
Abstract
Introduction:
Labyrinthine fistula (LF) is a complication of chronic otitis media, especially in cases involving Squamosal disease. The primary objective in managing these cases is to safeguard both cochlear and vestibular functions while effectively addressing the disease. In this study, we provide compelling data from cases treated at our institution, highlighting their presenting symptoms, therapeutic strategies and outcomes.
Methods:
A retrospective review was performed of 20 patients with LF among 96 patients with chronic otitis media squamosal disease managed at our centre between 2018 and 2024 by two surgeons. The clinical features, management, and outcomes were analysed.
Results:
The incidence rate of LF was 20.8%. Although a positive fistula test was observed in only 15% of cases, preoperative imaging with computed tomography (CT) of the temporal bone was conducted in all 20 patients, suggesting a LF. Around nine patients (45%) had symptoms of vertigo preoperatively and all improved after surgery. There was an average increase of 5 dB, 8 dB and 2 dB improvement in hearing on comparing preoperative and postoperative pure tone average, air bone gap and bone conduction thresholds, respectively, in 15 patients who came for follow-up (average duration of three months follow-up). It was also found that those with a higher stage of fistula had poorer hearing outcomes.
Conclusion:
In our study, we observed a striking incidence of LF at 20.8%. Notably, the most frequently affected area was the dome of the lateral semicircular canal, underscoring the importance of careful evaluation in this region. The positive fistula sign and preoperative symptoms of giddiness are unreliable in the preoperative diagnosis of LF. The higher the stage of LF, the greater were the symptoms of giddiness, positive was the fistula sign, and the poorer was the hearing outcome.
Keywords
Introduction
Cholesteatoma is a slowly growing and damaging epithelial lesion found in the temporal bone. Abramson et al. provided a detailed definition of cholesteatoma. Cholesteatoma is defined as a three-dimensional epidermal and connective tissue structure, typically resembling a sac that often conforms to the architecture of the middle ear, attic and mastoid spaces. This structure possesses the ability for progressive and independent growth, leading to the erosion of underlying bone and it is known to have a tendency to recur after surgical removal.[1] Labyrinthine fistula (LF) is a complication associated with chronic squamous otitis media, with an incidence rate ranging from 4% to 12%.[2–10] Among LF cases, approximately 50%–80% may experience vertigo,[11–13] alongside other common symptoms of chronic otitis media such as ear discharge and decreased hearing. Literature suggests that the positive fistula sign is present in about 9%–55% of these cases.[14,15] The primary objective of managing LF is to preserve cochlear and vestibular function while eliminating the disease. The extent of the fistula can lead to substantial hearing loss both preoperatively and postoperatively, as supported by compelling studies conducted by Soda-Merhy et al. and Kvestad et al.[16] This highlights the critical importance of addressing fistulas promptly to mitigate the risk of hearing impairment.
Regarding the management of LF, various approaches have been proposed. Some studies advocate removal of the matrix from the fistula site,[17–19] followed by fistula repair. Some suggest exteriorising the cavity, leaving the fistula site covered with matrix. The choice between these methods often depends on the extent of the disease, as recommended by different authors.[20] Achievement of a positive hearing outcome following surgery is considered to be low. Clinical records of 20 patients with LF in the setting of cholesteatoma who were managed surgically were studied retrospectively to assess the clinical profile, management and outcomes.
Materials and Methods
This is a retrospective study based on electronic patient data from January 2018 to December 2024. Ninety-six cases who underwent surgery for chronic otitis media squamosal disease were identified. Among these, 20 patients had LF. The clinical records of these patients were studied after obtaining clearance from the Institutional Ethics Board.
Inclusion Criteria:
Patients diagnosed with chronic otitis media squamosal type based on clinical history, examination and audiological assessment Patients who are undergoing a surgical procedure (canal wall down mastoidectomy) Patients aged 16 years or older Patients who underwent audiogram and computed tomography (CT) of the temporal bone as part of their investigation
Exclusion Criteria:
Patients with acute otitis media or any other infection in the ear Patients with incomplete details on clinical history, radiological and operative findings Patients in whom intracranial complications are present Patients undergoing other ear surgeries such as tympanoplasty.
