
Abstract
Background and Aims:
X-linked adrenoleukodystrophy (X-ALD) is a genetic disorder caused by mutations in the ABCD1 gene, results in beta-oxidation defect within the peroxisomes and leading to the accumulation of very long chain fatty acids. In his research, Loes et al. (AJNR Am J Neuroradiol. 1994;15(9):1761–6) developed a magnetic resonance imaging (MRI) scoring system on the basis of the anatomical location and involvement of white matter fibres to predict clinical outcomes. The primary objective of our study is to establish a clinical correlation between the Loes score and the neurological symptoms observed in patients with X-ALD.
Materials and Methods:
In our institution, during the study period from 2018 to 2024, 18 patients diagnosed with molecularly and genetically confirmed X-ALD were retrospectively evaluated. Clinical symptoms at presentation and MRI brain findings were assessed with the Loes score.
Results:
Among 18 patients, 10 patients presented without neurological symptoms, with only one of them showing a higher Loes score (>10). Of 8 patients with neurological symptoms, 5 had a Loes score higher than 10. Also, 6 patients with lower Loes score (<4), had no neurological symptoms. The Loes score has a higher sensitivity (87.50%) and a negative predictive value (85.70%) with lower specificity for detecting neurological symptoms.
Conclusion:
The Loes score acts as a preliminary predictor of neurological involvement in paediatric X-ALD cases. Early diagnosis and treatment with haematopoietic stem cell transplantation and continuous monitoring with MRI study play a crucial role in the patient’s prognosis and survival.
Introduction
X-linked adrenoleukodystrophy (X-ALD) is a rare uncommon genetic disorder caused by a mutation in the X chromosome involving the ABCD1 gene, resulting in progressive neurodegeneration. The ABCD1 gene-induced protein helps transport and metabolisation of very long chain fatty acids (VLCFAs) into peroxisomes. In X-ALD, there is defective transport of VLCFAs, leading to their accumulation in various tissues, including the adrenal cortex, spinal cord and cerebral white matter eventually causing neurological degeneration.[1] Owing to its X-linked pattern of inheritance, ALD is primarily a disease of males, though females may act as carriers with or without mild symptoms.[2]
The three distinct patterns of disease are recognised as follows:
Childhood cerebral form of ALD. The age of presentation is usually 4–10 years, characterised by progressive neurological symptoms. Adrenomyeloneuropathy (AMN) type. Usually noted in adult patients with adrenal insufficiency and spinal cord dysfunction. Rare Addison-only type. Characterised by the presence of adrenal insufficiency with no evidence of neurological involvement.
The clinical symptoms in childhood X-ALD vary from clinically asymptomatic patients to rapid neurological decline characterised by cognitive, psychomotor and behavioural impairment.[3] In 1994, Loes devised a 34-point magnetic resonance imaging (MRI)-based scoring system to determine the prognosis and future course of treatment response.[4]
This study primarily aims to determine whether the Loes score can effectively predict the extent of neurological impairment in childhood X-ALD.
Materials and Methods
This is an observational retrospective study conducted in our institution between January 2019 and December 2024. Total 18 patients with genetically proven X-ALD, who had undergone an initial MRI study, were evaluated for the presence of neurological symptoms.
Objective
The objective of our study is to correlate the presence or absence of neurological symptoms with regard to a higher or lower Loes score, based on the extent of white matter demyelination in primary MRI study.
Inclusion Criteria
Patients with genetically proven X-ALD with initial MRI study conducted in our institute.
Exclusion Criteria
Patients with X-ALD, with no initial MRI study available in our institute and X-ALD with only post haematopoietic stem cell transplantation (HSCT) MRI available, are excluded from the study.
Methodology
The MRI study was done using the Phillips Achieva 1.5T MRI Scanner in our institute, and the imaging findings are interpreted using T2, FLAIR pulse sequences and DWI sequences. The information regarding patient’s neurological symptoms at the time of presentation is extracted from electronic health records using a standard data collection form. The data collected include, age at diagnosis, symptomatic or asymptomatic and type of neurological symptoms if present, such as headache, seizure, diminution of vision, hearing loss and behavioural abnormality. The neuroparenchymal involvement in MRI was correlated with the presence or absence of neurological symptoms using the MRI-based Loes score, which employs the extent of white matter demyelination in cerebral neuroparenchyma and corticospinal tracts.
This retrospective study was conducted with prior approval from the Institutional Ethics Committee of Apollo Hospitals. Informed consent was waived due to the nature of the retrospective study.
Statistical Analysis
All continuous variables were tested for normality using Shapiro–Wilk’s test. Categorical variables were mentioned as percentages. Comparison of categorical variables was done by the chi-square test and Cramer’s V effect. Data entry was done using Microsoft Excel 2016. Data validation and analysis were carried out by IBM SPSS Statistics for Windows, Armonk, NY, Version 25.0. All P values <.05 were considered statistically significant.
Results
Out of 18 patients of X-ALD, 8 patients had neurological symptoms in which 1 patient had a Loes score of <4, 2 patients had a Loes score in the range of 4–10, and 5 patients had a Loes score of >10.
