
Abstract
Background:
The Percheron artery (APn) is an uncommon anatomical variation wherein the bilateral medial thalami are vascularised by a predominant thalamoperforating artery, as initially described by Frances Gerard Percheron in 1973. This study aims to clarify the mechanism of infarction by analysing the clinical characteristics and common locations of the APn.
Materials and Methods:
This narrative review attempted to summarise 140 publications regarding the APn, encompassing its surgical treatment, diagnosis, complications, and prevalent demographic data, searching ScienceDirect and PubMed/MEDLINE. Subsequently, utilised software such as Excel and Rayyan, an intelligent system. The investigation encompassed publications from January 2010 to June 2024.
Conclusion:
The study demonstrates that APn arteries are rare yet appear with noticeable and common symptoms affecting the paramedian thalamic arteries on both sides. Identified lately as a variant artery, it is connected with many clinical diseases. We advise rapid magnetic resonance imaging (MRI) diagnosis, coupled with patient examination, to diagnose APn infarction.
Abbreviations
ICU: Intensive care unit
tPA: Tissue plasminogen activator
DWI: Diffusion-weighted imaging
PCA: Posterior Cerebral Artery
AOP: Artery of the Percheron
CSF: Cerebrospinal fluid
FLAIR: Fluid-attenuated inversion recovery
Introduction
The Percheron artery (APn) is classified as a rare and unusual variation in which the bilateral medial thalami receive their supply from a dominant thalamoperforating artery, which differs in its contribution to the rostral mesencephalon. proposed by physician and scientist Frances Gerard Percheron in 1973. He was born in the French city of Pavilly. In the middle of the 1930s–2011. He was an expert researcher and scientist at the Institut National de la Santé et de la Recherche Médicale, where he participated in and performed research. His work on the vascular anatomy of the thalamus and basal ganglia, which led to the identification of the artery now known as the Percheron, was one of his important achievements. It can be blocked or display a pattern of ischemia, such as paramedian thalamic infarcts, with or without involvement of the midbrain.[1] The APn thalamus-perforating artery (PDA), which may or may not signal a midbrain infarction, develops from the P1 section of the posterior cerebral artery. Clinically, the lesions are associated with memory impairment, supranuclear vertical gaze palsy, and impaired awareness.[2] Similar to PDA, there are various forms of infarcts that impact the same locations. For example, bilateral thalamic lesions in deep cerebral vein thrombosis with the syndrome in its upper part of the base, or the upper part of the basilar artery syndrome, which affects the bilateral paramedian thalamic regions and is impacted if the basilar artery is clogged.[3] The neighbouring area is supplied by the posterior cerebral arteries, the superior cerebellar artery, and the pontine arteries. Venous sinus thrombosis, which can lead to obstructions of the internal cerebral veins, should also be taken into account. Headaches, vomiting, and papilledema are the clinical indications of cervical venous thrombosis. These symptoms may lead to a heart attack, which may cause seizures and focal neurologic abnormalities such as aphasia. Because Wernicke’s encephalopathy can create lesions in the bilateral thalami, periaqueductal grey plate, dorsal column, and mammillary bodies, we have included it as a differential diagnosis. It is only vital to emphasise that infections and osmotic myelinosis should be considered in this differential diagnosis.[4] Bilateral paramedian thalamic infarcts, which account for only 20% of thalamic infarcts, may occur from (APn) blockage in the midbrain and are seen in 0.1%–0.3% of infarcted patients.[5]
The purpose of this study is to clarify the mechanism of infarction through an analysis of the clinical features and location, more commonly of the APn. This will be achieved by the clinical and radiological diagnosis based on anatomical criteria, of the probability of surgical repair based on the results.
