
Abstract
Coronary artery disease is one of the main causes of mortality and morbidity among chronic heart diseases worldwide. Patients reported chronic chest pain as the primary symptom of coronary artery disease. Due to its progressive nature, it affects the health status and functional capacity of the patients. The current study was planned to compare the effects of prehabilitation resistance training in mild to moderate clinically frail patients awaiting coronary artery bypass graft (CABG). A randomized controlled trial was conducted on 74 patients awaiting CABG at the Faisalabad Institute of Cardiology, Faisalabad, Pakistan. A Modified Healthy Heart Questionnaire was used for screening of the patients. Interventions applied were resistance training by using cuff weights/dumbbells at light intensity (40%–50%) of a maximum of one repetition (10–15 repetitions for one to three times a day) per major muscle groups of upper and lower limbs of the body on weekly basis. The main outcome measures were the 6-minute walk test (6MWT), the New York Heart Association (NYHA) for heart failure, the clinical frailty score, and the essential frailty toolset. Significant differences between group A (resistance training group) and group B (conventional physical therapy group) patients were observed. The mean ranks for 6MWT in group A and group B were 1.70 and 1.55, respectively. The mean ranks of NYHA in group A and group B were 1.68 and 2.84, respectively. Clinical frailty scores in group A and group B were 2.68 and 2.74, respectively, with the essential frailty toolset in group A and group B were 1.14 and 1.11, respectively. There were significant (p < 0.05) differences within and between groups for prehabilitation resistance training after CABG. The study showed that the resistance training group had improved the clinical frailty score, strength, endurance, and functional capacity in patients who underwent elective CABG.
In ischemic heart disease, the surgeon often bypasses the stenotic segment of the coronary arteries using the patient’s long saphenous vein and internal mammary artery. Most commonly on-pump coronary artery bypass graft (CABG) is done. In mild to moderate clinically frail patients, multiple issues have a combined effect on the patient’s health. The adverse outcomes of higher risk who are exposed to stressors have a negative impact on patients due to loss of physiological reserve and compliance.
Prehabilitation resistance training improved the functional capacity through a 6-minute walk test and NYHA class in the resistance training group of the coronary artery disease patients awaiting CABG.
To facilitate the management of heart patients awaiting CABG through prehabilitation resistance training.
Introduction
Ischemic heart disease (IHD) is a common pathology in which patients present with severe chest pain, shortness of breath, palpitations, or syncope. 1 Diabetes mellitus, smoking, hyperlipidemia, hypertension, and family history are the established risk factors for IHD. 2 Diagnosis is often by clinical symptoms followed by numerous investigations. Coronary artery bypass surgery is a major surgical intervention in which median sternotomy is done. 3
In IHD, the surgeon often bypasses the stenotic segment of the coronary arteries using the patient’s long saphenous vein and internal mammary artery. The left internal mammary artery (LIMA) is very commonly used for grafting the left anterior descending artery because of the very high long-term patency rate of LIMA. 4 Clinical frailty is defined as a clinically recognizable state of increased vulnerability as a result of the age-associated decrease in physiologic reserve and function across multiple organ systems such as acute stressors or the ability to cope with everyday stresses. 5
In mild to moderate clinically frail patients, multiple issues have a combined effect on the patient’s health. The adverse outcome of higher risk who are exposed to stressors has a negative impact on patients due to the loss of physiological reserve and compliance. 6 There is no gold standard definition of frailty to encompass the various domains of frailty syndrome but it includes mobility, physical activity, strength, energy, independence, and lifestyle modifications. 7 By adjusting the routine risk scoring system, frailty was associated with 2- to 6-fold increased risks of adverse cardiovascular events, prolonged hospital stay, and in-hospital mortality risks in cardiac surgery. 8
Due to poor frailty and higher risk of complications which may lead to mortality, the total hospital stay was high in cardiac surgery patients. Coronary artery disease is the leading cause of death worldwide. 9 After CABG, altered mechanics that occur after median sternotomy and cardiopulmonary bypass invariably result in pulmonary interstitial edema which adds to respiratory difficulties. 10
The improved clinical frailty score was not evident in other relevant studies on these patients. In present-day practice, the increasing age also results in increasing frailty scores. Further research is needed to study the changes in the overall perioperative care of patients undergoing CABG. The present study was planned to compare the effects of prehabilitation resistance training in mild to moderate clinically frail patients awaiting coronary artery bypass graft (CABG).