In the asymptomatic group without any neurological symptoms, 6 patients had a Loes score of <4, 3 patients had a Loes score in a range of scores 4–10 and only one patient had a Loes score of >10 [Table 1].
Patient distribution across different Loes score category

Our study highlighted an inverse relationship between the Loes score and asymptomatic cases.
Patients with a higher Loes score (>10) demonstrated more neurological symptoms (5 cases) than asymptomatic cases (1 case).
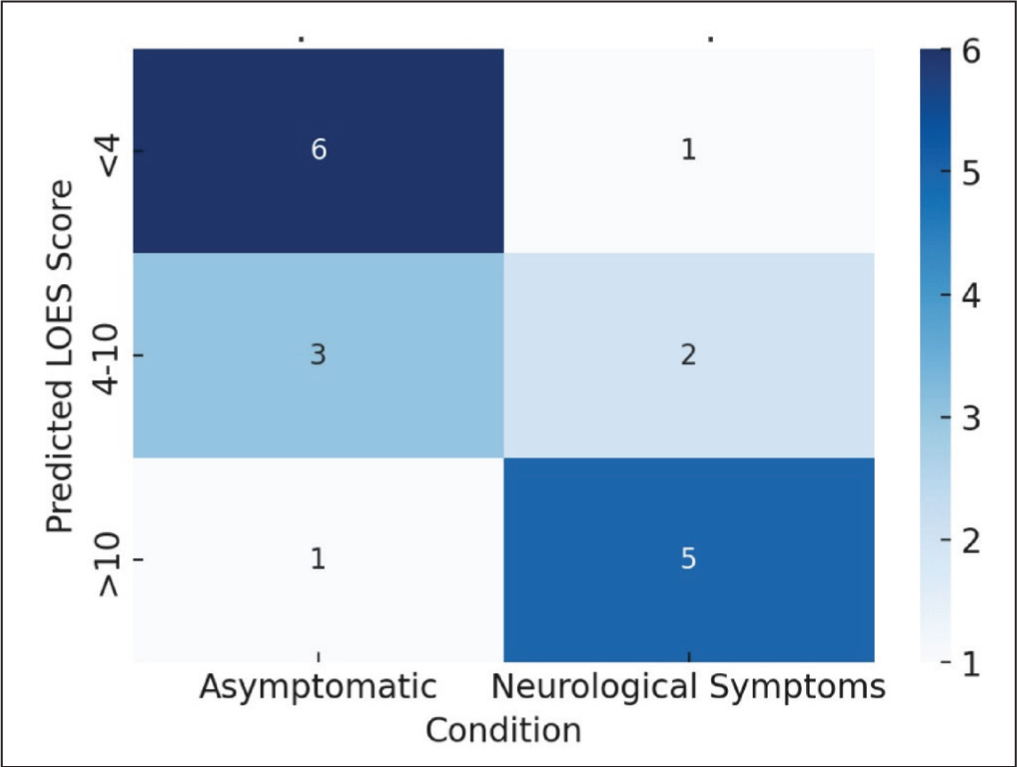
Patients with lower Loes scores (<4) demonstrated more asymptomatic cases (6 cases) than those cases with neurological symptoms (1 case) [Figure 1].
Heatmap frequencies. A heatmap showing the observed frequencies of asymptomatic versus neurological symptoms across different predicted Loes score categories. The darker the colour, the higher the frequency in that category
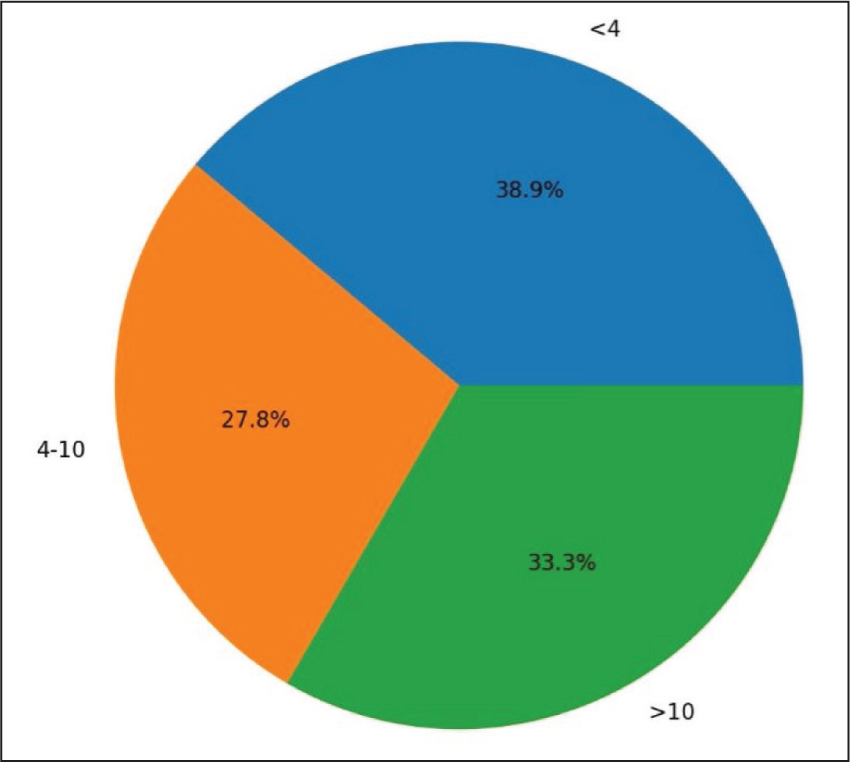
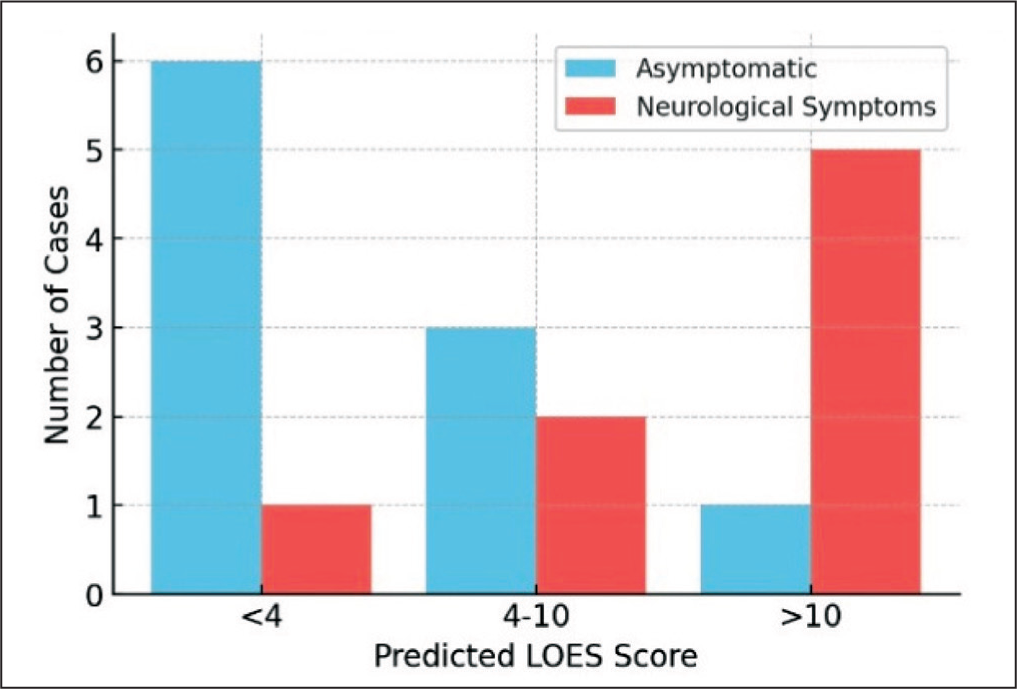
The pie charts and bar charts [Figures 2 and 3] illustrate the distribution of Loes scores and symptoms, emphasising the trend observed in the data. The stacked bar chart further highlights the relationship between the Loes score and symptom categories, showing a clear increase in the cases of neurological symptoms with a higher Loes score.
Pie chart depicting the distribution of asymptomatic and cases with neurological symptom across different predicted Loes score categories
Bar chart depicting the distribution of asymptomatic and cases with neurological symptom across different predicted Loes score categories
The chi-square test was performed, and the following values were obtained:
Chi-square statistic ( χ2) = 6.29; P value = .043; degree of freedom (df ) = 2.
Cramer’s V (effect size):
Cramer’s V = 0.591. Cramer’s V ranges from 0 to 1, where 0 indicates no association. Interpretation: 0.3 suggests a weak association; 0.5 indicates a moderate association; >0.5 suggests a strong association.
The chi-square test results indicate a statistically significant association between the predicted Loes score and the presence of neurological symptoms ( χ2 = 6.29, df = 2, P = .043). Given that the P value is <.05, we reject the null hypothesis, suggesting that the distribution of neurological symptoms varies significantly across Loes score categories. Furthermore, Cramer’s V = 0.591 indicates a strong association between these variables, as it exceeds the 0.5 threshold. This suggests that the predicted Loes score is meaningfully linked to neurological symptoms, implying a substantial relationship rather than a weak or moderate one. However, while the effect size is strong, further research may be needed to determine causality and explore potential confounding factors.