Materials and Methods
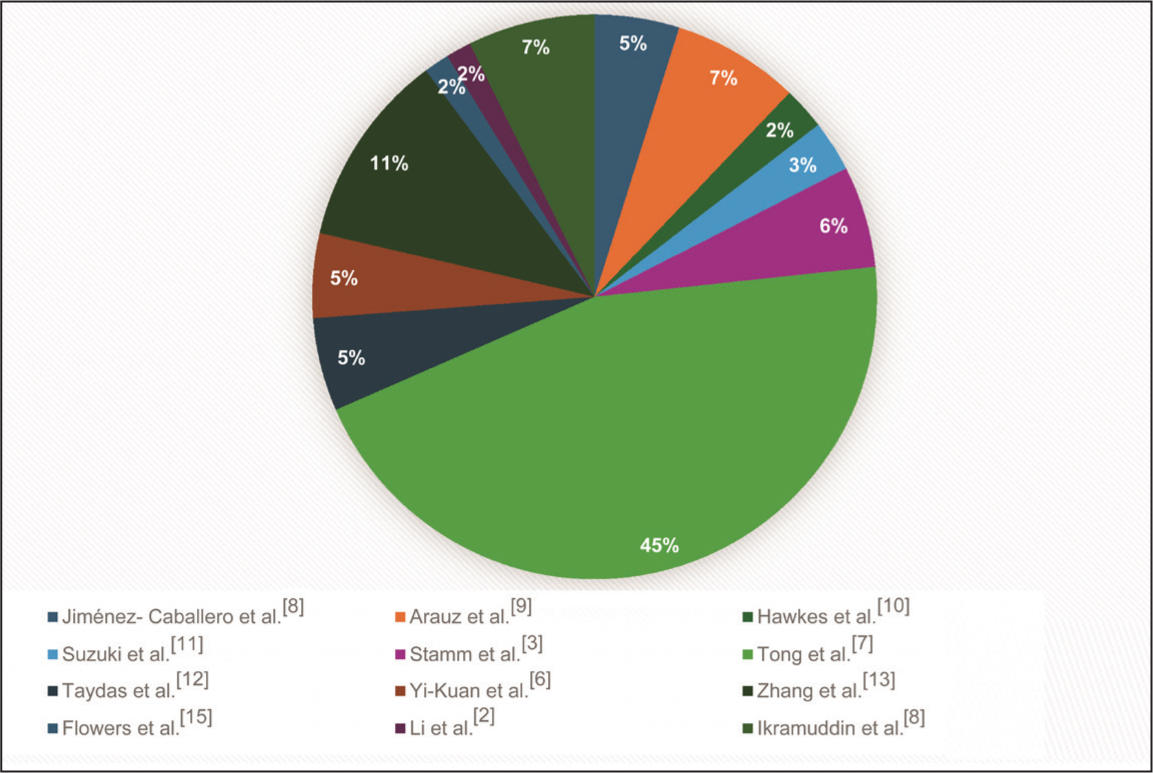
A complete assessment of the review scientific literature on the APn and its surgical therapy, diagnosis, complications, and common demographic information was undertaken in accordance with the criteria and standards. The search phrases ‘Artery of Percheron, occlusion, infarcts, or bilateral paramedian thalamic infarction’ were applied to discover pertinent literature within the Science Direct and PubMed databases, in addition to EMBASE, Google Scholar, and Cochrane reviews. The Excel criteria and Rayyan (intelligent system software) were also applied. The search was conducted on publications published from the earliest known date up to January 2010 till December 2024. This review of 140 articles revealed that 221 patients with APn infarction were included in the study [Table 1]. The images and tables offered in this inquiry, notably Figures 1–3 and Tables 2 and 3, contain investigations on pathological disorders that affect and impact the APn [Figures 1–3].
