
Abstract
An unexpected malposition of a testis can present a diagnostic dilemma in the interpretation of surveillance imaging for malignancies, especially in the pelvis and lower limb. Instances of dislocated or undescended testes (cryptorchidism) mimicking disease are sparsely described in the literature. We describe a case of testicular malposition in two young male patients with known lower limb soft tissue sarcomas. In the first case, surveillance MRI revealed a displaced testis mimicking sarcoma recurrence, with testicular dislocation occurring through an inadvertent surgical defect created during primary sarcoma resection. The second case reports misinterpretation of an undescended testis as inguinal nodal disease. Understanding these potential pitfalls when interpreting images in male patients with lower limb sarcomas presents both an opportunity to avoid unnecessary surgery and biopsy, plus preventing known complications of infertility, torsion and malignancy.
Keywords
Introduction
The typical causes of testicular malposition are congenital/developmental and trauma, the most common being cryptorchidism, which occurs through failure of normal testicular descent in the retroperitoneum and inguinal canal into the scrotum, and testicular retraction from a hyperactive cremasteric reflex. On rare occasions, ectopic testes have been reported in the perineum, femoral canal, superficial inguinal pouch, suprapubic area, or contralateral hemiscrotum.[1] Testicular dislocation is rarer still, and typically associated with scrotal or abdominopelvic trauma.[2,3]
We report cases of non-traumatic testicular dislocation into the adductor compartment following sarcoma resection from the proximal thigh and cryptorchidism within the inguinal canal in a patient with known contralateral lower limb soft tissue sarcoma.