Methodology
The demographic details, surgical records, imaging, preoperative and postoperative audiometry and follow-up records were obtained from electronic patient data. These data were entered into an Excel sheet and their inferences were obtained.
The incidence, clinical presentation, surgical technique and hearing outcomes were studied. The preoperative audiogram and the first postoperative audiogram (during the third month follow-up) were considered. The LF was graded as per Dornhoffer and Mileskwi staging. In addition to that, preoperative and postoperative pure tone audiograms were statistically analysed to determine improvement in the air bone gap following surgery. The air conduction and bone conduction at 500, 1,000, 2,000 and 4,000 Hz preoperatively and postoperatively were noted on Microsoft Excel software and analysed for change in hearing thresholds postoperatively. The air bone gap was calculated from the differences between the air conduction (AC) and bone conduction (BC) thresholds.
Results
Clinical Profile
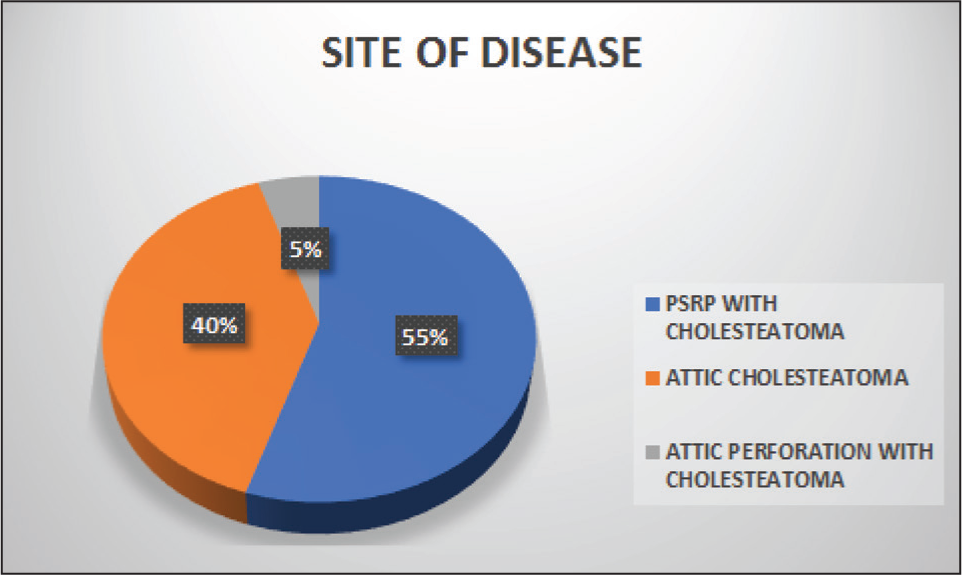
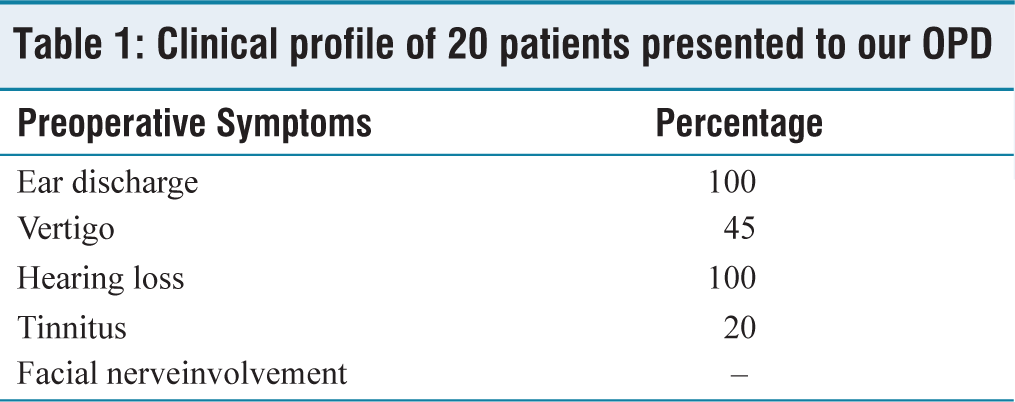
Within the study period of six years, January 2018-December 2024, a total of 96 patients with chronic otitis media squamosal disease were identified, out of which 20 cases had LF, which was suspected in high-resolution computed tomography (HRCT) temporal bone. The sites of disease in these 20 patients are illustrated in Figure 1. Out of the 20 patients, 15 (75%) had involvement of the right ear and five (25%) had involvement of the left ear. Thirteen (65%) were males and seven (35%) were females with, a median age of 31 years (age range, 11–63 years). Out of these 20 patients, three (15%) had positive fistula sign, 4 (20%) had tinnitus and four (20%) had sensorineural hearing loss preoperatively. None had facial palsy or aural pain preoperatively. The clinical profile of 20 patients presented to our outpatient department (OPD) is listed in Table 1.