An analysis of research on Percheron artery infarctions based on patient location and symptomatology comparability
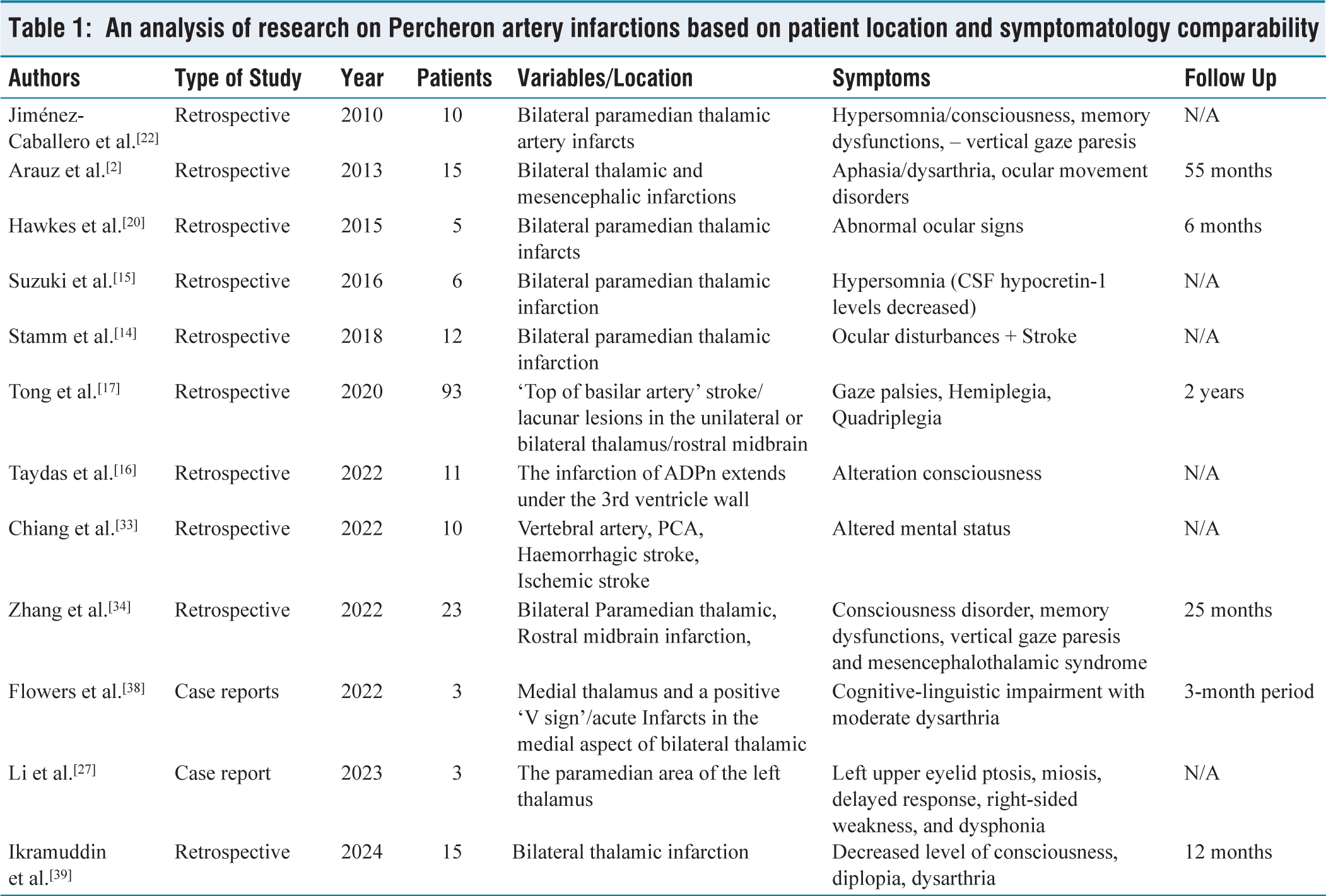
Clinical manifestations and most frequent sites of Percheron artery infarctions
(A) MRI image, with intensity in the paramedian thalamus, with FLAIR sequence, blue arrow. (B) MRI image of the contralateral paramedian thalamus with T2 sequence, noted in orange arrow; (C) normal circle of the Willis; (D) abnormal variant artery of Percheron

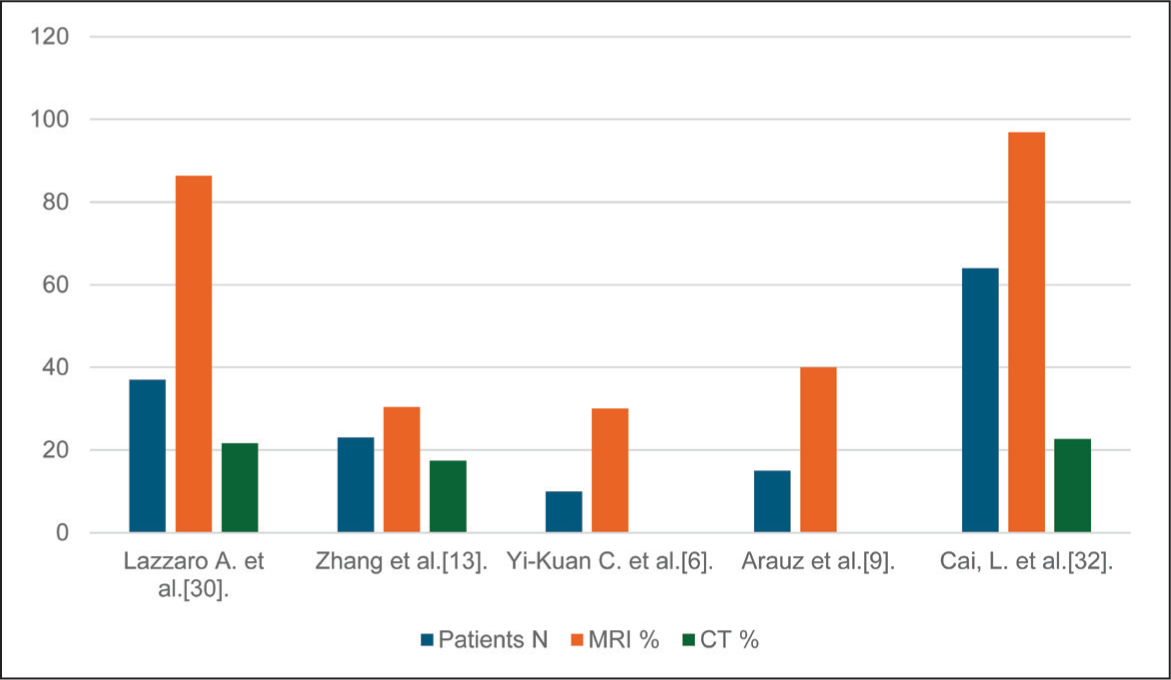
The presence of Percheron artery infarction confirmed on MRI-CT
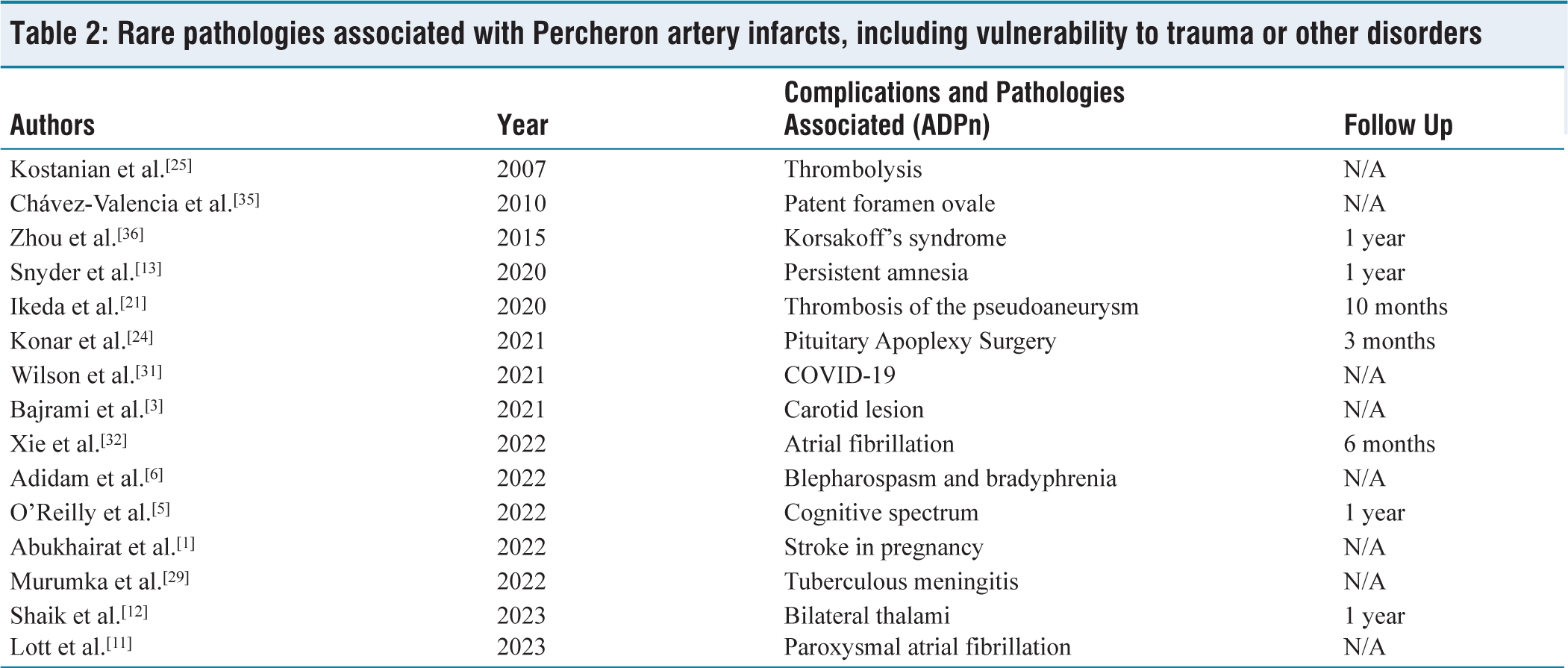
Rare pathologies associated with Percheron artery infarcts, including vulnerability to trauma or other disorders
Studies confirm the presence of Percheron artery infarcts, confirmed by MRI and CT images

Anatomy of the Thalamus, Stroke Region of the Artery of Percheron
Given the extensive discourse surrounding the irrigation of the thalamus, a macroscopic research initiative was undertaken, encompassing the administration of limited injections in over 50 hemispheres. The material was divided into three sections.
It referred to the three points highlighted by the macroscopic anatomical analysis of the origin segment in the thalamic branches: (a) The section of the arterial wall that connects the basilar artery’s union to its terminus was isolated. This artery serves to communicate posteriorly. The term ‘communicating basilar artery’ was proposed. The point marked by the Willis circle represents the point of origin of the posterior cerebral artery. (b) The terminal end of the choroidal artery exhibits considerable variation, though it is more frequently located ventral to the thalamus. (c) Given the intricate nature of the posterior choroidal artery system and the paucity of existing knowledge regarding it, it is imperative to emphasise the arterial systems that facilitate diverse organisational structures. In addition to the aforementioned variations, the postero-medial mesencephalo-thalamo-choroidal system and, on occasion, a single posteromedial choroidal artery may also be observed.[6]
The thalamo-choroidal-hippocampal posterior system is a complex network of interconnected structures. A single posterolateral choroid artery represents just one of numerous possible arrangements, which serves to further complicate the matter. The arterial territories and thalamic arteries: (a) In this method, the middle cerebral artery is deemed unimportant. (b) Because there is no pedicle formed ventrally, the choroidal artery is not a part of the choroidal pedicle’s constitution and does not supply the dorsal section of the thalamus. This artery in the thalamus is irrigated by a sporadic and restricted overflow of the pallidal-capsular region. (c) The anterior pole of the Formatio Lateralis is included in the region of the posterior communicating artery, also known as the thalamic polar artery, which emerges from a single thalamic branch. (d) The paramedian thalamic artery, which connects to the variable polar artery and the mesencephalic paramedian arteries, is one of the two thalamic branches that arise from the connecting basilar artery.[6]