Materials and methods
The study design used in this research work is a randomized clinical trial. A total of 74 patients were included in the study and divided into two equal groups. The purposive sampling technique was used for sample size calculation and allocated into two groups for randomization. The study was conducted at the Faisalabad Institute of Cardiology from December 1, 2020 to June 8, 2021 after the approval of the study plan from the Ethical Committee of Riphah International University Islamabad. Both male and female patients under 40–65 years of age who were planned elective primary isolated CABG, patients with double and triple vessel coronary artery disease, and mild to moderately frail patients with a clinical frailty score of 5–6 at the time of accepting surgery at the outpatient cardiothoracic surgical clinic were included in the study. Patients with musculoskeletal disability and neurological disability with affected respiratory rate; patients with renal dysfunction requiring dialysis; the use of immunosuppressive treatments during the 30-day period before surgery; left ventricular ejection fraction <30%; concomitant valve disease; dysrhythmias or pacemaker dependent; patients whose frailty score were severe (CFS 7–9); patients with a recently unstable cardiac syndrome (New York Heart Association (NYHA) Class IV, critical left main coronary disease, congestive heart failure before randomization); patients who were shifted to mechanical ventilation again after extubation postoperatively; and patients who were on the intra-arterial balloon pump after CABG were excluded. The consort diagram for the study is shown in Figure 1.
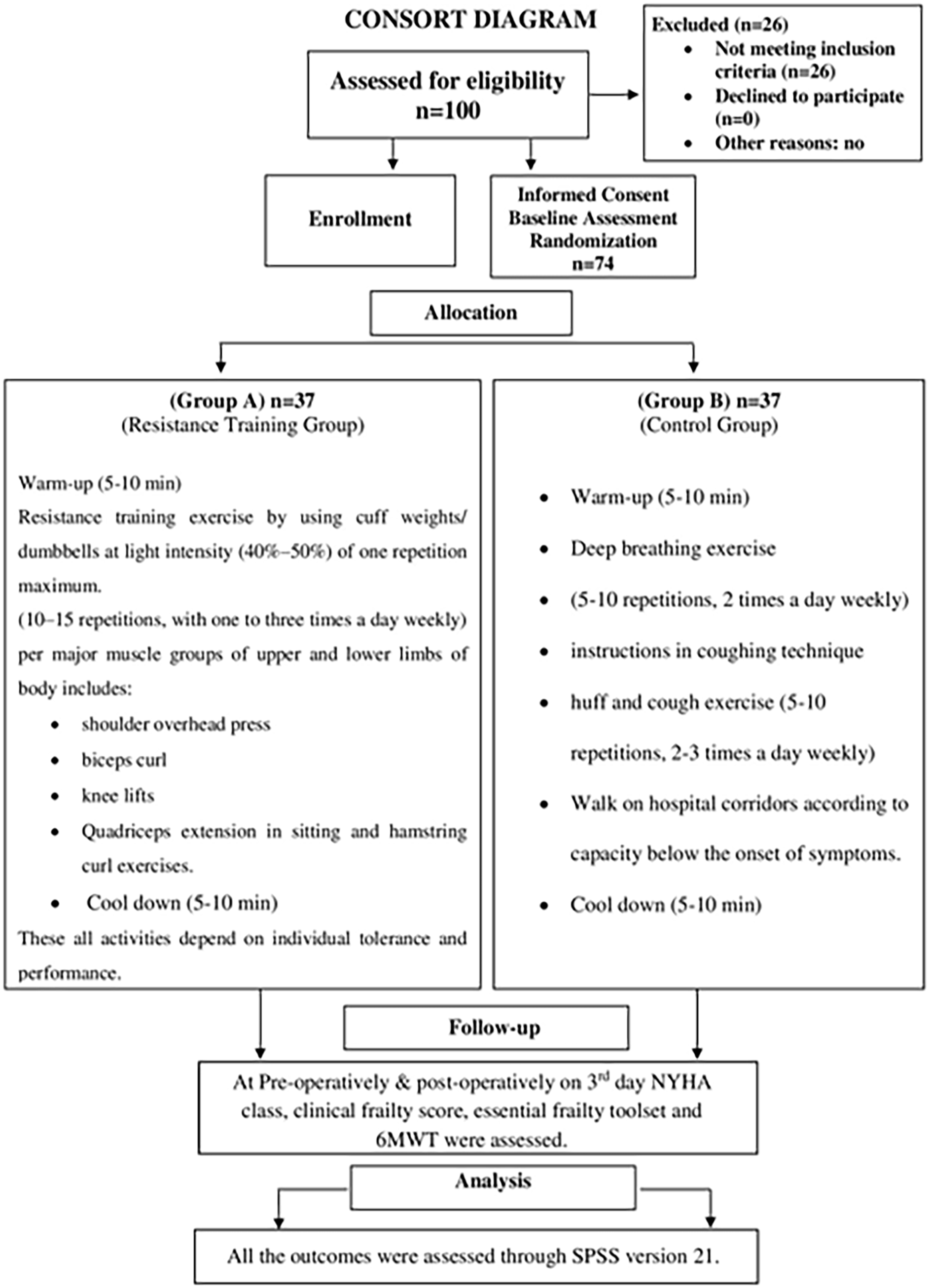
Consort diagram for the study.