Site of disease
Clinical profile of 20 patients presented to our OPD
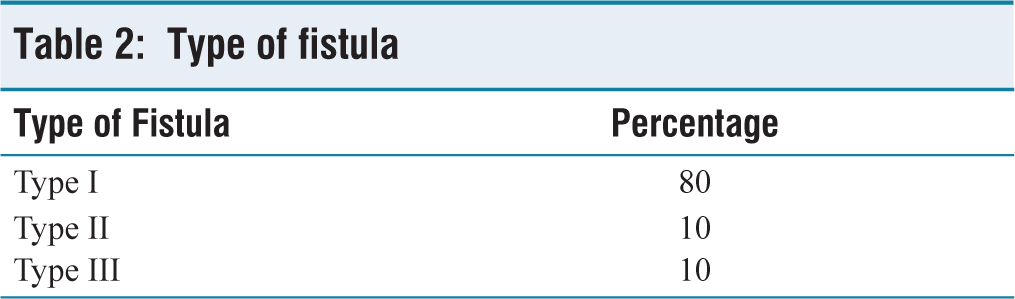
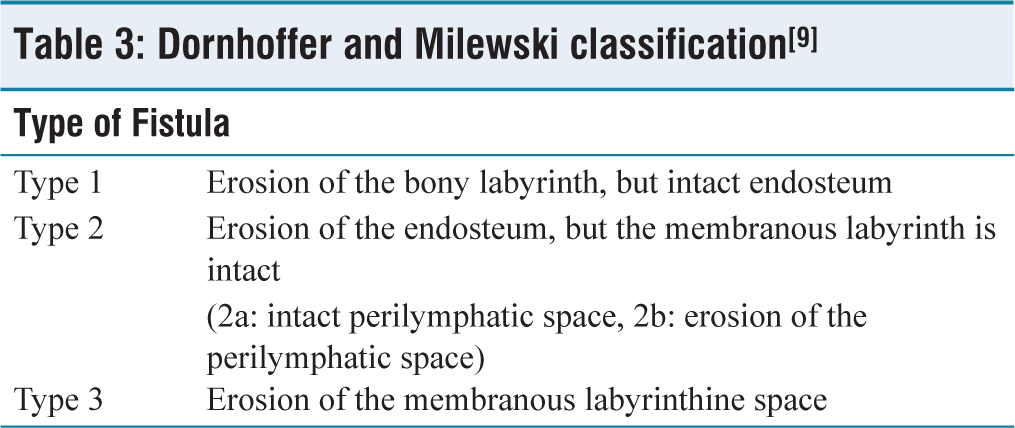
The findings on otoscopic examination of the diseased ear are summarised in Figure 1. In all these patients, CT temporal bone was performed preoperatively, which was suggestive of lateral semicircular canal dome fistula in 19 (95%) patients and superior semicircular canal arch fistula in one (5%) patient. None of these patients had multiple site involvement, or fistula on the promontory, or a cochlear fistula. Out of the 20 patients, 19 (95%) underwent primary surgery and one (5%) underwent revision surgery. During surgery, we found that 16 patients (80%) had a type I fistula, two patients (10%) had a type IIb fistula and two patients (10%) had a type III fistula. These results are shown in Table 2, and according to the Dornhoffer and Milewski classification system [Table 3].[9]
Type of fistula
Dornhoffer and Milewski classification[9]
Surgical Management
The operative management of the LF was done according to the uniform protocol followed at our institution. Surgery commenced with the decisive removal of the cholesteatoma and thorough eradication of the disease. Canal wall down mastoidectomy was done in all these 20 cases (100%). The management of the suspected fistula site was performed after each surgical procedure. As the surgery approached its conclusion, the matrix was expertly dissected from the fistula site using ample irrigation, ensuring a precise and efficient removal. The site was effectively sealed using either bone dust and temporalis fascia or a comprehensive layered approach that included temporalis fascia, conchal cartilage and additional temporalis fascia. All patients were followed up for a minimum duration of three months post-surgery to assess outcomes. The results were analysed concerning postoperative improvements in hearing, vertigo symptoms and disease eradication.