The posterior connecting artery, which is devoid of thalamic branches, is present in the polar area. It is possible that the thalamic paramedian arteries may originate from the connecting basilar artery on both sides. The short branches of the posterior cerebral artery’s trunk exhibit considerable diversity. The first group comprises the inferior thalamic arteries, which have their origin in the posterior ventral region of the Formatio Lateralis. The inferomedial aspect of the nucleus arcuatus is not supplied by the aforementioned artery. The inferolateral pulvinar arteries constitute the final group. The posteromedial choroidal system is characterised by the presence of two distinct types of arteries. The first of these is the inferolateral oblique thalamic artery, which courses inferiorly towards the inferomedial aspect of the arcuate nucleus. The second is a ventral group of arteries that constitute the medial geniculate arteries. This second group has yet to be described in detail. In addition, there is a third group consisting of the pulvinary arteries inferomedially, as well as the posterocentral thalamic artery, which is a unique artery that extends both posteriorly and superiorly. The lateral geniculate arteries have their origin in the posterolateral choroidal system. In addition to this, there are further groups of arteries, namely the inferolateral and superolateral pulvinary arteries, along with the superolateral thalamic arteries that reach the dorsal portion of the Formatio Lateralis. As outlined by Percheron et al.[6–17]
Clinical Manifestations of APn Infarction
It is well established that the four clinical manifestations of the artery of Percheron, namely vertical gaze paralysis (65%), memory impairment (58%), confusion (53%), and coma (42%), are dependent on the blood supply. Furthermore, the structures and functions of ADPn can exhibit complex relationships due to their variable vascular anatomy. It is also important to note that comas associated with the artery of Percheron can be highly variable, with patients experiencing periods of diminished consciousness that may last for several hours or even days. As the collateral circulation develops and the oedema in the ischemic brain tissue reduces, consciousness gradually returns.[6–31]
Image Analysis and Magnetic Resonance Imaging (MRI)
