
Abstract
Background:
Patients in the ICU frequently experience qualitative and quantitative sleep disruption. The Richards-Campbell Sleep Questionnaire (RCSQ) is a validated tool to assess the quality of sleep in critically ill patients. The aim of our study was to assess the quality of sleep in non-ventilated critically ill patients, explore reasons and evaluate patient and nurse perception of quality of sleep in critically ill patients.
Patients and Methods:
The study is a single-centre, prospective observational study conducted among non-ventilated patients in our tertiary critical care unit. After ruling out delirium in patients with the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) delirium screening tool, the perception of sleep quality was assessed twice using the modified RCSQ, from the patient and the bedside nurse in an independent, blinded manner during the ICU stay. In addition, factors contributing to sleep disruption were assessed.
Results:
In our study, during the first assessment, the average sleep score was 57.2 (±18.4) and 65.0 (±19.4) (P < .05), and the noise score was 52.3 (±23.8) and 61.8 (±26.1) for the patients and nurses (P < .05), respectively. During the second assessment, the average sleep score was 62.8 (±15.4) and 70.0 (±12.0) (P < .05), and the noise score was 62.9 (±16.4) and 72.4 (±15.8) for the patients and nurses (P < .05), respectively. Noise level, nursing interventions and blood sampling were the predominant factors affecting sleep.
Conclusion:
Patients admitted to our ICU had moderate quality of sleep, which improved over time. Nurses overestimated sleep and underestimated noise levels compared to patients. Noise was the predominant factor affecting sleep.
Highlights
A single-centre, prospective observational study was conducted among non-ventilated patients. The perception of sleep quality and factors affecting sleep were assessed twice using modified RCSQ, from the patient and the bedside nurse. Patients had moderate quality of sleep, which improved over time. Nurses overestimated sleep and underestimated noise levels compared to patients.
Introduction
Sleep is essential for recovery and restoration of health in acutely ill patients admitted to the intensive care units (ICU). Sleep patterns in critically ill patients are altered due to multiple factors, including environmental, disease-specific, patient-related and/or health care-associated factors, leading to adverse outcomes.[1,2] Sleep pattern in the ICU is more fragmented with reduced duration of NREM stage 3 and REM sleep.[2] Sleep dysregulation induced imbalance of hormones, including catecholamines, cortisol, growth hormone and prolactin, results in higher pain perception, poor glycaemic control, altered consciousness and immune suppression, leading to increased risk of infections.[3,4] The amplification of the physiological stress triggered by the poor quality of sleep in hospitalised critically ill patients delays the recovery following discharge from hospitals.[5] Although the effect of sleep quality on the incidence of delirium is not established, a severe reduction in the REM sleep duration is associated with a higher incidence of delirium and a higher need for sedatives.[6] It is not clear if delirium is a cause or effect of poor sleep in the ICU. Disturbance in sleep and circadian rhythms in critically ill patients is often associated with various neuropsychiatric manifestations, including cognitive impairment and post-traumatic stress disorder.[7,8]
Studies on sleep and circadian rhythms in critical illness survivors showed widespread sleep disruptions in this patient population.[7–9] Studies have shown that about 60% of patients report sleep disturbances after ICU admission.[10,11] To overcome this, guidelines formulated by various critical care groups recommend a multidisciplinary approach for improving sleep quality and minimising delirium.[12,13] Several factors are shown to disrupt sleep in critically ill patients, and some of them are known to persist even after discharge.[13] The environmental factors affecting the sleep of acutely ill patients include noise, temperature, telephone, television, conversation in the room and alarms.
Various subjective and objective methods have been used for the assessment of the quality of sleep in critically ill patients. Polysomnography (PSG) is the most reliable tool and is considered the gold standard for assessment of sleep.[14,15] The use of PSG for the assessment of sleep in hospitalised patients is complicated by its limited availability, interference from other electronic monitors and cost. Various questionnaire-based subjective methods for assessing the quality of sleep in patients are validated for use in ICU settings. Though the use of questionnaire-based assessment of sleep is simple, its clinical utility is limited by the inability of the critically ill patient to complete the questionnaire in most instances. The Richards-Campbell Sleep Questionnaire (RCSQ) was evaluated for assessment of sleep in critically ill patients in the ICU, and it demonstrated good inter-rater reliability and agreement.[16] Several studies have previously found RCSQ as a useful tool in evaluating the quality of sleep in ICU patients.[16–18]
There is inadequate data on the quality of sleep and the nurse’s perception of the same in the critically ill Indian population. We intended to assess the quality of sleep in our critically ill patients, assess the reliability of nurses’ perception of patients’ sleep and identify the factors disturbing patients’ sleep.
Materials and Methods
The study is a prospective observational study, conducted in a multidisciplinary critical care unit of a tertiary care hospital among non-intubated critically ill patients for a period of one year from September 2020 to August 2021.
The aim of the study is to assess the quality of sleep in our critically ill patients, assess the reliability of nurses’ perception of patients’ sleep and identify the factors disturbing patients’ sleep.