Statistical Analysis
The demographic data, surgical records, preoperative and postoperative audiological data and follow-up records were obtained from the computerised database maintained at our institution. The data were analysed in MS Excel. The baseline variables were represented using descriptive statistics. Four frequency averages (i.e., 0.5 kHz, 1 kHz, 2 kHz and 4 kHz) were obtained, and these were used to calculate the preoperative and postoperative air–bone gap (ABG), AC and BC.
Out of the 20 patients with LF, 15 patients came for follow-up. Of these 15 patients eight had symptoms of giddiness preoperatively. The symptom of giddiness had resolved in all the patients in the first postoperative visit.
Among the 15 patients who came for follow-up postoperatively, pure tone average, BC threshold and air bone gap were studied in the frequencies 500 Hz, 1,000 Hz, 2,000 Hz and 4,000 Hz [Table 4].
Average preoperative PTA, BC and ABG change and postoperative PT, BC and ABG according to the stage of fistula

Preoperative and postoperative change in pure tone average of 15 patients ranged from −3.75 dB to 27.5 dB and the mean change was 5 dB. There was an average increase of 5 dB in hearing among these patients.
Preoperative and postoperative change in BC threshold of 15 patients ranged from −1.25 dB to 36.5 dB and the mean change was 2 dB. There was an average increase of 2 dB in hearing among these patients.
Preoperative and postoperative change in air bone gap of 15 patients ranged from −1 dB to 26.25 dB and the mean change was 8 dB. There was an average increase of 8 dB in hearing among these patients.
Therefore, on an average, comparison of preoperative and postoperative changes in pure tone audiometry (PTA), BC and air bone gap, revealed an overall improvement in hearing.
Preoperative and postoperative hearing outcomes based on the stages of fistula: 16 patients had stage I fistula, of which 12 came for follow-up, two patients had stage IIb fistula, of which one came for follow-up, two patients had stage III fistula, of which both patients came for follow-up.
In stage I and IIb, on comparing the preoperative and postoperative PTA, BC and ABG, hearing did not deteriorate. However, in stage III, hearing deteriorated, which suggests that as the stage of fistula increases, hearing loss increases in parallelly [Table 4].
