support—on patients undergoing major abdominal surgery. Our findings suggest that prehabilitation is a feasible intervention with positive effects on patient-reported outcomes, mental well-being and maintenance of functional capacity, although improvements in physical metrics such as 6MWT were not statistically significant.
Functional Capacity and Physical Recovery
The pre- and post-operative 6MWT values in our study (318.76 vs. 324.51 m; P = .64) were maintained despite surgical stress. This echoes findings from previous studies such as Barberan-Garcia et al. and Bousquet-Dion et al., where prehabilitation stabilised or modestly improved physical capacity in the perioperative period.[1,2] While randomised trials like that of Carli et al. have reported variable outcomes, our results reinforce the value of maintaining baseline functionality, especially in high-risk patients.[3]
Post-operative Complications and Hospital Stay
The overall complication rate in our cohort was 42.9%, with pulmonary events constituting the largest proportion (31.4%). These figures align with the rates reported in international prehabilitation trials, including those by Kamarajah et al. and Howard et al., who demonstrated reduced pulmonary and major complications following pre-operative optimisation.[4,5] Although our study lacked a control group for direct comparison, the observed complication spectrum and mean hospital stay (11.1 days) were consistent with established ERAS-era benchmarks.
Psychological Impact and Quality of Life
Statistically significant improvements were observed in HADS depression (P = .046) and anxiety scores (P = .041), along with the Stark quality of life score (P = .032) post-operatively. These results highlight the psychological benefits of structured prehabilitation, supporting the assertion by Gilles et al. that enhanced engagement during the pre-operative window can reduce anxiety and improve peri-operative self-efficacy.[6] Weekly telephonic follow-ups and personalised counselling were instrumental in reinforcing adherence and may have contributed to these findings.
Clinical and Economic Relevance:
The reduction in post-operative readmissions (5.7%) and absence of mortality in our series align with data from programs such as the Michigan Surgical and Health Optimisation Program, where structured prehabilitation led to improved intra-operative physiology and lower overall costs.[5] With rising surgical volumes and pressure on hospital resources, such interventions offer an opportunity to enhance recovery while minimising expenditure.
Comparison With Literature
Several systematic reviews have attempted to consolidate the efficacy of prehabilitation. Moran et al. demonstrated decreased complication rates but inconclusive effects on hospital stay, mirroring our experience.[7] Meanwhile, Thomas et al. and Daniels et al. emphasised the heterogeneity of prehabilitation programs, calling for standardisation and identification of ideal candidates.[8,9] Our study reinforces the potential of prehabilitation, particularly when multimodal and personalised.
Following initial promising findings, we have proactively continued patient recruitment, aiming to double the current cohort within the subsequent year. This expansion aims to enhance statistical precision, validate the observed trends in physical recovery and more robustly establish clinical efficacy. Further interim analyses will be periodically conducted to monitor progress and outcomes rigorously.
Limitations
This study has inherent limitations. First, the absence of a control group limits comparative inference. Second, the small sample size, although statistically powered, may not capture rarer complications. Third, the short post-operative follow-up (4 weeks) may underestimate the long-term benefits of prehabilitation. Finally, the relatively short duration of prehabilitation (2 weeks) may not have allowed full physiological conditioning.
One important limitation of our study is the relatively small sample size (n = 35). While the sample size was calculated based on statistical requirements for the primary outcome measure, it might still be insufficient to robustly assess secondary outcomes and detect less pronounced yet clinically meaningful differences. Thus, caution is warranted in generalising these findings, and future studies should aim for larger cohorts.
Strengths and Practical Implications
Despite these limitations, this is one of the few Indian studies to prospectively evaluate a structured prehabilitation protocol in major abdominal surgery. The program was implemented without resource-intensive infrastructure and demonstrated high compliance, suggesting potential for scalable adoption. Moreover, psychological and quality-of-life benefits, often underreported, emerged as prominent outcomes.
Conclusion
Prehabilitation represents a promising paradigm shift in the perioperative management of patients undergoing major abdominal surgery. Our study demonstrates that a structured, multimodal prehabilitation program—encompassing individualised physical training, nutritional optimisation and psychological support—is both feasible and effective in improving patient-reported outcomes, preserving functional capacity and enhancing mental well-being in the Indian surgical population. While improvements in objective physical performance metrics such as the 6MWT were modest, significant benefits were observed in terms of anxiety, depression and quality of life. These findings highlight the broader impact of prehabilitation beyond physiological conditioning.
Although this study provides preliminary evidence supporting structured prehabilitation’s benefits, its observational nature precludes definitive conclusions regarding comparative effectiveness. Hence, future research must focus on randomised controlled trials directly comparing structured multimodal prehabilitation with standard perioperative management. Such studies will robustly validate our findings and guide evidence-based clinical practices.
Footnotes
Acknowledgements
We thank the Department of Dietetics and the Department of Physiotherapy, Indraprastha Apollo Hospital, New Delhi, for their unwavering support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Ethics Committee of Indraprastha Apollo Hospitals.
Credit author statement
Supreet Kumar: Conceptualisation, Methodology, Writing, Review and editing, Formal analysis.
Aishwarya S. Bhalerao: Literature review, manuscript drafting, Project administration, Correspondence.
Sherry Prabhakar: Physiotherapy and outcome assessment, Data curation, Clinical support.
Kiran Verma: Data collection, Validation, Clinical support, Project administration.
Vivek Tandon: Supervision, Manuscript editing.
Deepak Govil: Supervision, critical revision of final draft.
All authors have read and approved the final manuscript.
Data availability
The data supporting the findings of this study are available from the corresponding author on reasonable request. Due to patient confidentiality and institutional policy, individual-level data cannot be made publicly accessible.
Use of artificial intelligence
No generative artificial intelligence (AI) tools were used in the writing, editing, data analysis, or figure/table preparation for this manuscript. All content was produced by the authors.