The primary objective of the study was to assess the quality of sleep in critically ill patients admitted to critical care units in our hospital. The secondary objectives were to compare the patients’ and nurses’ perception of quality of sleep and to identify the barriers to good quality sleep in acutely ill patients.
All the patients admitted for more than 24 hours to the critical care unit who were non-intubated and above 18 years of age were included in the study. Patients who were intubated, unable to comprehend English and/ or refused to consent were excluded.
Methodology
The institution’s scientific and ethics committee approvals were obtained (IEC Number: AMH-DNB-006/02-20). After obtaining an informed written consent, the patients were assessed for orientation to time, place and person and then screened for delirium with the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) delirium screening tool.[19]
After ruling out delirium, the quality of sleep as perceived by the nurse providing care and the patient was assessed independently and in a blinded manner, using the modified RCSQ. The RCSQ evaluates five parameters related to sleep, namely the sleep depth, sleep latency, awakenings, returning to sleep and sleep quality and is scored on a visual analogue scale, with 0 indicating a poor score and 100 representing a better score. The perceived quality of sleep is evaluated by a total score derived from the mean of the five parameters of sleep. Perceived night-time noise was included as the sixth parameter (range: 0 for ‘very noisy’ to 100 for ‘very quiet’).[20] In contrast to the sleep components of RSCQ, the lower and higher scores of noise components indicate more and less noise perception, respectively. The nurses were educated on the RCSQ questionnaire prior to the commencement of the study. Patients were educated on RCSQ by a research assistant, who also remained at the bedside of the patient to address their queries while filling out the assessment form. The RSCQ questionnaire was in English, and hence, patients unable to read and/or understand English were excluded from the study.
Factors related to sleep disruption, as perceived by the patient, were collected along with RCSQ. The factors recorded include patient-related factors (pain, nausea, breathing difficulty, anxiety, pre-existing sleep disorders), environmental factors (noise, light, temperature, conversation in room, alarms, television, bedside phone) and healthcare-related factors (nursing interventions, imaging, vitals measurement, blood sampling, nebulisation, oxygen probe, drug administration, non-invasive ventilation).
Questionnaire Administration
Nurses’ perception of the sleep quality of patients was assessed with the RCSQ questionnaire filled by the respective night shift nurses, on completion of their shifts. The patients were simultaneously evaluated with the RCSQ independently, on the subsequent morning. Both the nurses and patients