After obtaining consent from all the patients and allocation of patients into control and interventional groups through randomization, the baseline data regarding NYHA score for functional classification, 6-minute walk test (6MWT) for measuring functional capacity, and clinical frailty score were measured by CFS and EFT. Then, all the study participants were given exercises as per defined criteria for 8 weeks. After the completion of prehabilitation at 8 weeks, the data regarding NYHA for functional classification scoring, 6MWT for measuring functional capacity, and clinical frailty score were taken for both the study groups. After CABG surgery, again the data regarding NYHA for functional classification scoring, 6MWT for measuring functional capacity, and clinical frailty score were taken for both groups of patients.
Statistical analysis
Statistical analysis was performed using SPSS version 21. The Shapiro–Wilk test was applied to check the normality of data. Mann–Whitney U test was applied to data for between-group analysis and the Friedman ANOVA test was applied to within-group analysis. The p ≤ 0.05 was considered statistically significant.
Results
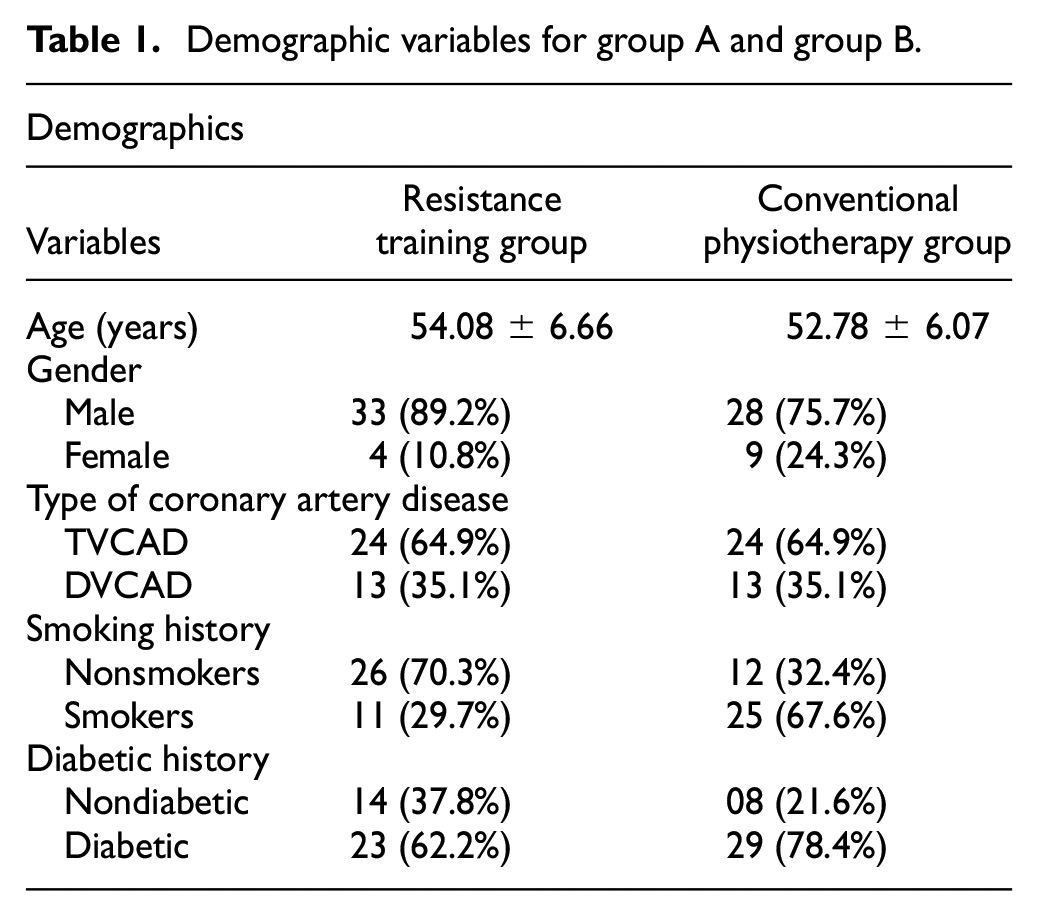
A total of 74 study subjects (N = 74) of both genders were equally divided into two groups: group A (resistance training group) and group B (conventional physiotherapy group) with 37 patients (n = 37) in each group. In this study, three follow-ups were taken at baseline, preoperatively, and postoperatively. The means and standard deviations for the age of group A (resistance training group) and group B (conventional physiotherapy group) were 54.08 ± 6.66 and 52.78 ± 6.07 years, respectively. There were 33 (89.2%) males and 04 (10.8%) females in group A (resistance training group) and 28 (75.7%) males and 9 (24.3%) females in group B (conventional physiotherapy group). In all, 24 (64.9%) patients were planned for CABG surgery due to Triple