
Abstract
Introduction:
Ewing sarcoma is a rare and highly aggressive malignancy, mostly involving the axial skeleton. Ewing sarcoma usually affects children and young adults under 20. Usually presenting as a painful swelling and discomfort worsening over time.
Case report:
We present a case of a 19-year-old female with no known co-morbidities presenting in the Emergency Department with complaints of fever and backache for the past 2 weeks and bilateral lower limb weakness for more than a week. She was started on steroids and broad-spectrum antibiotics and packed cell volume due to low hemoglobin. The screening MRI of the cervical and dorsal spine without contrast revealed signal abnormalities in the vertebral bodies at multiple levels (C2, C5, C6, C7, T1, and T3), as well as within the spinous processes and interspinous musculature. Further evaluation with contrast-enhanced MRI was recommended. The contrast-enhanced MRI showed straightening of the cervical and dorsal spine due to muscular spasm. Additionally, there were small soft tissue components in the left paravertebral region at the level of D3, extending into the epidural space, and epidural components encasing the thecal sac at the levels of D5, D9, and D10 suggestive of neoplastic lesions, most likely metastasis. The morphological and immunohistochemical correlation established the diagnosis of Ewing Sarcoma of the left thigh with nodal, para-spinal, and soft tissue metastatic lesions.
Conclusion:
Ewing Sarcoma is generally reported in the pediatric population and may come into clinical view based on a plethora of signs and symptoms. Appropriate imaging in the form of X-rays, CT scans, and MRI must be employed to correctly diagnose, and stage the condition.
Introduction
Ewing sarcoma is a rare and highly aggressive malignancy, characterized microscopically as small, round, blue cells that are sub-divided into osseous and extraosseous varieties. 1 The axial skeleton accounts for 54% of cases with osseous involvement, followed by the appendicular skeleton (42%), and other long bones. 2 Extraosseous ES, which often develops within the axial skeleton, is present in a smaller percentage and is more common in elderly people and women. 3 Ewing sarcoma is a rare entity that usually affects children and young adults under 20. 4 The primary signs and symptoms of Ewing sarcoma include swelling, pain, and discomfort that worsens with time in the affected area. Other non-specific symptoms include fever, extreme exhaustion, and weight loss. 5 Rapidly progressive paraplegia is subject to a high threshold of suspicion since it is an unusual finding in young patients and warrants timely diagnosis and treatment. 6
Case Presentation
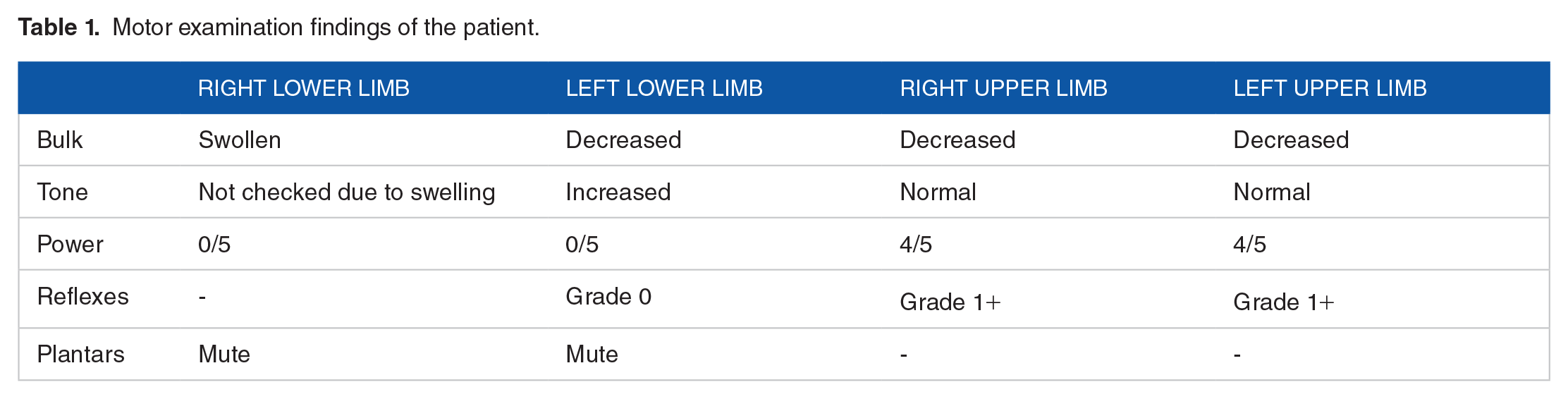
A 19-year-old female, resident of Nawabshah, student of 12th Grade, with no known co-morbidities, was admitted via ER with complaints of fever and backache for 15 days and bilateral lower limb weakness for 8 days. On inquiring about the detailed history, it was revealed that she developed an intermittent fever of 102F associated with rigors and lower back pain that radiated bilaterally to the lower limbs. The pain was moderate to severe, aching, and relieved by oral analgesics. Lower limb weakness occurred concurrently with fecal incontinence and urinary retention, with numbness of lower limbs. Her systemic review was unremarkable, with only undocumented weight loss and reduced appetite. Contact history for Tuberculosis is positive from her grandfather, who has been suffering from it for 5 months. Examination of the lower limb was performed, where the right limb was found to be shiny, tender, and warm, with swelling reaching up to the shin. Other findings have been summarized in Table 1. Cerebellar signs could not be assessed in the lower limbs, while spinal examination revealed a bilaterally sensory level at T10. MRI of the lumbar spine on admission also yielded no meaningful information. Differentials based on this history were Pott’s Disease, Transverse Myelitis, Spinal Abscess and Spinal Tumors.