were blinded to each other’s responses. The assessment by the nurse and the patient was done twice during the patient’s stay. The first assessment was done after 24 hours of admission to the ICU, and the second one after 5 days of the first assessment, or before discharge from the ICU, whichever was earlier. Patients who were intubated between the first and second assessment were excluded from the study.
In addition to RCSQ data, demographic data including patients’ age, sex, co-morbidities before hospitalisation, provisional diagnosis, and severity of the illness at admission as measured by the Sequential Organ Failure Assessment (SOFA) score were also recorded.
Statistical Analysis
IBM SPSS Statistics for Windows, Version 23.0, was used to evaluate the obtained data. For categorical variables, frequency analysis and percentage analysis were used, and for continuous variables, the mean and standard deviation were used. The Paired sample t-test was used to assess the bivariate samples in Paired groups. In each of the statistical methods, the probability value of .05 is regarded as significant.
Results
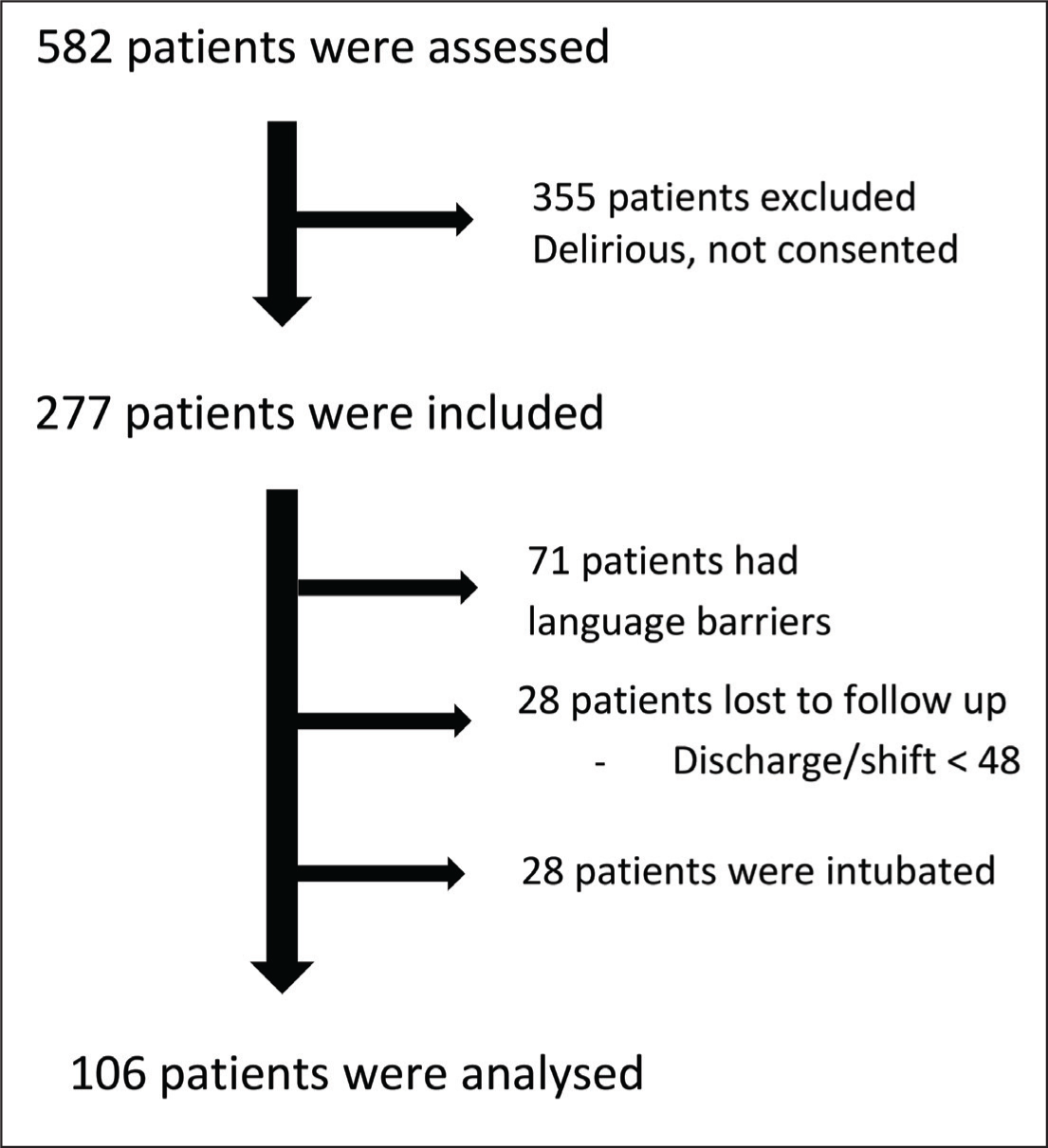
A total of 582 patients were screened, of whom 355 were excluded due to delirium and/or refusal to consent. Among 227 patients who met the inclusion criteria, 71 had language barriers, 28 had been lost to follow up and 22 patients got intubated and were excluded from the study. Hence, data collected from the remaining 106 patients were included for analysis [Figure 1]. Table 1 presents the baseline characteristics of the patient.