vessel coronary artery disease (TVCAD) and 13 (35.1%) were due to Double Vessel Coronary Artery Disease (DVCAD) in both groups. In the resistance training group, 11 (29.7%) and 26 (70.3%) were smokers and nonsmokers, respectively. While in group B (conventional physiotherapy group), most of the patients were smokers. There were 25 (67.6%) smoker and 12 (32.4%) nonsmoker patients in group B. In group A, diabetic and nondiabetic cases were 23 (62.2%) and 14 (37.8%), respectively, while in group B, 29 (78.4%) and 8 (21.6%) cases were diabetic and nondiabetic (Table 1).
Demographic variables for group A and group B.
Four variables were compared at baseline, preoperatively, and postoperatively on the third day. These variables include 6MWT, heart rate, oxygen saturation, NYHA, clinical frailty score, and essential frailty toolset. At baseline, there was no significant difference in both groups regarding 6MWT, oxygen saturation, and heart rate. Mann–Whitney U test was applied and p values were 0.489, 0.889, and 0.026 for 6MWT, oxygen saturation, and heart rate, respectively. Significant (p < 0.05) differences in 6MWT, oxygen saturation, and heart rate were observed in preoperative and postoperative cases (Table 2). Other variables were NYHA, clinical frailty score, and essential frailty toolset. At baseline, there were no significant differences between the two groups regarding these three variables. Preoperatively, a significant difference was found in the NYHA class, clinical frailty score, and essential frailty toolset between the two groups with p values of 0.020, 0.032, and 0.022, respectively. A significant difference was also found postoperatively on the third day between the two groups for all three variables including NYHA (p = 0.003), clinical frailty score (p = 0.021), and essential frailty toolset (p = 0.016).