Motor examination findings of the patient.
The patient was admitted with the aforementioned complaints under the observation of the neurosurgery and medicine wards.
MRI Cervical Spine and Thoracic spine screening was done that showed areas of signal abnormality within the vertebral bodies at multiple levels with signal on STIR imaging involving C2, C5, C6, C7, T1, and T3. Areas of high signal noted within the spinous process at multiple levels with slight high signal within interspinous musculature. Full study with IV contrast was advised for further evaluation.
Contrast-enhanced MRI of dorsal spine demonstrates multilevel enhancing abnormal bone marrow signals in the vertebral body, including posterior elements. Gadolinium-staining of the vertebral bodies seen by the signal disparity within the vertebral bodies in the sagittal section indicates infiltration of neoplastic tissue. A high-signal component, most likely the metastatic component of the cancer tissue is also notably visible at the Level of D9-D10 vertebra. It is better appreciated in the axial views, where at the level of D3 vertebra, a small soft tissue enhancing mass is seen in left paravertebral region, extending into the epidural space through left neural foramen. Large epidural component was also recognized posteriorly and to the left side at D9 and D10 vertebrae levels, causing significant pressure and anterior displacement of the thecal sac and spinal cord. This could be appreciated in the sagittal view as the loss of normal anatomy of the anterior longitudinal ligaments. These findings related to neoplastic lesions with metastasis. Figure 1 shows the findings of the MRI after Gadolinium staining.

Patient’s MRI of the dorsal spine with contrast (T1 axial and contrast enhancing T1 axial and sagittal images).
The Neurosurgery department planned for spine decompression with or without fixation and excision of the spinal space-occupying lesion. Concurrently, a venous Doppler Ultrasound done for the right leg swelling showed Deep Vein Thrombosis in the Common Femoral, Popliteal, and Right External Iliac veins, which extend into the saphenofemoral junction. The patient was subsequently also given Enoxaparin subcutaneously. Intravenous Vancomycin and Amikacin were added to Meropenem due to the epidural collection found.
Due to the high-risk nature of the surgery, neurosurgery further recommended engaging the radiology department and obtaining a biopsy to establish a diagnosis. A CT scan of the dorsolumbar spine was also scheduled, which showed the possibility of osteomyelitis with paravertebral and epidural mass, likely denoting Tuberculosis. A thrombus was also seen in the right external iliac vein, extending into the right common femoral vein.
Consistent with the findings, the medicine department initiated Antitubercular Therapy (ATT). Ultrasound-guided biopsy of the left paraspinal mass was carried out—which showed benign reactive lymph nodes—and a gastroenterology opinion was sought for low hemoglobin levels, for which they proposed an esophagogastroduodenoscopy (EGD) along with colonoscopy once the patient is stabilized. The patient had developed persistent tachycardia, and echocardiography (ECG) demonstrated sinus tachycardia for which Ivabradine was added to the treatment regimen.