The unexpected location of these testes was misinterpreted during surveillance and staging scans as potential recurrence and metastasis, respectively. Non-traumatic testicular dislocation is extremely rare,[3] and postsurgical cause in patients following normal testicular descent has, to the best of our knowledge, not been previously reported in the literature. A comprehensive literature search using the PubMed database revealed only one case of a non-traumatic testicular dislocation, occurring in the setting of cryptorchidism, with dislocation outside the inguinal canal.[3] Cryptorchidism is a relatively common entity[4] although there is only a solitary report that describes an undescended intrapelvic testis masquerading as a caecal mass.[5]
The entity could be overlooked on routine imaging, especially given the unexpected asymptomatic testicular malposition, as the imaging characteristics of a normal testicle can mimic a tumour or pathological lymph node. This article aims to raise awareness of this potential pitfall and emphasise the need to consider this entity in patients with an inguinal or adductor compartment mass, particularly in the setting of prior lower limb or pelvic malignancy.
Case Reports
Case 1
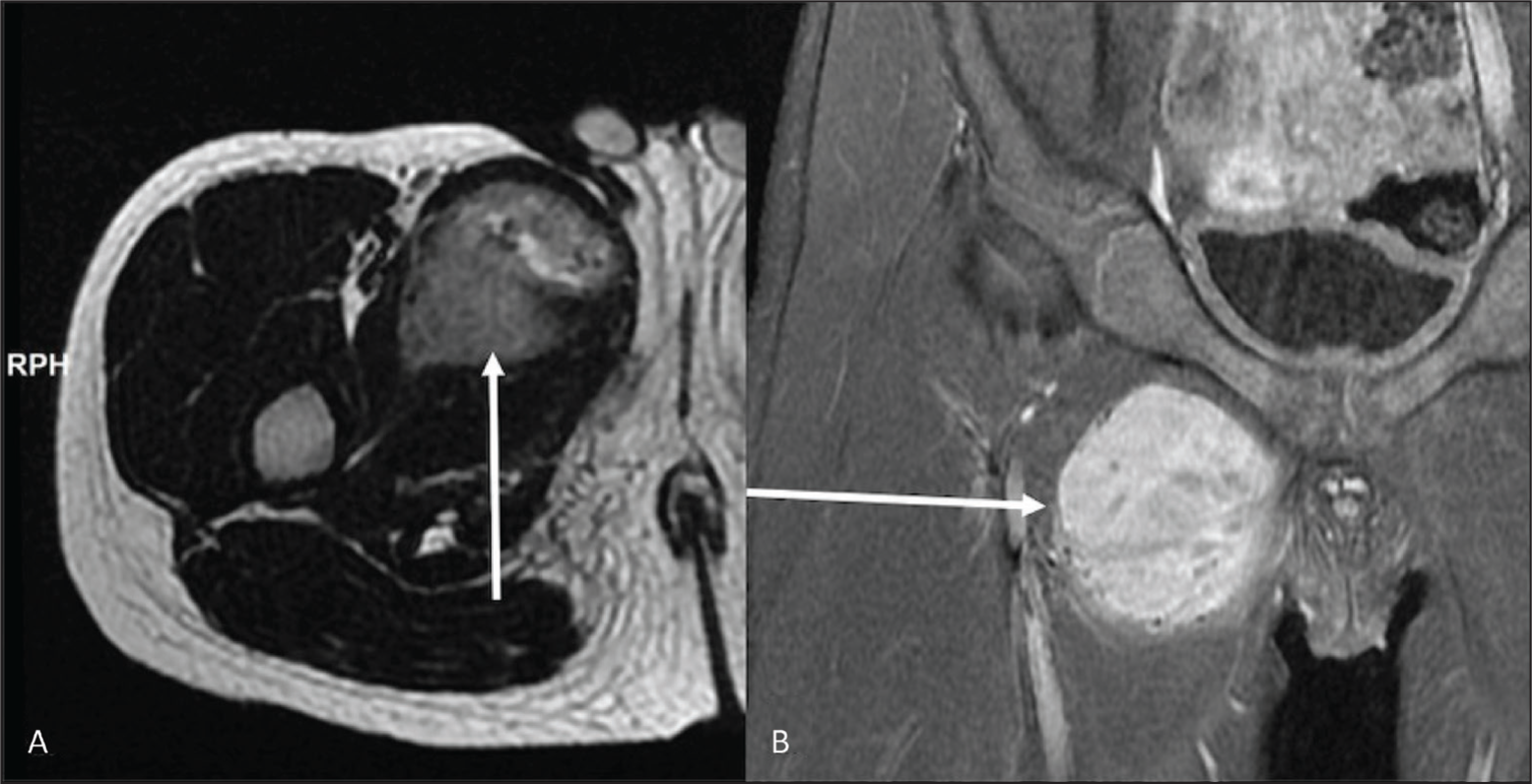
A 10-year-old male with prior dendritic cell sarcoma resection from the proximal right thigh adductor compartment [Figure 1A, B] excised four years earlier, presented with a proximal thigh mass identified on routine surveillance MRI [Figure 2A, B]. Excision required en-bloc oncological resection involving the mass and right pubic ramus requiring a rotational anterolateral thigh flap for primary soft tissue reconstruction. Postoperative surveillance had been clear of locoregional disease recurrence.