Mann–Whitney U test for 6MWT, oxygen saturation, and heart rate for group A and group B at baseline, preoperatively, and postoperatively on the third day.
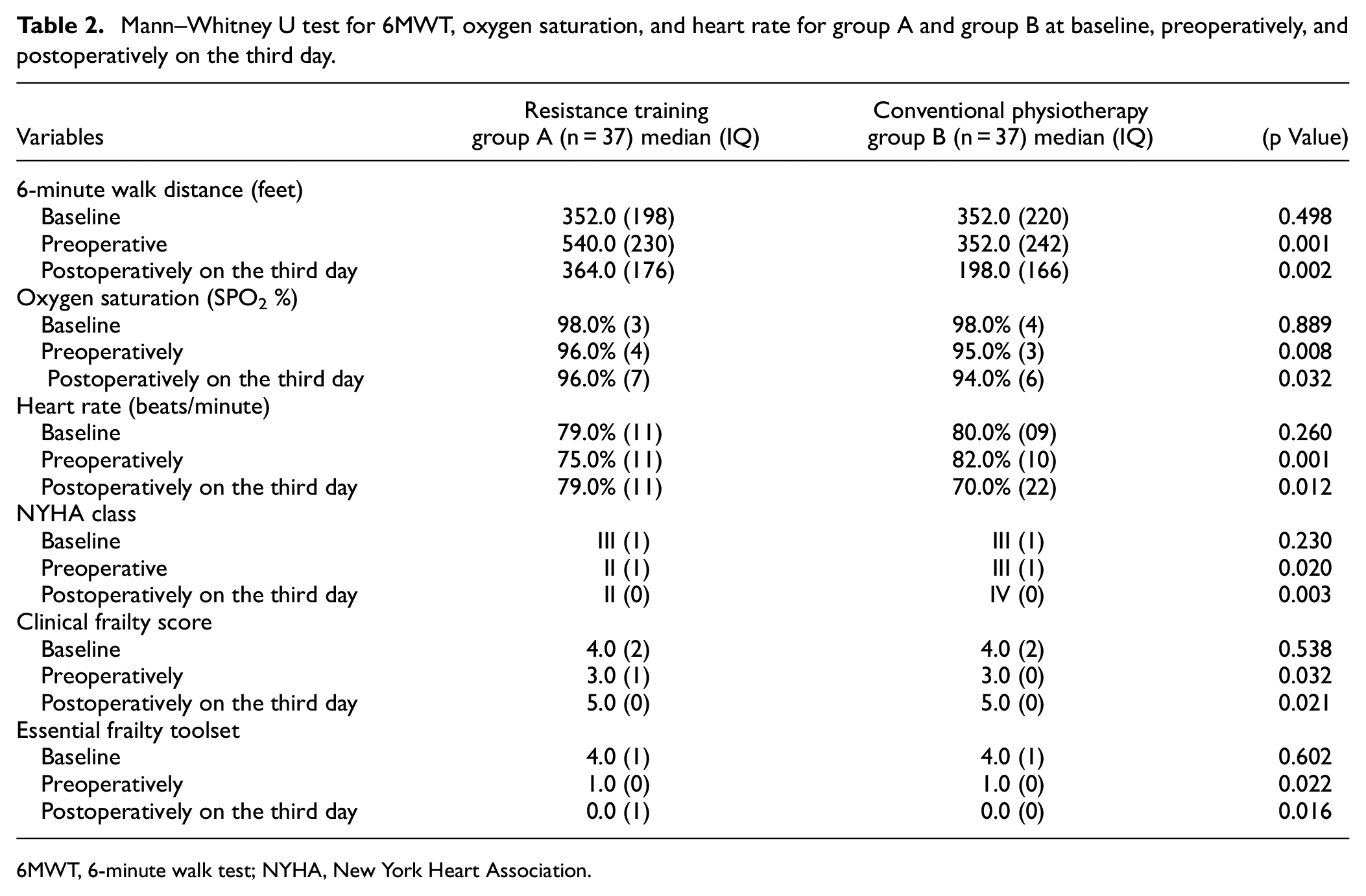
6MWT, 6-minute walk test; NYHA, New York Heart Association.