A laminectomy at D8-D9-D10 levels, tumor excision, and duroplasty was performed on the 15th day of admission. A sample for biopsy was sent, and per-operative findings illustrated that the mass was most likely neoplastic and not tubercular, thus halting ATT. The patient then developed shortness of breath, cough, and oxygen saturation dropped to 89% on room air. Chest X-Ray showed a left-sided non-homogenous opacity, confirmed as pleural effusion on ultrasound chest. Intravenous Colomycin was added to the treatment armamentarium.
The bone marrow aspirate shows a diluted tap with an aparticulate specimen. It contained 2 to 3 small clusters of mononuclear cells, medium in size, scattered throughout the smears. Granulocytic precursors, lymphoid cells, and denuded cells are also observed. Trilineage hematopoiesis is notably suppressed. The touch preparation revealed hypocellular imprints mainly composed of medium-sized mononuclear cells with round to oval nuclei and moderately basophilic cytoplasm, along with degenerating cells, indicating suppressed normal hematopoiesis. The trephine biopsy displays areas of moderate to marked fibrosis with distorted hematopoietic and non-hematopoietic cells. Small areas of intact mononuclear cells, both hematopoietic and non-hematopoietic, were present, as well as areas of normal hematopoiesis. Large areas of necrotic tissue were also noted.
The high suspicion for malignancy warranted a CT of the chest, abdomen and pelvis for primary site evaluation and staging, which depicted neoplastic lesions involving the proximal thigh with nodal, para-spinal, and soft tissue metastatic deposits.
An immunohistochemical examination was performed by DAKO envision method and was positive for CD99 and FLI-1 antibodies. The morphological and immunohistochemical correlation established the diagnosis of Ewing Sarcoma.
The oncology department was also taken on board for further evaluation. The patient was now stable, but the family refused further MRIs, and the patient got a Leave Against Medical Advice (LAMA). Bone Marrow biopsy was followed, and confirmed the diagnosis of Ewing Sarcoma, while raising a strong suspicion of metastasis. The final diagnosis was documented as Ewing Sarcoma of left thigh with nodal, para-spinal, and soft tissue metastatic lesion.
Discussion
Ewing Sarcoma is entitled to the Primitive Neuroectodermal Tumor (PNET) family of tumors, showing histological similarity with other central tumors of the family, including pinealoblastoma, supratentorial PNET, and medulloblastoma. The pathological and molecular presentation is analogous to Primary Ewing Sarcoma, extraosseous Ewing Sarcoma, peripheral PNET, Askin tumors, lymphoma, malignant meningioma, and atypical rhabdoid tumor.7,8 Given the similitude of Ewing Sarcoma with other classes of tumors, clinical presentation and immunohistochemical staining remain the mainstay of diagnosing the condition. FLI-1 and CD99 are the commonly implicated markers, with FLI-1 showing higher specification for Ewing Sarcoma whilst also being found in other soft-tissue tumors.
A multitude of patients with Ewing Sarcoma undergo a reciprocal translocation of the EWS and FLI-1 genes which gives rise to a fusion transcript, represented as t(11,22)(q24,q12). 9 The absence of this mutation does not, however, rule out Ewing Sarcoma as other translocations such as t(21;22)(q22;12), EWSR1 gene on chromosome 22, ETV1 gene on chromosome 7, FEV gene on chromosome 2, and ETV4 gene on chromosome 17 have also been implicated in literature.10 -12 Elucidation of genetic mutations by molecular analysis is complementary to immunohistochemical analysis when it is highly suggestive of Ewing Sarcoma. CD99 expression and FLI-1 antibodies are highly suggestive of Ewing Sarcoma. 13 CD99 or FLI-1 antibodies are also individually sensitive to the presence of Ewing Sarcoma; however, they are not specific to the diagnosis. CD99 expression is also frequently found in rhabdomyosarcomas, hematopoietic malignancies, synovial sarcomas, neuroendocrine tumors, and solitary fibrous tumors. FLI-1 antibodies are also found in vascular and lymphoblastic malignancies.14,15 A whole-body workup is required to exclude a primary malignancy, followed by a PET scan or spinal MRI for staging purposes. 16 MRI is the investigation of choice for assessing spinal lesions. 13
Ewing sarcoma is normally a childhood malignancy usually confined to the skeleton and arising in the long bones and pelvic region, with only 3.4% to 7% of cases reported to involve the spine. 17 Radiographically, spinal lesions exhibit osteolytic or osteosclerotic development in the vertebral body. 18 In a systematic review of case reports conducted by Lu et al, the lumbar and sacral regions of the spine were most commonly involved (61%), followed by the cervical (20%) and thoracic (18%) regions. The predominant complaints of the patients were pain (59%) and weakness (41%), which are in lieu of the case we have reported above. 19 A review of literature by Eren Mungen found only 17 cases of Ewing Sarcoma, in children less than 18 years of age. The predominant complaints reported by these individuals are as follows: solely back pain by 7, solely leg pain by 2, back pain along with extremity pain by 3, and motor weakness by 5. Physical examination was unremarkable in 4 cases, while among the 14 cases, limb weakness was reported in 7, loss of sensations in the limbs in 8, and altered reflexes in 1 case. 20 The clinical appearance of the patient we have reported amalgamates several of these findings.