The imaging protocol comprises a T1-T2 axial-weighted spin echo with additional scans, a T2 fluid-attenuated inversion recovery (FLAIR) sequence, and diffusion-weighted imaging (DWI). Many radiologists employed DWI, FLAIR, and T2-weighted imaging to identify and highlight specific lesion sequences. In clinical practice, the DWI signal’s maximum intensity and the diffusion coefficient maps’ lowest intensities, which were presumably regarded as acute infarcts, were identified as the most significant areas.[32]
Furthermore, a full analysis of fifteen individuals proved to have APn infarcts. However, this study, performed retrospectively between 2014 and 2022, revealed that the most common clinical presentations were systolic blood pressure (SBP) >140 in 12 patients, decreased consciousness in 11 patients, diplopia in 8 patients, disorientation in 6 patients, dysarthria in 4 patients, and impaired memory in 4 patients.[18] A 10-year research study was undertaken on APn infarcts, based on the clinical and radiological findings of 15 patients. The scans were characterised as bilateral paramedian thalamic with rostral midbrain infarction, as well as without midbrain infarction. The patients’ altered state of consciousness included aphasia, dysarthria, ocular movement problems, motor deficiency, and altered cerebellar signals. Furthermore, the photos were appraised using the Rankin scale.[7–15,19–30] In a further study conducted retrospectively between 2010 and 2019, the authors reported that 90.9% of patients had patterns or radiological evidence indicative of asymmetric ischemia damage in 11 patients with APn infarctions. Of the patients, eight had hypertension, five had coronary disease, and eight had ADPn infarcts, with 72.3% reaching below the third ventricle wall.[7–16,20–30]
In a further analysis, only 18 patients with Pecheron artery infarctions (APn) were found to have this pathology at the time of admission (P < .05), out of 6,539 stroke patients evaluated by the National Institutes of Health (NIHSS) and the Acute Physiology and Chronic Health Evaluation II (APACHE II). Given that the majority of cases have an unfavourable outcome or poor prognosis, it is important to consider the potential impact of midbrain lesions with a higher infarct volume and increased haemorrhagic production. The primary symptoms included dizziness, transient blurred vision, double vision, botulism, cerebellar ataxia, somnolence, and coma. Three subtypes of artery of Percheron symptoms have been identified: (a) bilateral anterior and paramedian thalamic infarction without midbrain involvement, (b) bilateral paramedian thalamic infarction with midbrain involvement, and (c) bilateral paramedian thalamic infarction without midbrain involvement. From the time of stroke onset until the Glasgow scale score, patients with current smoking, hypertension, diabetes, hyperlipidaemia, hyperhomocysteinaemia, and heart disease exhibited certain characteristics that did not differ significantly from those observed in patients with favourable and unfavourable outcomes.[6,17,31,32,37]