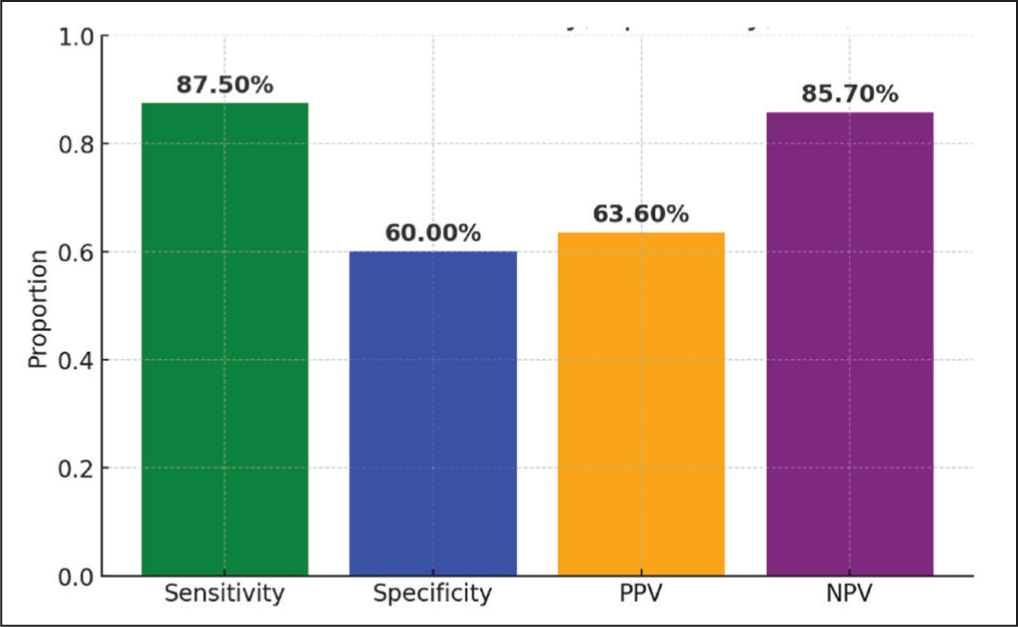
The bar graph [Figure 4] illustrates the key performance metrics—sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV)—for the predictive model based on Loes scores. Sensitivity (87.5%) indicates that the Loes score is highly effective at identifying individuals with neurological symptoms, minimising false negatives. However, specificity (60%) is comparatively lower, meaning that the model has a moderate ability to correctly classify asymptomatic individuals, leading to some false positives. The PPV (63.6%) suggests that about 64% of cases predicted as having neurological symptoms are positive, indicating room for improvement in predictive accuracy. Meanwhile, NPV (85.7%) is relatively high, meaning the model is more reliable at predicting asymptomatic cases correctly. Overall, the model performs well in detecting true positive cases but may require adjustments to improve specificity and reduce false positives.
Key performance metrics of Loes score
Key Observations
For the Loes score <4, most cases are asymptomatic.
For the Loes score 4–10, there is a more balanced distribution.
For the Loes score >10, neurological symptoms dominate.
This visually reinforces our statistical finding that Loes scores are significantly associated with symptom presence. While the sample size is small (~18), the observed effect size (Cramer’s V~ 0.59) supports sufficient sensitivity to detect large associations.
Discussion
X-linked adrenoleukodystrophy is a progressive neurodegenerative disorder caused by mutations in the ABCD1 gene, leading to the accumulation of VLCFAs in brain, adrenal glands and testes.[5] The disease presents with a wide range of clinical variations, from the milder AMN to the more severe cerebral form, known as cerebral X-ALD (cX-ALD). A major challenge in managing X-ALD is the unpredictable nature of neurological deterioration, making regular monitoring and early detection essential for better patient outcomes.
Significance of the Loes Score
The Loes score is a widely recognised imaging tool used to evaluate the severity of cerebral involvement in X-ALD. Based on MRI, quantifies white matter abnormalities, such as demyelination, in specific brain regions [Table 2]. This scoring system plays a crucial role in tracking disease progression, particularly in individuals with cX-ALD, who often experience rapid neurological decline.[4]