The within-group comparison showed that both interventional therapy and conventional therapy on 6MWT, NYHA, clinical frailty score, and essential frailty toolset. In group A, the mean ranks at baseline, preoperatively, and postoperatively on the third day were 1.69, 2.61, and 1.70, respectively, and the p value was 0.0001 for 6MWT. For oxygen saturation in group A, the mean ranks at baseline, preoperatively, and postoperatively on the third day were 2.26, 2.08, and 1.66, respectively, and the p value was 0.017. In group A, the mean ranks at baseline, preoperatively, and postoperatively on the third day were 2.04, 2.38, and 1.58, respectively, and the p value was 0.002 for heart rate. The Friedman test was applied (Table 2).
For 6MWT in group B, the mean ranks at baseline, preoperatively, and postoperatively on the third day were 2.35, 2.09, and 1.55, respectively, with a p value of 0.001. In group B, the mean ranks at baseline, preoperatively, and postoperatively on the third day were 2.9, 1.92, and 1.59, respectively, with a p value of 0.001 for oxygen saturation. The Friedman ANOVA test was applied. In group B, the mean ranks for all three follow-ups were 2.09, 1.73, and 2.18, respectively, with a p value of 0.113 for heart rate. The Friedman test was applied.
Other variables were NYHA, clinical frailty score, and essential frailty toolset. In group A, the mean ranks at baseline, preoperatively, and postoperatively on the third day were 2.24, 2.08, and 1.68, respectively, with a p value of 0.004 for NYHA class. The Friedman ANOVA test was applied. For the clinical frailty score, the mean ranks at baseline, preoperatively, and postoperatively in group A on the third day were 2.00, 1.32, and 2.68, respectively, with a p value of 0.001. While the mean ranks at baseline, preoperatively, and postoperatively on the third day were 3.00, 1.86, and 1.14, respectively, with a p value of 0.001 for the essential frailty toolset. In group B, the mean ranks at baseline, preoperatively, and postoperatively on the third day were 1.58, 1.58, and 2.84, with a p value of 0.001 for NYHA class. For the clinical frailty score, the mean ranks at baseline, preoperatively, and postoperatively on the third day were 1.96, 1.28, and 2.76, respectively, with a p value of 0.001, whereas these were 3.00, 1.89, and 1.11, respectively, with a p value of 0.001 for essential frailty toolset (Table 3).
The Friedman test for 6MWT, oxygen saturation, and heart rate for group A at baseline, preoperatively, and postoperatively on the third day.