Discussion
The artery of Pecheron is classified as one of the variations of the paramedian artery, which supplies the midbrain and the paramedian region of the thalamus on both sides of the brain via a single arterial trunk that arises from the posterior cerebral arteries. A comparative study was conducted between the Pecheron artery and the occurrence of both temporary and persistent coma. A total of 93 patients met the inclusion criteria, as they exhibited symptoms indicative of stroke or lacunar lesions in the thalamus or rostral midbrain in a unilateral or bilateral manner. It is notable that the symptoms and coma themselves receded following the administration of the treatment, a phenomenon that can be observed from both a clinical and anatomical perspective.[17] It is estimated that 4%–18% of all thalamic infarcts and 0.1%–2% of all strokes are caused by this variation, which affects 33% of individuals with the artery of Percheron infarctions.[10] The initial therapy for acute ischemic stroke will vary depending on the patient’s thrombolytic contraindications at the time of injury. The optimal treatment for occlusion of a proximal cerebral artery is a recombinant tissue plasminogen activator, administered during the first 4–5 hours after onset, in conjunction with mechanical thrombectomy within less than 6 hours. It is recommended that patients receive aspirin and clopidogrel antiplatelet therapy in the event of underlying cardioembolic events.[9] Some research indicates that diffusion-weighted MRI is the optimal method for diagnosing acute infarctions caused by the artery of Percheron. However, interval reviews are recommended in the event that the MRI does not yield useful radiological patterns or data. In such cases, the patient’s clinic should be consulted. Given the rarity of the APn. Cerebral angiography would not be an adequate diagnostic method. Consequently, an infarction of the artery of Percheron may be postulated based on the symptoms. To diagnose the artery of Percheron (APn), MRI can provide a definitive answer, given that it is an anatomically rare and little-discussed variant. It is conceivable that a considerable number of emergency physicians may not initially be cognizant of this possibility, or that the diagnosis may emerge at a later stage. Nevertheless, to exclude the possibility of haemorrhages and to administer the most appropriate therapy with intravenous thrombolysis, it is necessary to perform a computed axial tomography of the brain when there is a suspicion of an infarction in the posterior circulation region. The early detection of basilar artery obstruction is advantageous for the purposes of reperfusion and recanalisation, which may be achieved through the use of intravenous or intra-arterial thrombolysis. The treatment of APn blockage is via acute endovascular thrombolytic therapy, which has the effect of improving both picture quality and clinical outcomes in less than a day; the professionals should look into this medication for a better treatment of this kind of patient with this pathology.[8]