MRI severity scale scoring (Loes et al.[4])
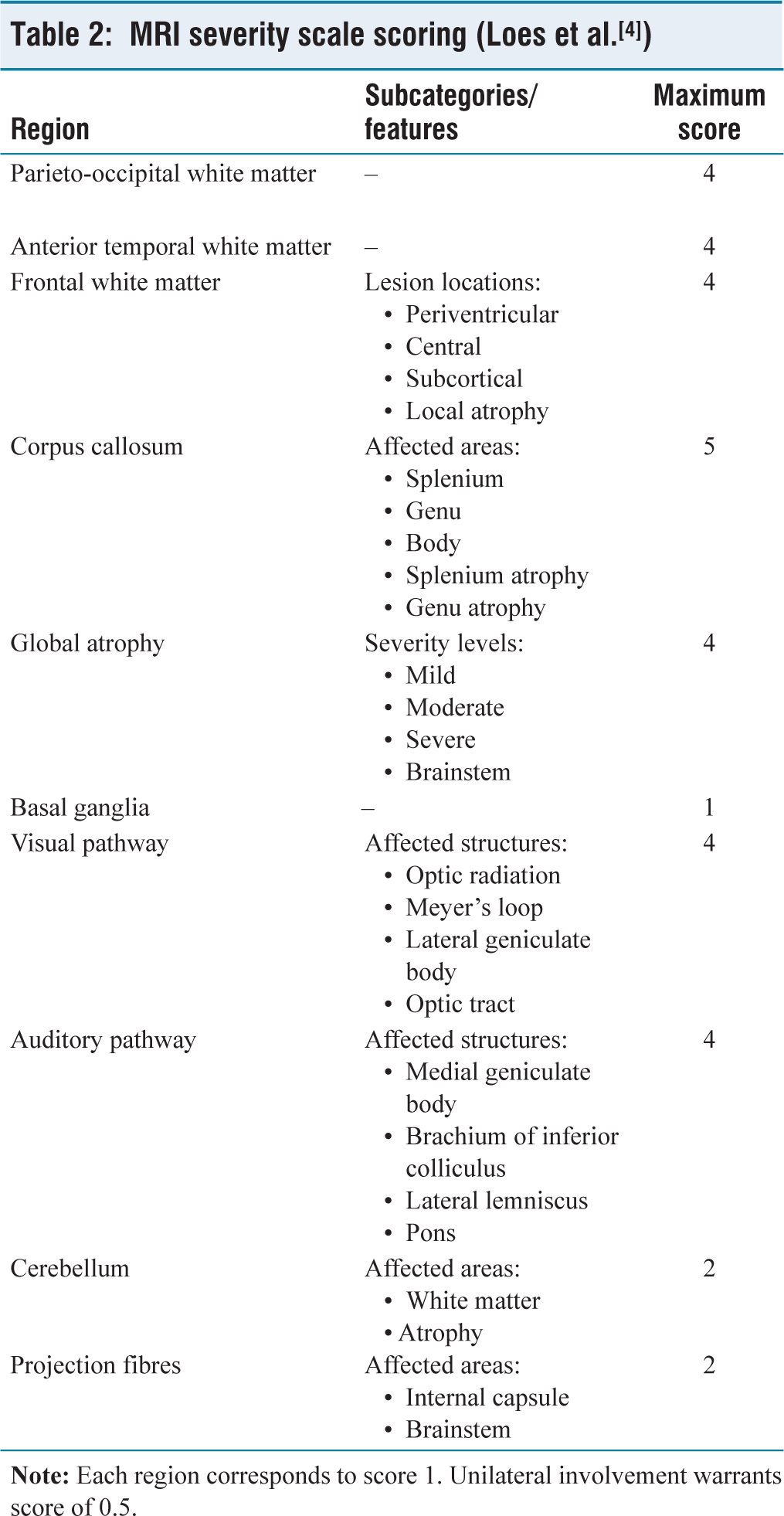
Recent research studies have established a strong link between the Loes score and neurological symptoms, making it a crucial tool for clinicians in evaluating the extent of brain damage and monitoring disease progression. The Loes score divides the brain into multiple regions, including the frontal, parietal, occipital and temporal lobes, as well as the periventricular area, providing a detailed assessment of demyelination. Higher scores indicate more extensive disease involvement and are often associated with a faster onset of neurological symptoms, such as cognitive decline, motor impairments and behavioural changes.
Neurological Symptoms in X-ALD
The neurological symptoms of X-ALD vary based on the age of onset and disease severity. In childhood-onset cX-ALD, symptoms typically progress rapidly, starting with behavioural changes, learning difficulties, vision impairments, hearing loss and motor dysfunction. In late stages, this may progress to spasticity, ataxia, loss of speech and immobility.[6] Hence, early diagnosis and timely interventions are critical, as treatment like HSCT can slow down the progression of neurological symptoms if administered rarely.
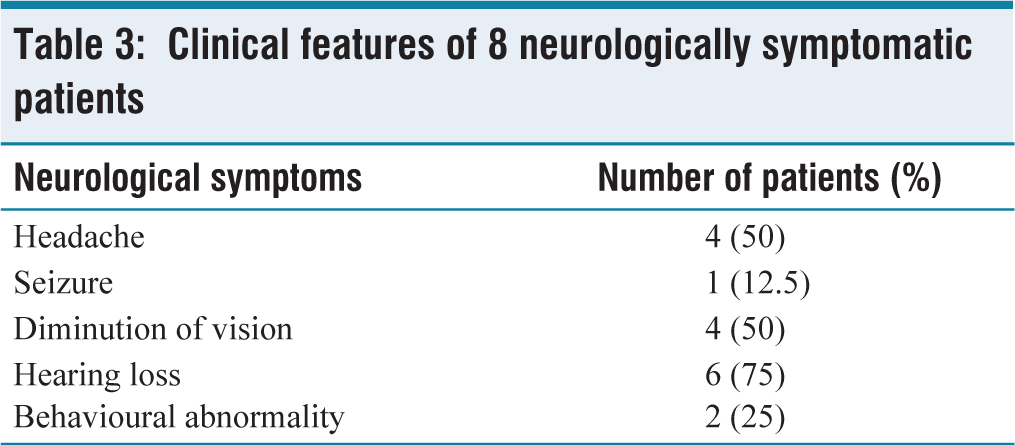
In our study cohort, hearing loss/auditory disturbances were the most frequent symptom [Table 3], present in about 6 out of 8 patients with neurological symptoms (75%). Similar studies have shown that the Loes score is a valuable predictor of neurological deterioration in X-ALD. Kumar et al.[7] in his study demonstrated that Loes score >10 was associated with an increased incidence of motor dysfunction, cognitive decline and disability. In our study, patients with a higher Loes score (>10) showed a greater correlation with neurological symptoms (5 out of 6 patients) than those in the lower Loes score category (<10) [Figure 5]. Thus, the Loes score can be used as an essential tool for determining the disease severity at the time of initial presentation even before the rapid neurological decline sets in. The Loes score can also be used as an early predictor of radiological progression, helping clinicians make timely treatment decisions.