(A) Axial proton density (PD) and (B) coronal PD fat suppressed (FS) sequences of the upper thigh demonstrating the initial soft tissue sarcoma within the right adductor compartment (white arrows)
(A) Axial and (B) coronal PD FS MRI of the upper thigh shows a solid ovoid structure in the proximal right adductor compartment demonstrating uniform high fluid signal (white arrows) on surveillance MRI
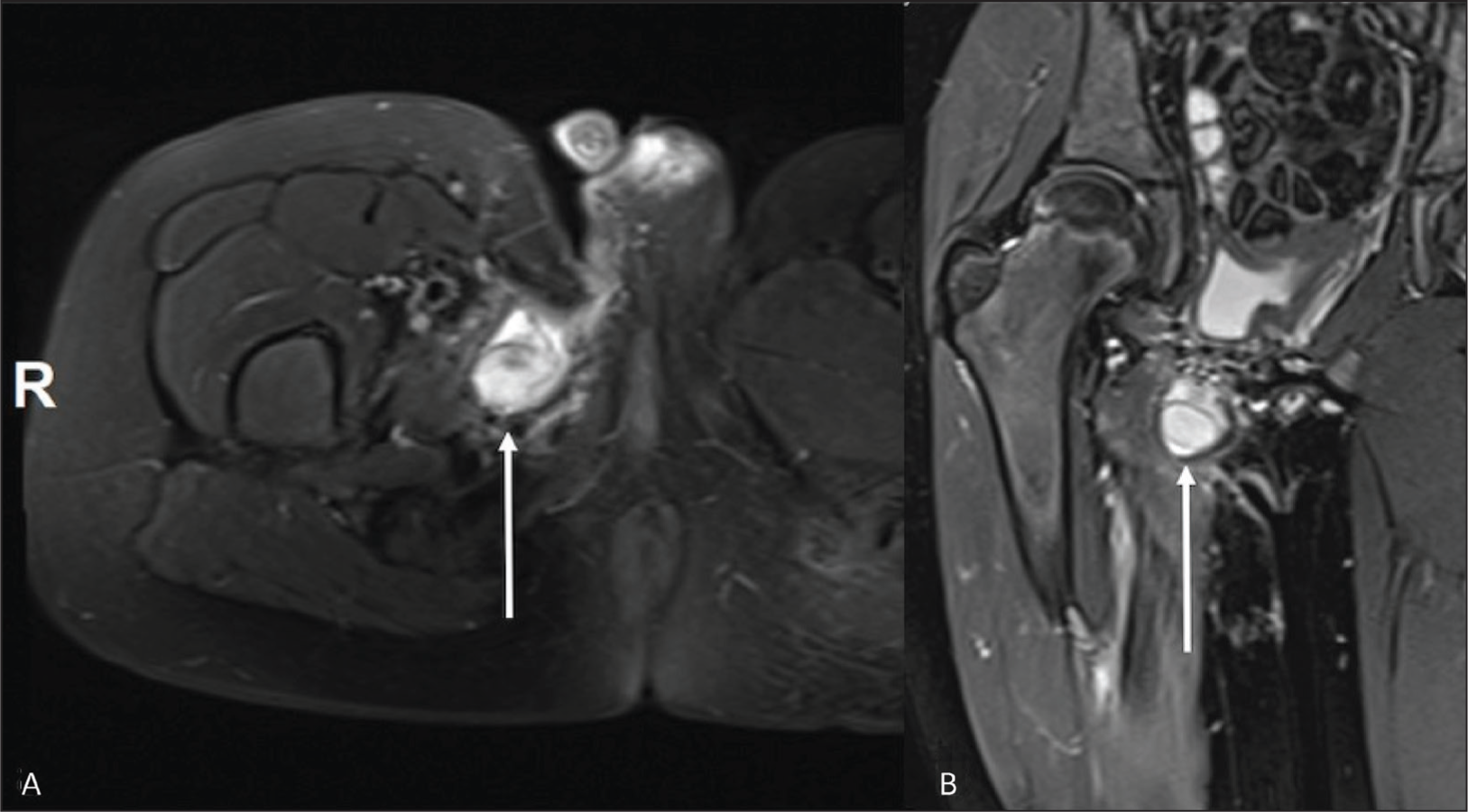
This lesion shared both T1 and T2 signal characteristics with the original resected primary tumour. The combination of location, imaging features, and absence on interval surveillance scans suggested a provisional diagnosis of local recurrence. On clinical examination, the mass was not palpable and there was satisfactory healing on inspection of the right groin flap.
Further characterisation of the lesion was warranted, and the region was interrogated with ultrasound. This revealed the solid mass-like lesion seen on MRI to be a malpositioned right testicle situated within the right adductor compartment. This mass was contiguous with the spermatic cord, which could be traced proximal to the inguinal canal. Careful examination of the scrotum revealed an absent testis and an empty right hemi-scrotum. The patient did not have a history of undescended nor retractile testes, and retrospective review of previous pre-operative MRIs confirmed the normal position of both testes within the scrotum. The patient subsequently underwent a successful right-sided orchidopexy and was followed up with MRI scans every three months for two years. These MRIs, performed since the orchidopexy did not show any significant signal abnormality or evidence of recurrence within the right adductor compartment.