An analysis was undertaken at a Taiwanese hospital between 2009 and 2020 based on MRI data. The study comprised 10 individuals who had sustained acute bilateral paramedian thalamic infarcts arising from APn infarcts. The patients were grouped according to the level of territorial involvement, as assessed by the patient’s APn infarction, using the highly modified Rankin scale. Based on angiography, just one case indicated both vertebral and basilar obstruction, while 90% of patients demonstrated a changed mental status. Two individuals revealed bilateral vertebral arteries, while five demonstrated unilateral posterior cerebral arteries.[35]
An additional study was undertaken from 2012 to 2015 on 918 patients across a three-year period when they were in acute coma. The study focused on the evolution of temporal damages after rising from an acute ischemic coma produced by the Percheron artery. The study comprised three groups: 93 patients with APn infarction, 234 with ischemic strokes in the anterior cerebral artery, and 559 with haemorrhagic strokes. Monitoring of the development of these transitory lesions was undertaken utilising high- or powerful-power diffusion imaging (DWI) techniques. Consequently, 90 patients developed either permanent or transient APn infarction, in addition to unconsciousness. Patients who had undergone a stroke at the upper level of the basilar artery demonstrated damage to both sides of the paramedian thalamus and the bilateral rostral midbrain.[7–31]
Risk Factors
In accordance with the classification system for brain illnesses, occlusions of the smaller arteries, lacunar haemorrhage, and cardioembolism are identified as the causes of an ADPn infarction. The occurrence of cardiac embolism is associated with several risk factors, including hypertension, diabetes, smoking, malignancies, inflammation, coagulation disorders, hypotension, and illnesses of the tiny blood arteries. The dissection of the basilar and vertebral arteries, in addition to basilar aneurysms, constitutes a risk factor for APn.[27]
Prognosis and Treatment
A review of the literature reveals that 65% of patients with this specific paramedian thalamic infarction of the APn have a favourable prognosis, with some cases demonstrating complete recovery. At present, recanalisation is recommended as a treatment option for acute PDA blockage. In instances where a head CT scan exhibits no evidence of oedema or cerebral bleeding within the initial six-hour period, patients are subjected to thrombolytic treatment. The