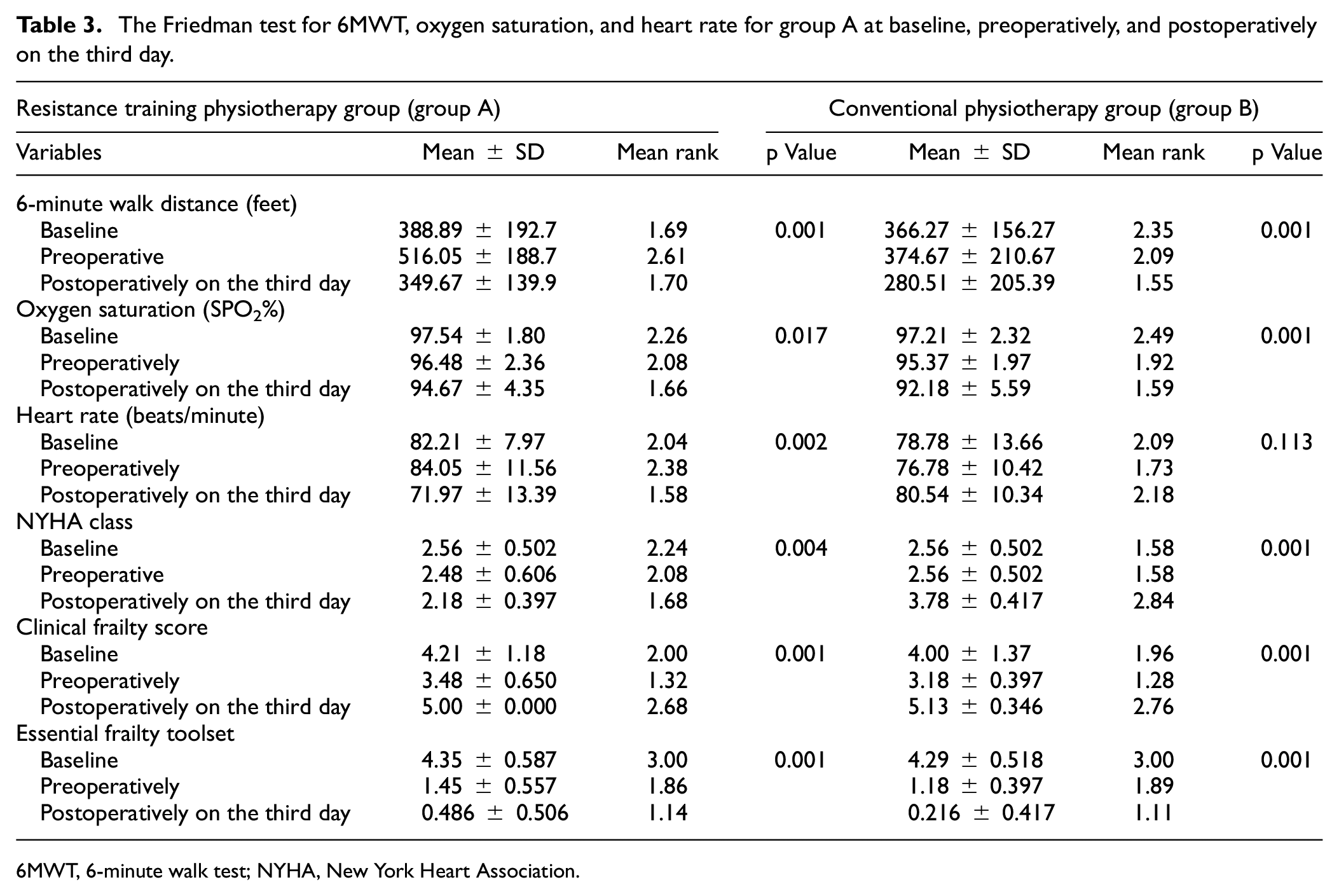
6MWT, 6-minute walk test; NYHA, New York Heart Association.
Discussion
Before cardiac surgery, prehabilitation was selected to return patients to a prior level of functioning in a better way. It was an essential way of intervention to ensure a better quality of life and survival for the patients. Prehabilitation consists of a 2-month intervention before cardiac surgery. It involves exercises like resistance training by using cuff weights/dumbbells. Different respiratory muscle exercises such as diaphragmatic breathing technique (pursed lip breathing) and segmental breathing exercise which includes (apical costal expansion exercise, lateral costal expansion exercise, and posterior costal expansion exercise). The main purpose of prehabilitation is to improve functional capacity, dyspnea, clinical frailty, and essential frailty in patients awaiting coronary revascularization operation.