Case 2
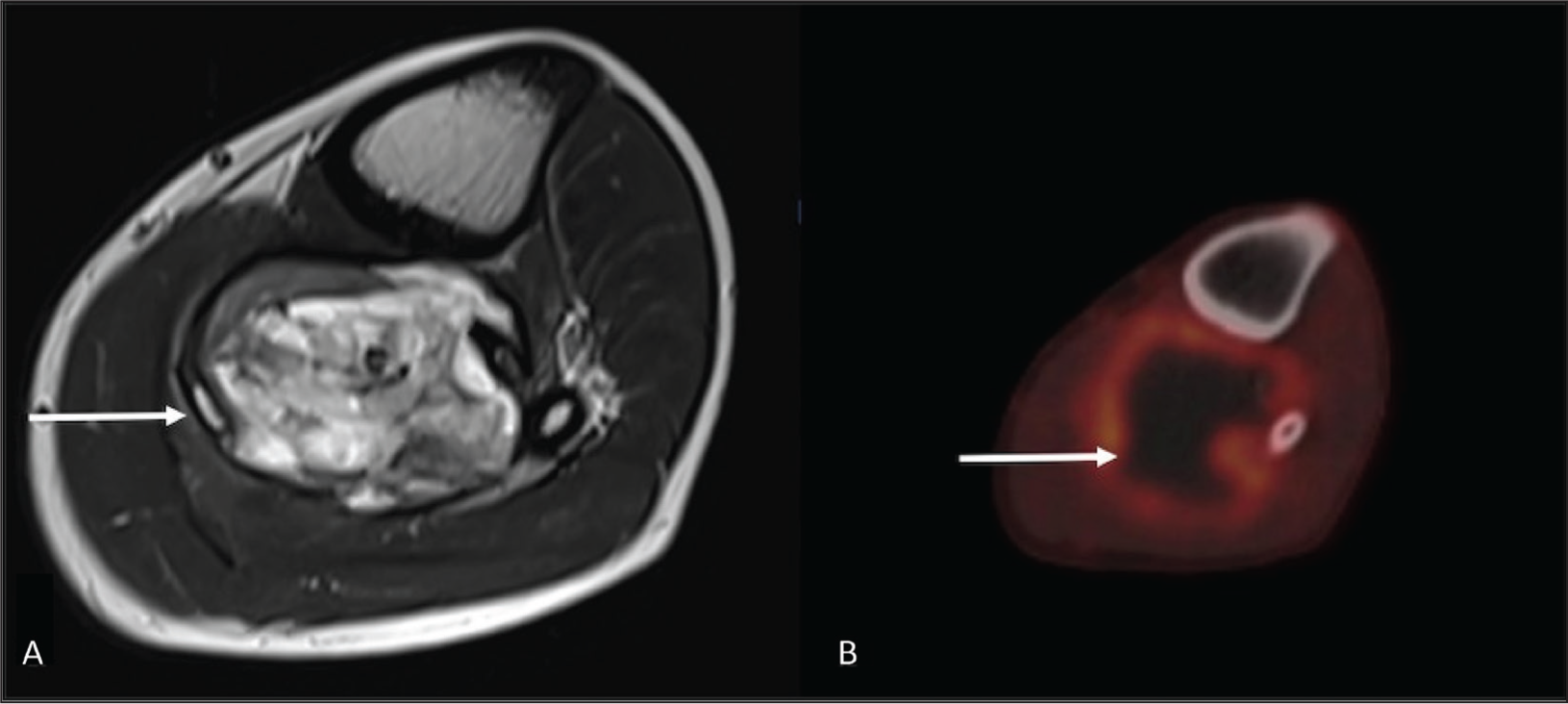
A 20-year-old male presented with a painful enlarging mass in the left calf. Initial MRI revealed a locally aggressive mass within the deep posterior compartment of the left proximal calf, encasing the neurovascular bundle [Figure 3A, B]. Biopsy of the mass revealed this to be synovial sarcoma. There was no evidence of distant metastatic disease on initial staging.