Given the coincidental symptomatology of the disease, several indefinite diagnoses could be envisioned. These include osteomyelitis, osteosarcoma, metastatic disease, lymphoma, and neuroblastoma. Tuberculosis manifesting as Pott’s disease is also a differential that must be credited in Tuberculosis-endemic regions, as in this case. As discussed previously, immunohistochemical analysis is crucial to definite diagnosis; biopsy remains the gold-standard test for diagnosis. 21 This is again in congruence with how the abovementioned case was investigated.
Treatment for Ewing Sarcoma may be based on the North American or European approaches, both of which generally initiate chemotherapy, succeeded by confined treatment comprising of surgery or radiation and another round of chemotherapy.
In North America, the chemotherapeutic paradigm is repeated every 2 weeks and consists of Vincristine, Adriamycin, Cyclophosphamide, and either Ifosfamide or Etoposide (VDC/IE). 22 Patients with metastatic disease follow a modified regimen, VACA (Vincristine, Actinomycin, Cyclophosphamide, and Adriamycin). The efficacy of this armamentarium is not yet conclusive. Surgery for the primary tumor is protracted till the first cycle of chemotherapy is administered. Cohesive surgical resection, inclusive of the tumor and biopsied lesion, along with safe margins, must be performed to suspend adjuvant chemotherapy. 23 The choice between surgical resection and radiotherapy is tailored to each patient and is contingent on tumor location, feasibility of resection, and predicted morbidity. Literature suggests a leverage to surgical resection when compared with radiotherapy. 24
In Europe, a slightly distinctive chemotherapy regimen, VIDE (Vincristine, Ifosfamide, Doxorubicin, and Etoposide), is employed. A maximum tolerated dose with the briefest possible time duration is induced. Stem-cell therapy is being extensively studied to succeed in chemotherapy. The role of surgery and adjuvant radiotherapy is based on the same principles as in North America.
Conclusion
Our case presented a typical young adult female with signs of weakness, pain, and other constitutional symptoms, and was diagnosed with Ewing Sarcoma as per her biopsy findings. Ewing Sarcoma is generally reported in the pediatric population and may come into clinical view based on a plethora of signs and symptoms. Appropriate imaging in the form of X-rays, CT scans, and MRI must be employed to correctly diagnose, and stage the condition. The foundation of treatment is based on an initial trial of chemotherapy, followed by surgical resection and/or radiotherapy, tailored to the unique case of each patient, depending on the response to chemotherapy and tumor burden. Another cycle of chemotherapy is again explicit in each case. Our patient unfortunately left against medical advice and was thus lost to follow-up without being provided any treatment. The patient also had positive Tuberculosis contact, which could be misleading for clinicians, making this case a crucial example, especially in regions where Tuberculosis is rampant.
Footnotes
Acknowledgements
The authors are very appreciative to the patient for the opportunity to learn as well as thankful to the hospital for providing support for completing this report.
Author Contributions
RW and MS: Substantial contributions to the conception or design of the work. Drafting the work or revising it critically for important intellectual content.
SG, EK, MSH, and HHS: Drafting the work or revising it critically for important intellectual content. Final approval of the version to be published.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Patient Consent
Written Informed Consent was obtained from the patient for the publication of this case report.
Provenance and Peer Review
Not commissioned, externally peer reviewed.