Sample size
Baseline characteristics of patients
Patient Demographics
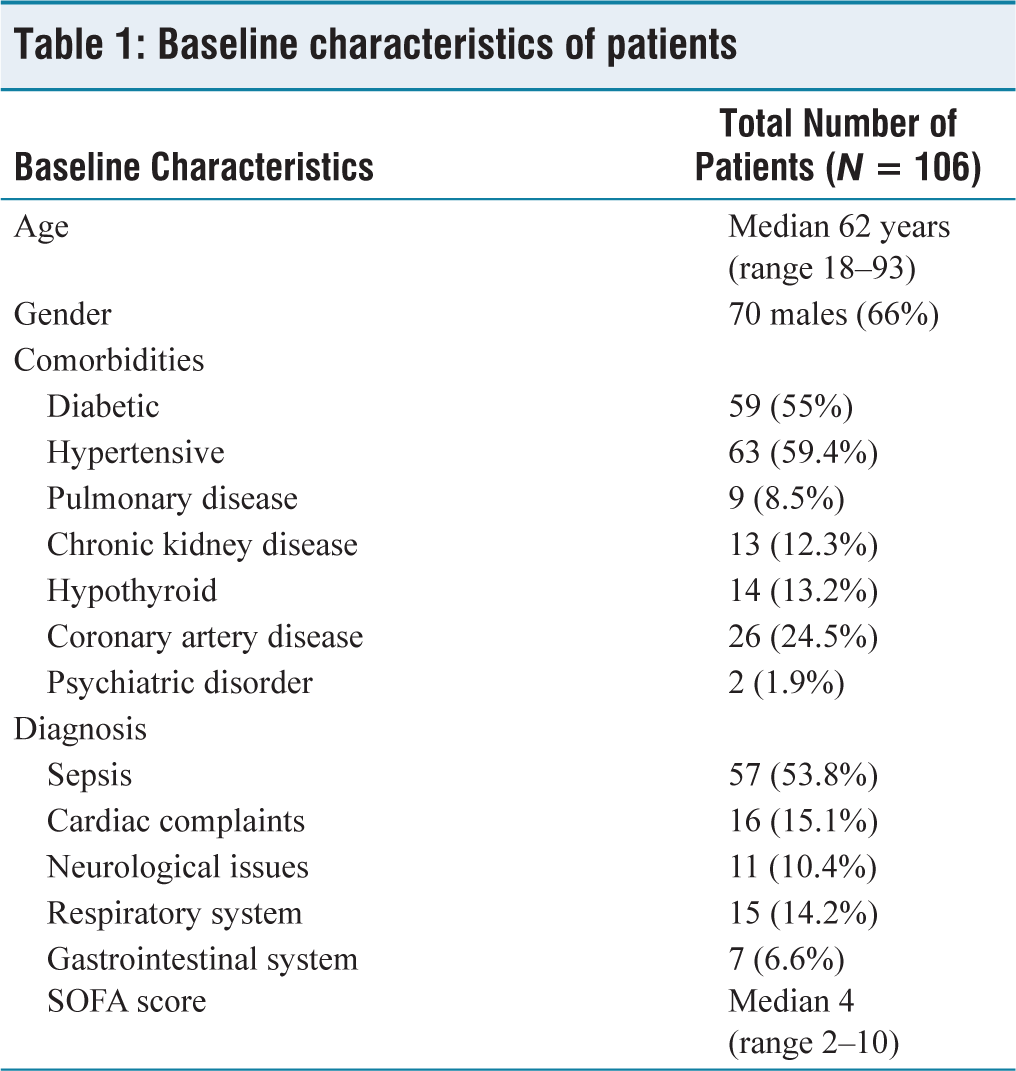
The median age of the patients was 62 years, with a range of 18–93, and 66% of our patients were males. The common comorbidities include diabetes (55.7%), hypertension (59.4%), COPD (8.5%), chronic kidney disease (12.3%), hypothyroidism (13.2%), coronary artery disease (24.5%) and psychiatric illness (1.9%). Among the study population, 53.8% of patients were admitted for sepsis. Others were admitted with cardiac ailments (15.1%), neurological disorders (10.4%), respiratory failure (14.2%) and gastrointestinal disorders (6.6%). The mean SOFA score of the study population is 4 (range 2–10).
Patient Perception of Sleep
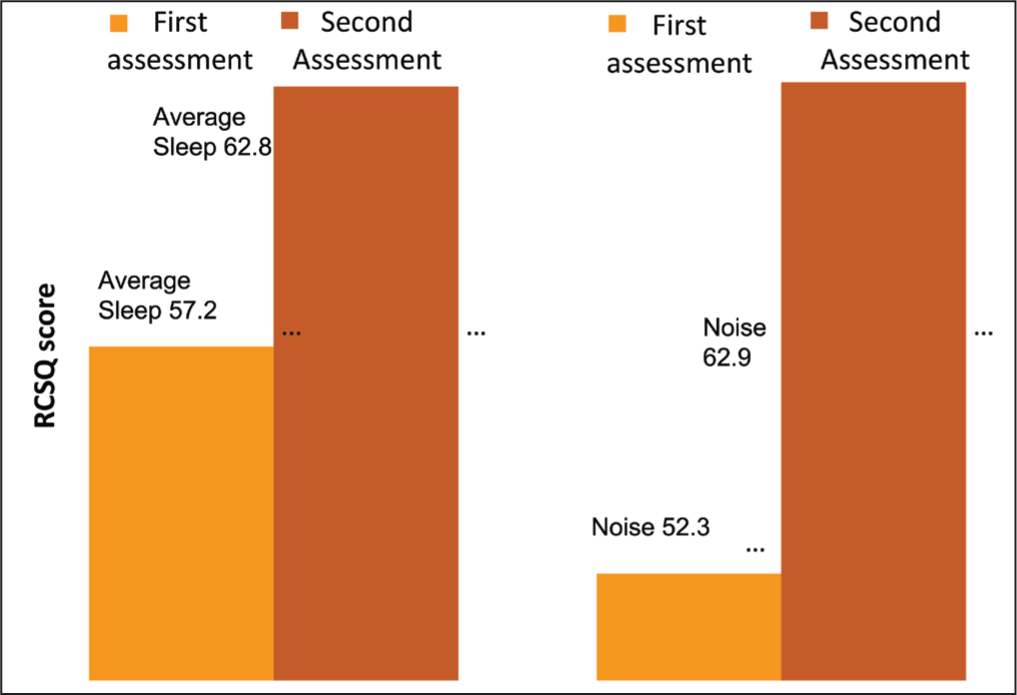
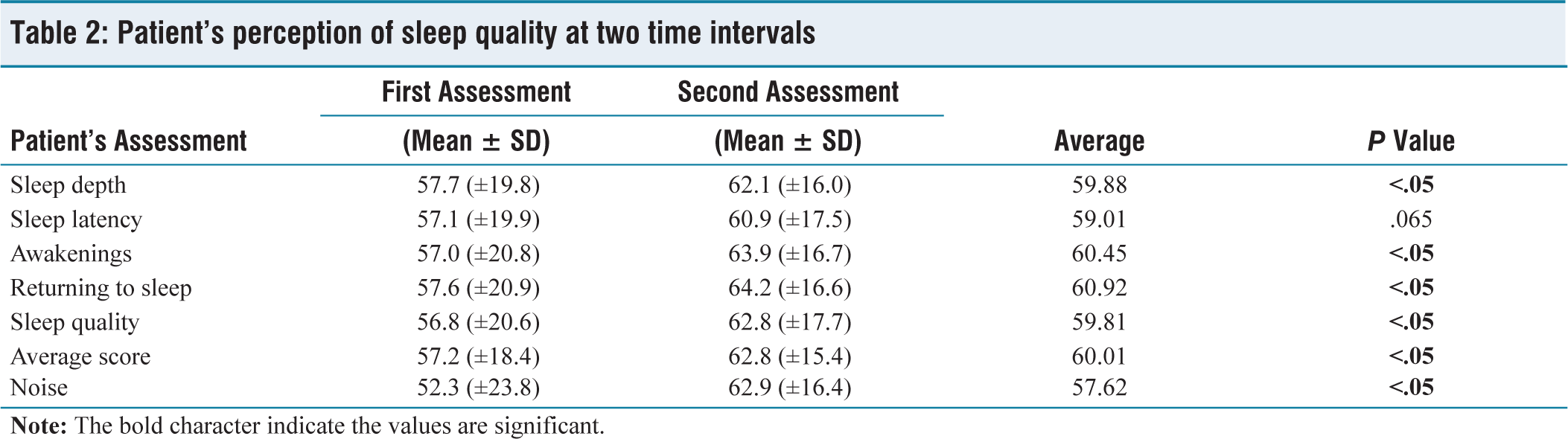
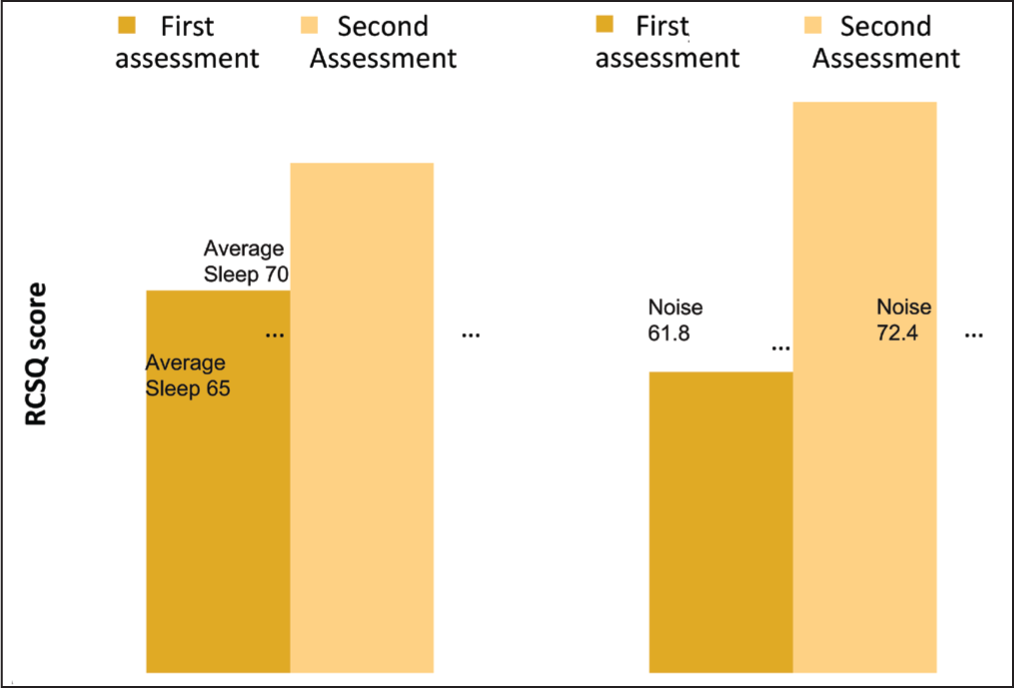
On analysing the patient’s sleep score, the first assessment showed a sleep score of 57.2 (±18.4) and the second assessment showed a significant increase in the sleep score to 62.8 (±15.4) (P < .05). It was noted that all the parameters of the sleep were affected to the same extent [Table 2]. Also, the assessment of noise showed a significant increase in the second score compared to the first one [62.9 (±16.4) vs. 52.3 (±23.8)] (P < .05), probably due to reduced perception of noise by the patient over time [Figure 3].