Clinical features of 8 neurologically symptomatic patients
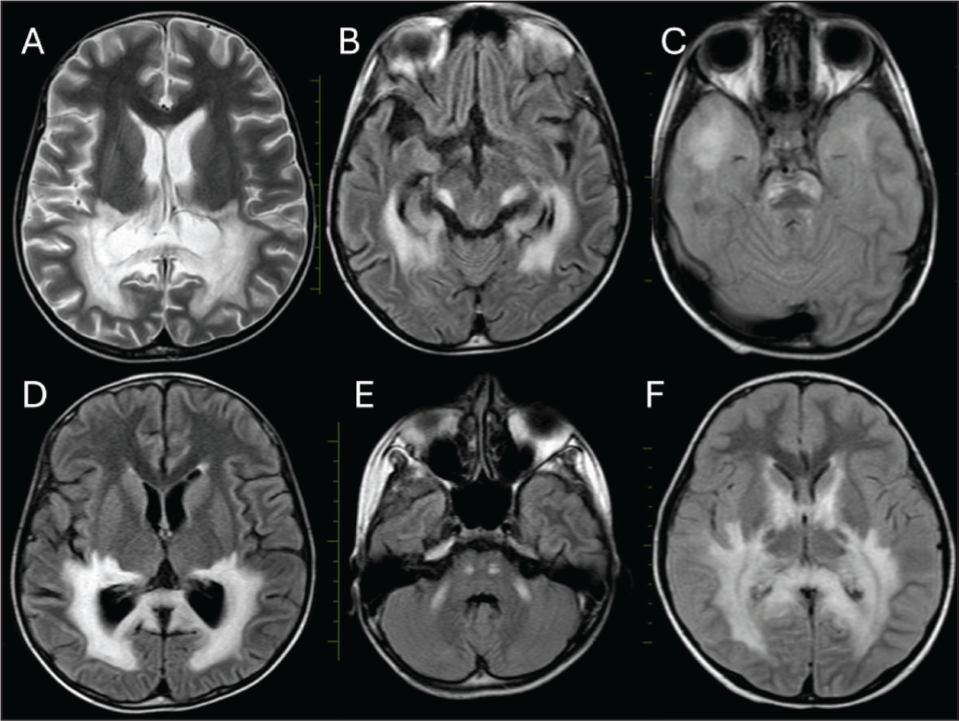
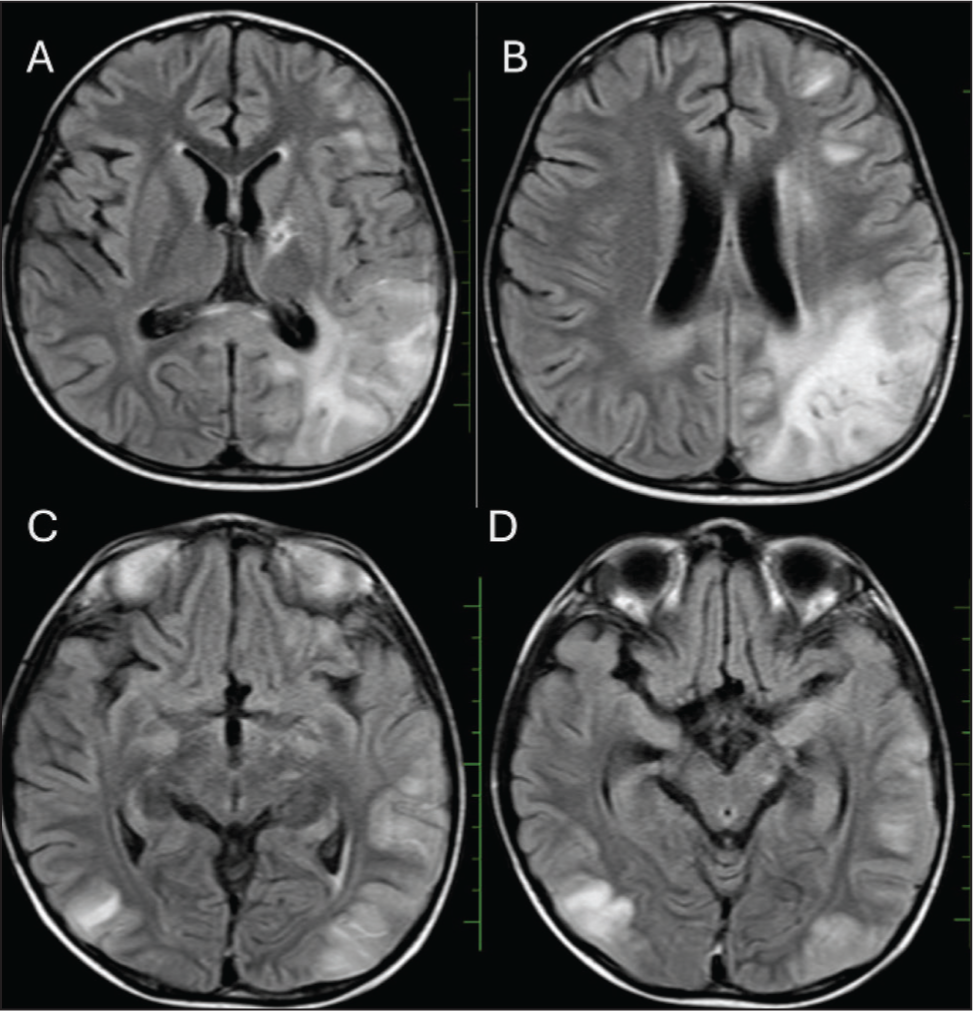
Higher Loes score with neurological symptoms; 4-year-old boy presented with clinical symptoms of decreased visual acuity, worsening hearing loss, muscle atrophy, loss of bladder and bowel control. T2 and FLAIR images show diffuse parieto-occipital white matter demyelination (A and D), with the involvement of bilateral optic radiations and lateral geniculate nuclei (B), bilateral anterior temporal white matter (C), bilateral lateral lemnisci and pons (E), bilateral basal ganglia and internal capsules (F). Calculated Loes score-16 correlated with higher grade of neurological symptoms
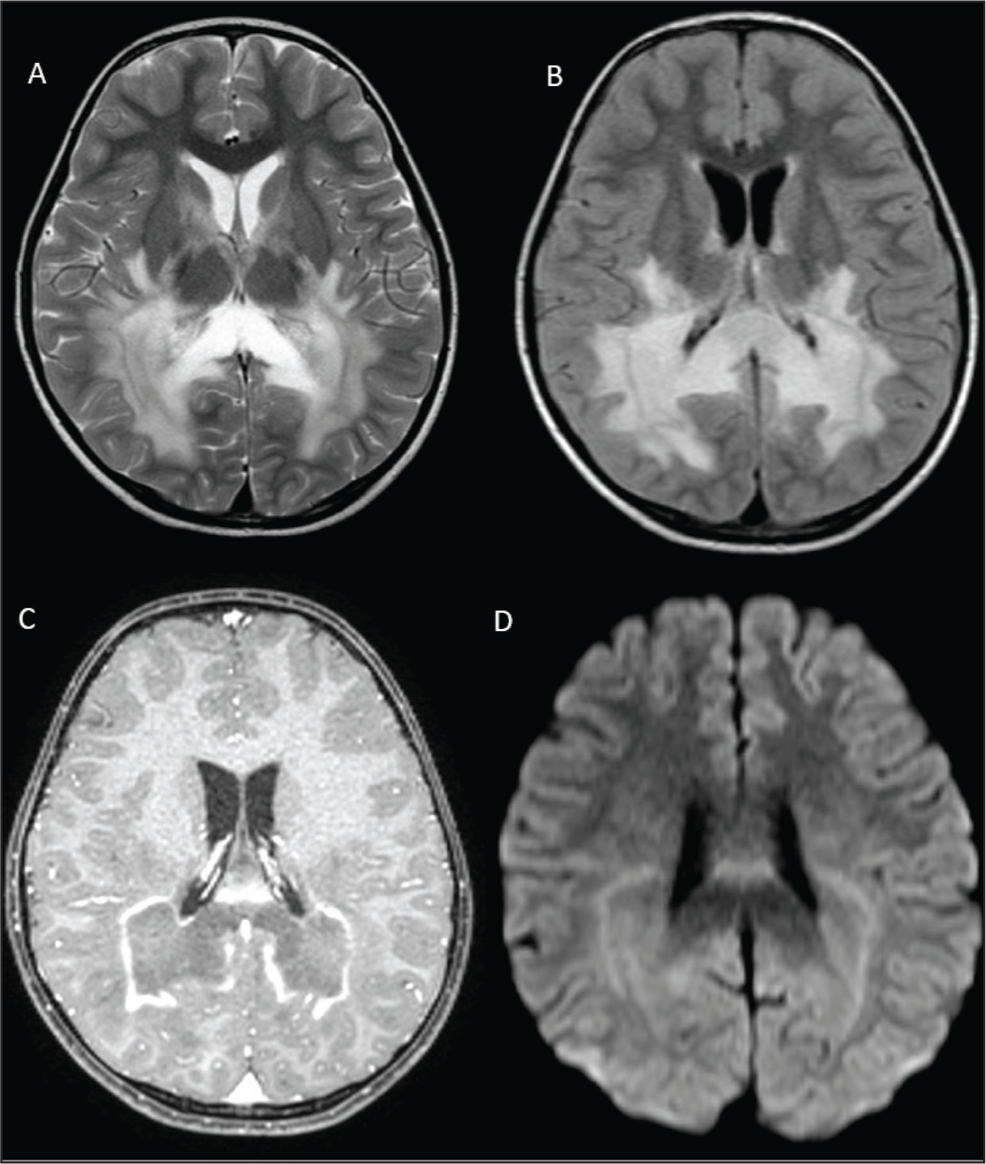
However, in some circumstances, the extent of white matter demyelination reflected as the Loes score may not always align perfectly with the neurological symptoms. Some patients may be asymptomatic despite extensive parieto-occipital white matter and optic tract demyelination changes in MRI [Figure 6], while some patients with lower Loes score may experience mild to moderate neurological symptoms [Figure 7]. This inconsistency may be attributed to factors beyond demyelination, such as genetic variation, inflammatory process and treatment interventions.[8]
Intermediate Loes score without neurological symptoms; 5-year-old asymptomatic boy with X linked ALD. Initial MRI images show diffuse bilateral parietooccipital white matter T2 hyperintensities extending to the splenium and body of corpus callosum on both sides and bilateral internal capsules (A and B). Linear post-contrast enhancement along the leading edge of demyelination (C) and mild restricted diffusion on DWI sequences (D). The calculated Loes score 7, but the patient is neurologically asymptomatic
Intermediate Loes score with neurological symptoms; 3-year-old boy presented with clinical symptoms of decreased visual acuity, worsening hearing loss and muscle atrophy. Preliminary MRI screening shows T2 and FLAIR hyperintensities in bilateral parieto-occipital lobes (A, C and D), left frontal lobe (A and B) and left internal capsule involvement (A). The calculated Loes score is 7, and there is concomitant presence of neurological symptoms