time threshold for thrombolytic therapy, which is believed to be the optimal period for treating acute myocardial infarction, has been established to be between 4.5 and 6 hours. In cases where thrombolytic therapy is not an option for patients due to contraindications, heparin and antiplatelet therapy should be administered for a minimum of six hours. To prevent recurrence, the majority of patients should be administered oral anticoagulants.[34]
Limitations and Future Directions
From an anatomical, symptomatic, diagnostic, and therapeutic perspective, the APn represents an intriguing cerebral manifestation. However, there is a paucity of retrospective or random studies on the subject, which makes it challenging to locate an impressive case report or large-scale, widely reported manifestation of this pathology. Nevertheless, this study aimed to focus on the aforementioned characteristics. Future guidelines will attempt to classify this defective auxiliary variable artery with its numerous particularities or clinical presentations based on the diagnosis, as it is a manifestation of this pathology. It is recommended that the pattern of these clinical presentations be committed to memory so that the clinical image is available at the time of diagnosis and can be used to manage the pathology conservatively or surgically if necessary.
Conclusion
The findings of this study indicate that although the APn is uncommon, it frequently and clearly manifests clinically as symptoms that impair the paramedian thalamic arteries bilaterally. Given the relatively recent discovery of the APn infarction and its association with a multitude of pathological conditions, it is recommended that early detection be achieved through the use of MRI. This, in conjunction with the patient’s symptoms, provides sufficient evidence to diagnose the condition. Given that one of the primary symptoms is altered consciousness or cognition, including hypersomnia or, in the most severe cases, coma, a conservative approach is recommended, with aspirin plus clopidogrel prescribed based on proven results. In addition, a limited cognitive test evaluation for the state of consciousness is advised. However, it is commonly held that the APn is susceptible to a wide range of diseases and disorders, which leads us to consider stroke as a potential first scenario.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Ethical approval is not applicable to this article.
Credit author statement
DES, BC, KY: Conceptualisation, methodology, software.
GEC, DAES: Investigation.
DAES: Data curation.
GC, EC, IB: Supervision, visualisation, validation.
DAES: Writing - original draft.
DAES, IB, MA, MO, KY: Review & editing, formal analysis.
Data availability
It will be available upon reasonable request.
Use of artificial intelligence
No AI was used for this article.