Average score of patient versus nurse’s assessment
Patient’s assessment over time
Patient’s perception of sleep quality at two time intervals
Nurses’ Perception of Sleep
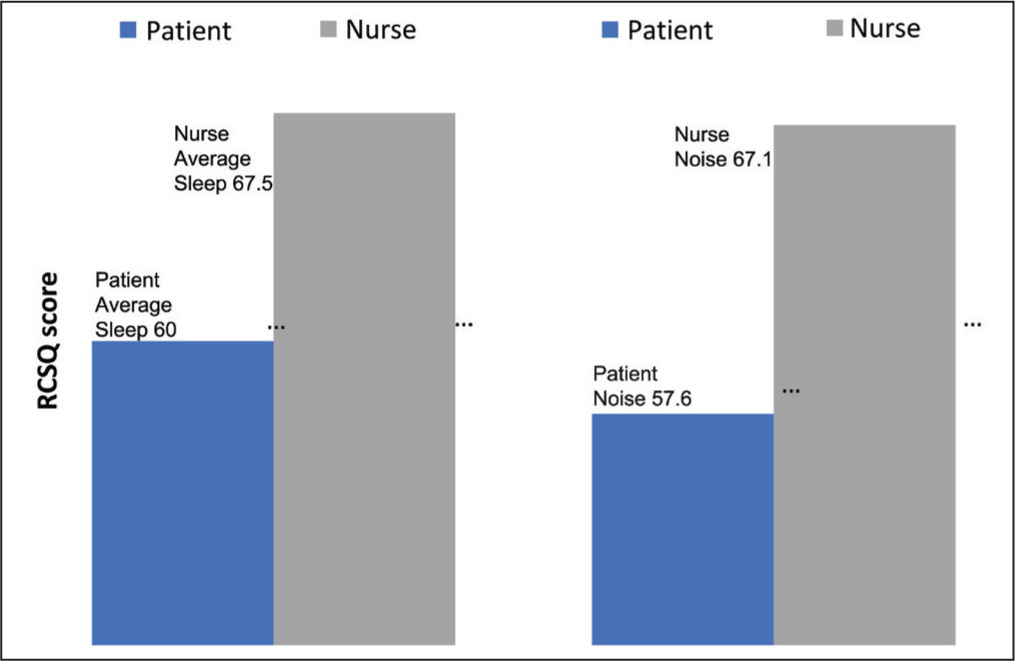
The nurses’ RSCQ score on the first and second assessment was 65 (±19.4) and 70 (±12.0), respectively, suggesting improved quality of sleep over time [Figure 4]. The noise perception by nurses also showed a similar trend with noise scores increasing from the first assessment to the second assessment [61.8 (±26.1) vs. 72.4 (±15.8)]. Hence, the nurses perceived an improved quality of patients’ sleep and decreased perception of noise over time during the ICU stay.
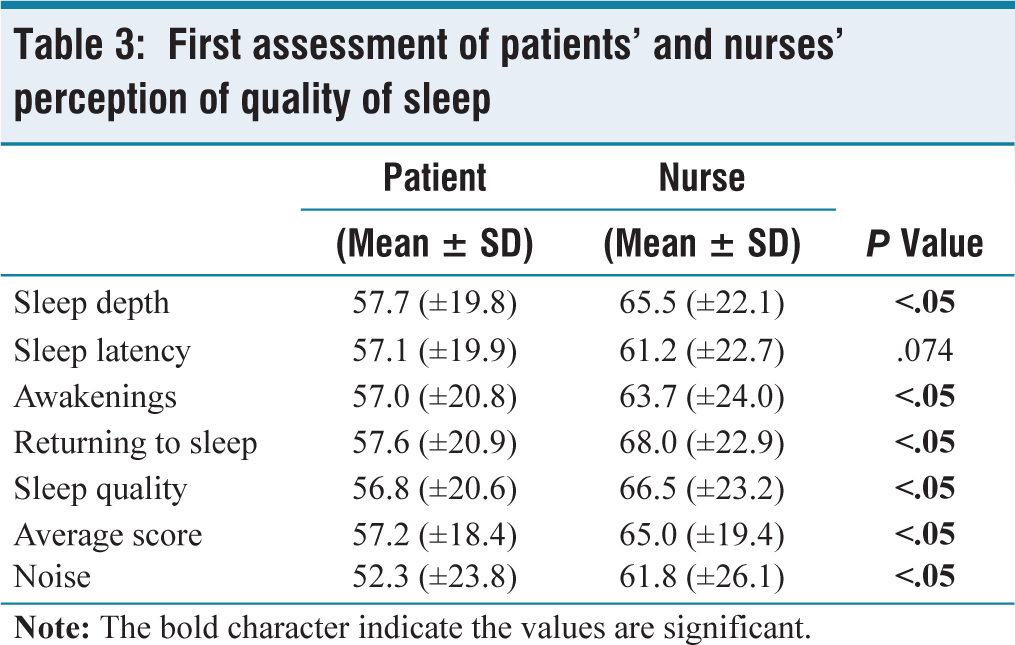
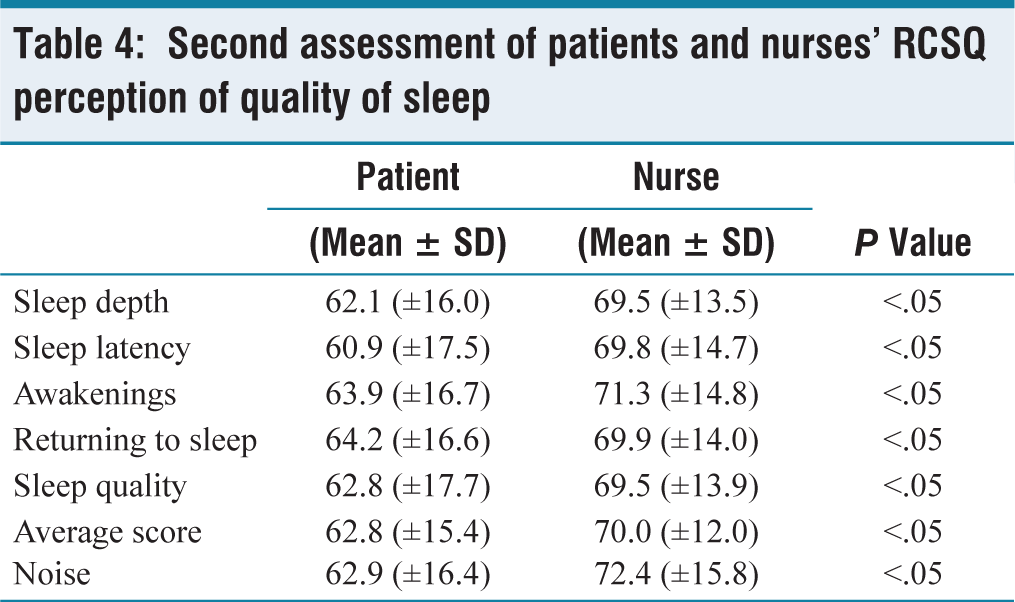
The patients’ and nurses’ perception of sleep were compared at two time intervals [Figure 2, Tables 3 and 4]. In both instances, the RCSQ scores of nurses’ assessment were significantly