Genetic and Pathophysiological Factors Affecting Disease Progression
Beyond the Loes score, mutations in the ABCD1 gene significantly influence disease progression. The type of mutation can affect the age of onset and severity of symptoms. For instance, mutations causing a complete loss of ABCD1 function are often associated with an earlier onset and more severe neurological decline. In contrast, mutations that allow for partial residual function of the ABCD1 protein may lead to a milder presentation and slower disease progression.[9]
Early Diagnosis and Treatment
Early detection of X-ALD is essential for prompt and preventing disease progression. By checking for elevated VLCFA levels in infants or at-risk individuals, the condition can be detected before the symptoms manifest, enabling early treatment.[2]
Haematopoietic stem cell transplantation is considered as an effective management for cX-ALD, particularly when administered in early changes of disease. Early HSCT can reduce the progression of neurological symptoms, highlighting the significance of regular follow up screening MRI and Loes score monitoring.[10]
Limitations and Future Direction
One key limitation of our study is its cross-sectional design, which prevents us from determining causality or assessing the long-term predictive accuracy of the Loes score for neurological outcomes. Future longitudinal studies are necessary to explore how variations in the Loes score over time align with clinical symptoms and disease progression.
Additionally, this study did not fully account for other influencing factors such as genetic variability, age at symptom onset and coexisting medical conditions. Future research should integrate these variables to provide a more comprehensive understanding of the determinants of neurological decline in X-ALD.