(A) Axial T2 MRI and (B) axial fused FDG-PET images demonstrating the locally aggressive synovial sarcoma in the deep posterior compartment of the left calf
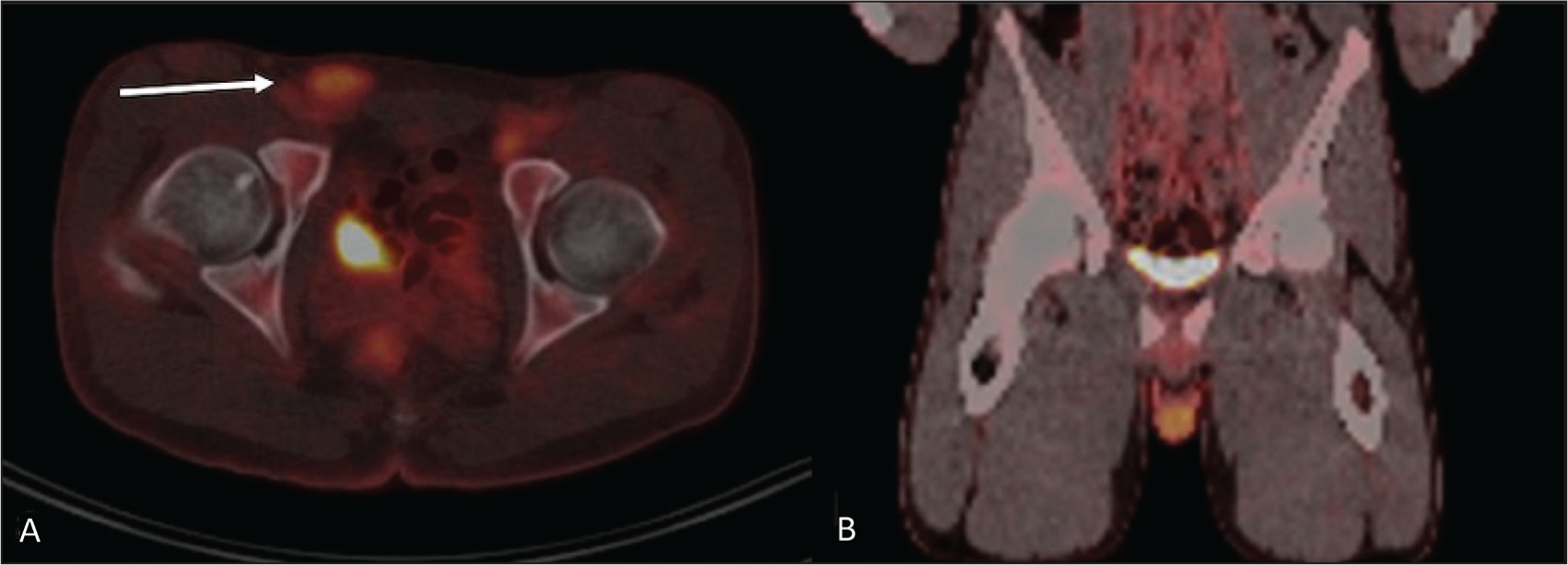
A routine PET scan was also undertaken as part of the completion of staging. A rounded FDG-avid structure was identified in the right inguinal region on the PET scan. The FDG uptake of this structure was also increased and similar to the primary synovial sarcoma, with the primary tumour having a 6.2 standard uptake value (SUV), and the right inguinal mass recording 4.1 SUV [Figure 4A, B]. This further raised suspicion for right inguinal nodal disease.