Coronary artery disease is one of the leading causes of heart attack when blood supply to heart muscles is reduced. It may cause myocardial damage and if this problem is not addressed timely then it causes mortality and morbidity. 11 CABG surgery is the best surgical intervention to treat such conditions in a better way. However, this surgery is highly associated with the occurrence of complications in the postoperative period. It enhances the length of hospital stay, reduces functional capacity, enhances the loss of muscle mass and strength, and it also increases the sensation of fatigue as well. 12 Before surgery, prehabilitation is an important component for the preparation and better functional outcomes of patients after cardiac surgery. Muscular weakness, disturbed activity of daily living, pain, poor pulmonary health, reduced functional capacity, and frailty occurred in patients after CABG surgery. 13
A study conducted by Hulzebos (2019) reported no significant variation in heart rate improvement. 14 However, our current study showed that there was significant variation in heart rate improvement as seen in p value (0.001) preoperatively among both groups of patients. Moradian (2018) conducted research and reported a significant improvement in oxygen saturation in patients after CABG. 15 Our current study also reported a significant improvement (p = 0.032) in oxygen saturation after cardiac surgery. Elkins et al. (2019) reported a significant improvement in rapid shallow breathing by prehabilitation conducted 2 months prior to cardiac surgery. Respiratory muscle training is a more effective technique to reduce breathing, control respiratory rate and heart rate as well. 16 We, in the current study, also found effective results of prehabilitation on patients who have undergone elective CABG surgery.
There was a significant difference observed in functional capacity through 6MWT in the current study when compared to the findings of a published study conducted by Sahar et al. (2020) in which they evaluated the effectiveness of preoperative inspiratory muscle training in patients undergoing CABG and assessed their pulmonary status and functional capacity after surgery. They found differences in the functional capacity in resistance training group patients after CABG surgery. 17 Borges et al. (2019) in their study suggested physical activity for patients with coronary artery disease who are undergoing cardiac surgery. 18 The early 6MWT is a very simple test for the assessment of functional capacity and there is no need for advanced training. Their study concluded a significant difference in improving the functional capacity. While current study results showed significant differences in functional capacity by 6MWT.
Guizilini et al. (2017) reported significant variation in the interventional group concerning the time of 6MWT among the interventional and conventional groups. 19 Helders and van Meeteren (2017) reported positive outcomes for the implementation of 6MWT for better physical activity and survival. 20 Current study also showed a significant difference (p = 0.001) preoperatively to improve exercise capacity. Shakuri et al. (2018) reported significant differences in physiological parameters such as heart rate and oxygen saturation before and after the 6MWT among the two groups. 21 However, there is a contradiction in the findings of such a study that there was no significant variation observed in heart rate, oxygen saturation, and distance covered by 6MWT. 22
Prehabilitation is an effective technique to get better outcomes after surgery. Hirschhorn et al. (2017) in their study observed no significant variation in the physiological parameters such as heart rate, blood pressure, and oxygen saturation 23 while current study results showed a significant difference (p = 0.002) postoperatively on the third day in physiological parameters.
One of the major causes of postoperative pulmonary problems which increases the duration of mechanical ventilation and oxygen therapy was poor preoperative pulmonary fitness in cardiac surgery patients of 45–60 years of age. Nooris et al. (2019) reported that there is a need to find ways to get better preoperative health in patients elected for CABG operation which will have a constructive impact on the outcome of surgery. 24
The current study showed significant variation in essential frailty based on serum albumin, hemoglobin, and chair rises score between two groups while an observational study conducted by Shulman et al. (2019) reported that pre-rehabilitation affects better than improving frailty and reducing shortness of breath. 25
To overcome the risk of postoperative pulmonary complications, it is better to start with physical therapy in prehabilitation phase. A published study illustrated that prehabilitation plays an important role in the postoperative recovery of patients after cardiac surgery. 26 So this intervention was very effective in getting better outcomes.
Conclusion
The present study concluded that resistance training is an effective strategy for the improvement of patient outcomes after cardiothoracic surgery through 6MWT and NYHA class. No significant variation was observed in the clinical frailty score and essential frailty toolset at baseline, preoperatively, and postoperatively on the third day in both the resistance training and conventional physiotherapy groups.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval Reference Number
Ref # Riphah/RCRS/REC/00980