higher than those of patients’ assessment. Except for the sleep latency in the first assessment, the difference was noted in all the parameters of sleep, with nurses overestimating the quality of sleep. The patients’ assessment of noise too differed from that of the nurses. The noise perception scores in both assessments suggest less perception of noise by nurses compared to patients.
Nurse’s assessment over time
First assessment of patients’ and nurses’ perception of quality of sleep
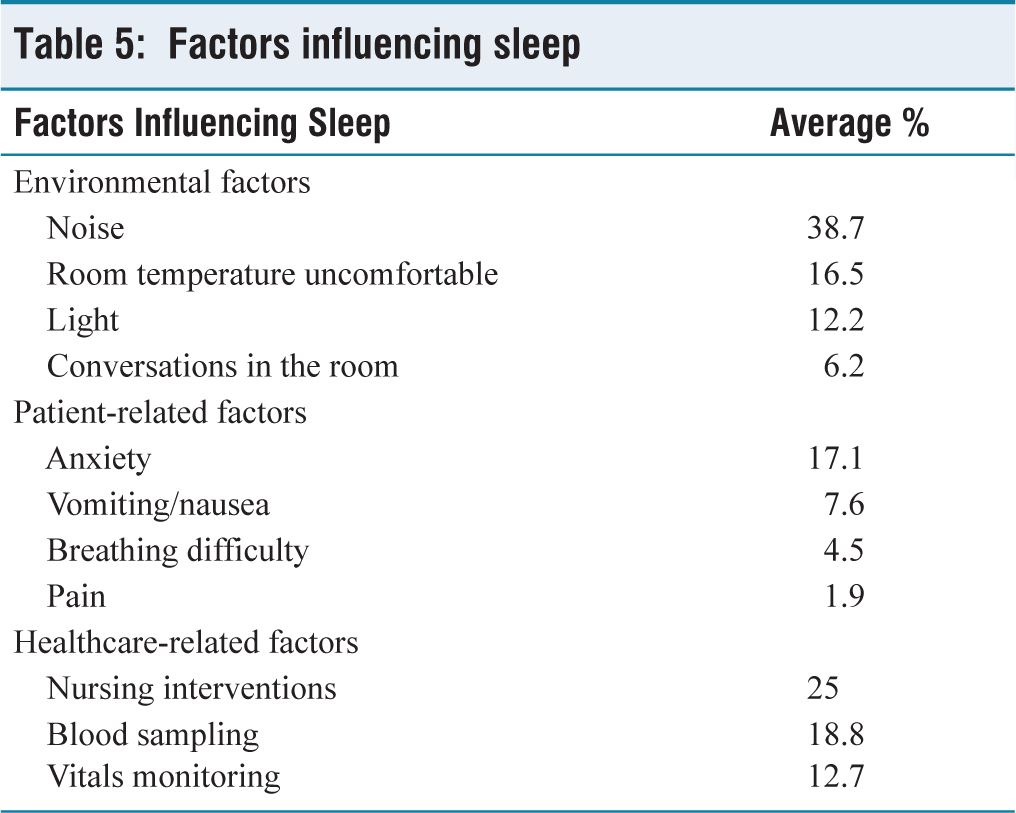
In our study, we evaluated various factors affecting sleep, including the environmental, patient-related and healthcare-related factors and the results are tabulated in Table 5. Among all the factors, noise was the predominant disruptor of sleep. Other factors influencing patients’ sleep include nursing interventions, blood sampling, anxiety of the illness, uncomfortable room temperature and measurement of vitals.