(A) Axial PET/CT showing a right undescended testis within the inguinal canal (white arrow), demonstrating physiological high FDG uptake; (B) the absence of the right testis within the ipsilateral scrotal sac on the coronal image
Upon revisiting the MRI and staging CT scans, this structure was revealed to be a normally developed but undescended right testis malpositioned within the inguinal canal. The patient did not provide a clear history of such symptoms, but this was confirmed through clinical examination as well as by the absence of a normal testis within the right hemi-scrotum on the available imaging. The patient was subsequently scheduled for a left above-knee amputation, as well as an orchidopexy.
Discussion
While undescended testes are a well-known entity, dislocation of the testes is rare.[6–8] Traumatic testicular dislocation usually occurs either due to direct or indirect force resulting in expulsion of the testis out of the scrotum after rupture of the external, internal and cremasteric fascia of the spermatic cord.[2] Three types of dislocation have been originally described in the literature, namely superficial, internal, or complex dislocation.[9,10] Superficial dislocation is the displacement of the testis within the radius of the spermatic cord and centred on the external inguinal ring. Internal dislocation involves the testes moving backward from the scrotum to the inguinal ring and the inguinal canal, intra-abdominally or into the femoral canal. Complex dislocation constitutes translocation of the testis from an open wound in the scrotum to the outside of the scrotum. In many of the cases (approximately 50%), the most common site for dislocation is the superficial inguinal pouch, and typically in the setting of trauma.[7,8]
The first patient is an unusual case of a dislocated testis occurring in the post-operative setting, where the dislocation occurred through the surgical defect created during the en-bloc oncological resection of the primary sarcoma. In this instance, the resection of the right-sided pubic ramus and the dissection of the spermatic cord performed for mobilisation prior to tumour resection resulted in communication between the scrotum and the adductor compartment. Post-surgical scarring and gradual retraction of the right testis through this defect into the adductor compartment was implicated to account for the interval testicular migration. In this instance, the finding on MRI mimicked local tumour recurrence.
Healthy testes show physiologic accumulation of FDG on PET/CT due to their high level of metabolic activity.[9,10] FDG-PET/CT has an important and complementary role in the diagnosis, staging, restaging, treatment response monitoring, and prognostication of soft tissue sarcomas.[10] As such, PET findings could add to confusion in a patient with an undescended testis or a testis in another unusual location.
Demonstrating continuity with the spermatic cord, as well as an absent testis within the ipsilateral scrotum on clinical examination would allow a confident diagnosis. Paying particular attention to the presence or absence of a testis within the scrotum when such an abnormality is identified on cross-sectional imaging would also aid in diagnosis. These patients may not routinely undergo a testicular examination unless symptoms develop, making the diagnosis challenging, thus making radiological interpretation of the abnormality crucial. Furthermore, continuity with the spermatic cord can be difficult to demonstrate on non-dedicated wide field of view MRI as well as on PET, particularly when there are surrounding post-operative changes and owing to poor contrast resolution of the latter. Therefore, when in doubt, ultrasound can be a helpful adjunct in further characterisation, as was shown to be the case in the first scenario.
Abnormal position of the testis outside the scrotum can lead to complications such as testicular torsion,[2] increased rate of orchidectomy and loss of spermatogenic function,[1] as well as higher risk of malignancy in the case of cryptorchidism.[4] Early identification of the entity would provide an opportunity for timely orchidopexy, thus avoiding these potential complications. Misinterpreting the displaced testis as a soft tissue mass may also result in unnecessary biopsy or inappropriate surgical intervention.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author Rajesh Botchu is a member of the Editorial Board of Apollo Medicine. The author did not take part in the peer review or decision-making process for this submission and has no further conflicts to declare.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Not applicable.
Informed consent
Written informed consent was obtained from the patients.
Credit author statement
All authors contributed significantly to the article.
SA - primary manuscript draft and preparation of figures, RDH - Drafting and review, AMD - supervision and final approval, proof reading, SLJ - supervision and final approval, proof reading, RB - supervision and final approval, assistance with figures.
Data availability
Not applicable.
Use of artificial intelligence
No.