Discussion
The incidence of LF in patients with chronic squamous otitis media was found to be 20.8% in our study. In previous studies by Soda-Merhy et al.[10] and Gersdorff et al.[13] has quoted lesser rates of 7.5% and7%, respectively. Compared to the literature, our incidence was greater, citing the better preoperative diagnostic modalities (HRCT temporal bone) and better intraoperative microscope and surgical expertise in identification of LF. Compared to the studies by Quaranta et al.[6] (57% in males and 42% in females) and Soda-Merhy et al.[10] (41% in males and 59% in females), in our study the incidence of LF was 65% in males and 35%in females, which revealed no significant gender preference. Our results revealed no significant difference between the involvement of the right ear (75%) and the left ear (25%), which was comparable to the study done by Dornhoffer and Mileskwi.[9]
In our study, the symptoms of hearing loss and ear discharge were observed in all 20 (100%) preoperatively, which was comparable to the study by Rajasekhar et al. which showed 100%.[21] Giddiness as a main complaint was present in 45% of the cases, which is similar to the study by Quaranta et al.[6] where they found that 43% presented with giddiness. Other studies by Dornhoffer and Mileskwi,[9] Soda-Merhy et al.,[10] Kobayashi et al.[15] showed 62%, 78% and 100%, respectively. The symptom of giddiness has improved in all patients postoperatively which was comparable to study by Chen et al.[22] Also, it was interesting to note that the symptoms of giddiness (three out of nine patients) were found in patients with both the stage IIb and one stage III fistula patients, which was comparable to a study by Busaba[12] Tinnitus was detected in 20% of cases, which was similar to the study by Kvestad et al.[14] which showed 16%. Positive fistula sign was noted in three patients (15%), out of which two had stage IIb fistula and one had stage III fistula which was similar to the study by Busaba.[12]
Similar to other studies, in our study, the presence of lateral semicircular canal fistula was recorded in about 95% of patients, and the remaining 5% had superior semicircular canal arch fistula. A study done by Herzog et al.[11] reported lateral semicircular canal fistula in 94.1% and superior semicircular canal involvement of 7% was found in a study by Soda-Merhy.[10] There was no multiple site involvement, promontory or cochlear fistula in our study, which was also similar to studies by Herzog et al.,[11] Kobayashi et al.[15] and Palva et al.[16] Preoperative CT scan showed evidence of LF in all the patients (100%) which was similar to the study by Kobayashi et al.[15] which also showed 100%. However, in the study conducted by Parisier et al.[8] the detection rate of LF using imaging was only 55%. Factors such as the imaging protocol used in the CT scans and the thickness of the slices obtained during the scanning process might also influence the effectiveness of the preoperative scans. Stage I LF was seen in 16 (60%) patients, stage IIb in two (20%) patients and stage III in two (20%) patients intraoperatively. However, in another study by Meyer et al.[18] the type II fistula (52%) was higher, followed by type I (38%) and type III (10%). On comparing the preoperative and postoperative, BC and air bone gap there was an improvement in hearing overall which was comparable to a study by Kobayashi et al.[15] On studying the hearing outcome based on the stage of fistula, the higher the stage of fistula lower the hearing outcome. Where in our study, in stage III fistula, on comparing preoperative and postoperative PTA, BC and ABG averages, there was 6 dB, 2 dB, and 4 dB decrease in hearing which was comparable to study by Chen et al.[22] a reduction in BC threshold of 10 dB hearing on an average was observed in patients with stage III fistula. Therefore, hearing outcome correlated best with the extent or stage of fistula, which was comparable to the study by Busaba[12]
Limitations
Small sample size, where the findings may not be generalisable to a larger population, Single-centre study and lack of longitudinal follow-up.
Conclusion
Our study found that the incidence of LF was 20.8% which is higher than the rate quoted in the literature. We attribute this to better preoperative diagnostic modality such as HRCT temporal bone, better intraoperative microscopes and better surgical expertise in the careful removal of fistula. The commonest site involved was the dome of the lateral semicircular canal. The positive fistula sign and preoperative symptoms of giddiness are unreliable in the preoperative diagnosis of LF. The higher the stage of LF, greater were the symptoms of giddiness, positive was the fistula sign and the poorer the hearing outcome.
Footnotes
Acknowledgements
To the Research Department, Apollo Main Hospital, Chennai.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Institutional ethical committee approval number: IEC-BMR App No.: AMH-C-S-030/03-25.
Informed consent
Informed consent from individual patients was not required as this was a retrospective study using anonymized hospital records.
Credit author statement
MM participated in conceptualisation, methodology, data collection, data analysis, literature search and manuscript preparation.
SKS and PSR: Conceptualised and designed the study, supervised data collection and performed critical revision of the manuscript.
All the authors have reviewed and approved the manuscript.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author upon request.
Use of artificial intelligence
The authors confirm that no generative artificial intelligence tools were used in the preparation of this manuscript.