Second assessment of patients and nurses’ RCSQ perception of quality of sleep
Factors influencing sleep
Discussion
Sleep is essential for the physical and psychological well-being of patients, especially in the critical care unit. Multiple factors in the critical care units can affect the quality of sleep. Evaluating sleep quality and identifying the factors affecting it are the essential initial steps in improving the quality of sleep in critically ill patients admitted to ICUs. Patients requiring mechanical ventilation frequently receive high doses of sedative medications as a part of care. Sedative medications could affect sleep and its assessment, and potentially confound the results of the study. Hence, only non-ventilated patients were included in our study. Also, the perception of the bedside care takers, especially the staff nurse, is vital in facilitating the sleep of the patients. Hence, the nurses’ perception of sleep quality was also assessed in our study. The patients were evaluated twice during ICU stay to validate the initial finding and to evaluate the change in sleep pattern while staying in the ICU.
The patient population in our study had a median age of 62 (range 18–93), and 66% of them were male patients. The patients included in our study had a mean SOFA score of 4 and were less sick compared to the patients evaluated by Biren B Kamdar et al.[16] (mean SOFA of 6). This is probably due to the exclusion of mechanically ventilated patients in our study.
The patients in our study had a moderate quality of sleep with an average RCSQ score of 60. This is comparable to other studies,[16,18,21,22] which also showed a moderate quality of sleep among their patient population, with the mean RCSQ scores in the range of 45–62.
Our study is unique in having paired assessments of the patient and the nurse RSCQ scores at two different time periods to evaluate the trend of sleep quality during ICU stay. The reduced noise perception over time among the patients demonstrated in our study probably improved the quality of sleep over time in our study population. This phenomenon of adaptation to noise among ICU patients was noted in prior studies, which showed a progressive increase in the auditory threshold and a change in perception of noise during their stay in the ICU.[23,24]
The simple bedside RSCQ tools have numerous limitations, including reliability and recall bias. To overcome these limitations, the nurse’s assessment of quality of sleep was evaluated in our study. In our study, the nurses’ scores were higher for the patient’s sleep in both assessments [Tables 3 and 4], indicating overestimation of sleep by the nurses. The studies on nurses’ perception of patients’ sleep quality showed conflicting results. Frisk et al. showed better perception of sleep quality by nurses and pointed out the limitation of RSCQ, with over half of the patients unable to the patients to complete RSCQ.[18] In contrast, Biren B. Kamdar et al. and Ana Nicolas et al. showed poor perception of patients’ sleep quality by nurses, with nurses overestimating the quality of patients’ sleep in their studies.[16,25] This overestimation of sleep in patients by nurses was highlighted by Richard S Bourne in his review on the methods of sleep assessment in acutely ill patients.[26] Also, the nurse perceived lower noise levels compared to the patient. The difference in the noise perception between the patient and nurse is probably due to the acclimatisation of the nurse to the noise levels in the ICU.
On the assessment of factors affecting the quality of sleep in our ICU patients, noise was noted to be the predominant factor affecting the quality of sleep. Our finding is consistent with other studies done previously.[27,28] Noise exposure affects the cardiac and respiratory muscle function by stimulating the sympathetic nervous system.[28] Efforts to minimise noise in the ICU, including reducing the volume of monitors, alarms, infusion pumps, and phone rings, were made to improve the quality of sleep.[29,30] In a small randomised study, Pureepat Arttawejkul et al. showed an insignificant improvement in the quality and quantity of sleep with simple interventions including the use of earplugs and eye masks.[31] The application of white noise by Williamson et al., in the post-surgical ICU, was shown to improve the quality of sleep in post-surgical patients.[28] Other factors, including room temperature, lighting, nursing interventions, blood sampling, vital monitoring and anxiety were also found to affect of quality of sleep in our patients.[13,28]
Our study is designed in a pragmatic way to assess the patients’ and nurses’ perception of the quality of sleep in our patients. Our study used a subjective, well-validated tool for the assessment of quality of sleep. The sample size in our study is the largest among the studies that evaluated sleep quality using RCSQ in the ICU. Our study is unique in having paired scores obtained twice in a predefined time interval during the study period, to ensure validity and consistency of the results. The study also looked into the major barriers to sleep in acutely ill patients.
Our study was done in a single centre, excluding mechanically ventilated and delirious patients, and thereby limits the generalisation of the results. As the RCSQ tool was not validated in local languages, patients who do not read/understand English were excluded from the study. In spite of early and timely applications of the questionnaire, the study has a potential risk for recall bias.
Conclusion
The non-ventilated patients admitted to the ICU had moderate quality of sleep. The nurses tend to overestimate the sleep and underestimate the noise levels perceived by the patients. The sleep score of the patients improves, and the noise perception decreases over time in the ICU. Noise is likely to be the major factor causing sleep disruption.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
AMH-DNB-006/02-20.
Informed consent
Not applicable.
Credit author statement
Gerard Joseph Gonsalvez: Conceptulisation, methodology, writing—original draft.
Gowtham Kannan: Investigation, resources.
Nagarajan Ramakrishnan: Formal analysis, validation, supervision.
Ramesh Venkataraman: Formal analysis, writing—review and editing.
Vignesh Chandrasekaran: Methodology, data curation, writing—review and editing.
Data availability
Data available on request.
Use of artificial intelligence
None.