Moreover, while the Loes score is widely used, it remains a semi-quantitative measure that may not completely capture the complexities of disease pathology in X-ALD. Advanced neuroimaging techniques, such as diffusion tensor imaging, could offer deeper insights into microstructural white matter changes and enhance the assessment of disease severity.[11]
Conclusion
In summary, this study highlights the Loes score as a valuable neuroimaging tool that correlates with the severity of neurological symptoms in X-ALD. The strong association between the Loes score and clinical outcomes underscores its role in tracking disease progression and guiding treatment decisions. Given the progressive nature of X-ALD, early diagnosis and timely intervention are critical for improving patient outcomes, with the Loes score playing a crucial role in this process. Future research focused on longitudinal data and advanced imaging techniques are essential for further refining our understanding of X-linked ALD and optimising treatment approaches.
Footnotes
Acknowledgements
It is with deep gratitude, I thank Head of Department, Radiology and Imaging, Dr Jayaraj Govindaraj; my guide Dr Vandana Mahajan, consultants and staffs of HOPE team, Department of Pediatric, Hemato Oncology, for the whole hearted support, steady and strong motivation to complete the task. I also thank the research team, Apollo Hospitals, for their support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Institutional ethical committee approval has been obtained (approval number: ASH-C-S-005/04/2025).
Informed consent
Approval for waiver of consent already obtained from institutional ethical committee, because of retrospective nature of study. Hence no patient consent is required.
Credit author statement
Participated in data acquisition, literature search, investigations, data analysis and manuscript preparation. Participated in conceptualisation, investigation, supervision, data analysis and manuscript editing.
All the authors have reviewed and approved the manuscript.
Data availability
Data presenting the study’s findings are available with the corresponding author.
Use of artificial intelligence
The ideas, interpretations and results are sole work of authors. No AI tools are used in interpretation of data.