
Abstract
Objectives:
Low rectal cancer presents dual challenges—achieving oncologic radicality while preserving sphincter function. Neoadjuvant chemoradiation (NACRT) has become the cornerstone of treatment, yet it induces significant histological changes that complicate intraoperative assessment of resection margins. This review aims to critically evaluate the management of positive doughnut margins in the context of NACRT.
Methodology:
A comprehensive literature search was conducted using PubMed, Scopus, and Web of Science databases to identify peer-reviewed articles from January 2015 to May 2025. The keywords included “positive doughnut margin,” “low rectal cancer,” “neoadjuvant chemoradiation,” and “intraoperative frozen section.” Emphasis was placed on surgical decision-making, histopathologic interpretation, and oncologic outcomes.
Results:
Doughnut specimens obtained during stapled anastomoses represent critical proximal and distal margins. Post-NACRT histological distortion may yield ambiguous frozen section results. While a positive doughnut margin may raise concerns of residual disease and local recurrence, its prognostic significance remains debatable. Current strategies range from re-resection and extended dissection to watchful waiting in select cases. Emerging modalities—such as high-resolution MRI, diffusion-weighted imaging, and molecular profiling—show promise in refining intraoperative decision-making.
Conclusion:
Positive doughnut margins should not be viewed in isolation but interpreted alongside tumor regression grade, main specimen margins, and patient fitness. A multidisciplinary approach, integrating imaging and pathological cues, is vital. This review provides a practical and evidence-based framework for surgeons managing these complex scenarios while identifying future research directions.
Keywords
Introduction and Clinical Background
The management of low rectal carcinomas demands a careful equilibrium between ensuring complete tumour removal and preserving critical functions, particularly sphincter control. Neoadjuvant chemoradiation is now widely used to reduce tumour size and facilitate surgical resection, while also improving the chances for sphincter preservation.[1,2] Despite these benefits, accurately assessing the response to therapy remains a challenge.
Modern imaging modalities such as positron emission tomography (PET) and magnetic resonance imaging (MRI) play an important role in evaluating tumour response to neoadjuvant therapy. However, these methods sometimes fail to detect residual microscopic disease. In the context of a circular stapled anastomosis, the excised ‘doughnut’ specimen—comprising the circumferential margin of the resected bowel—is routinely examined by frozen section analysis. It is critical to distinguish between the doughnut margin, which specifically refers to the circular stapled proximal and distal bowel margins examined intraoperatively, and the circumferential resection margin (CRM), representing the radial margin around the rectal tumour within the mesorectal fascia. This differentiation avoids clinical and pathological ambiguity. A positive result on this specimen indicates the presence of tumour cells at the resection margin, which could signify a higher likelihood of local recurrence. Consequently, the intraoperative findings can trigger an urgent need to either extend the resection or consider alternative management options.[3,4]
Understanding the histopathological effects of neoadjuvant chemoradiation and the limitations inherent to frozen section analysis is essential for tailoring the best surgical strategy. This review provides an integrated discussion on these topics, outlines current management approaches for positive doughnut margins, and offers insights into emerging diagnostic and therapeutic advancements.
Impact of Neoadjuvant Chemoradiation on Tumour and Margin Assessment
Histopathological Changes Following Therapy
Neoadjuvant chemoradiation induces a range of histopathologic changes in rectal cancer tissues. Typically, these changes include tumour regression, the development of fibrosis, and associated inflammatory responses. The introduction of total neoadjuvant therapy (TNT)—involving the administration of systemic chemotherapy followed by chemoradiation before surgery—has further intensified histopathological alterations in rectal cancer specimens. TNT tends to cause profound tumour regression and stromal changes, which may exacerbate diagnostic ambiguity during margin assessment. Importantly, TNT has also shifted the timeline of tumour response evaluation, requiring careful integration of radiologic, pathologic, and intraoperative findings to interpret doughnut margin status accurately. Notably, the fibrosis resulting from treatment can blur the boundaries between viable tumour cells and normal tissue, complicating both macroscopic and microscopic assessments.[1,2]
In many cases, the tumour may be largely replaced by fibrotic tissue, with only scattered clusters of residual malignant cells remaining. This can pose a diagnostic dilemma during intraoperative frozen section analysis. For instance, the presence of extensive fibrosis might lead to under-sampling of small clusters of tumour cells (resulting in false negatives), whereas inflammatory or reparative tissue changes might be misinterpreted as residual malignancy (resulting in false positives).
Discordance Between Imaging and Pathology
Despite advances in imaging, discrepancies between radiological findings and histopathological results are not uncommon. MRI is particularly adept at identifying changes in tissue architecture; however, its sensitivity may be limited when it comes to detecting microscopic residual disease.[3,5] Similarly, while PET imaging provides functional insights by measuring metabolic activity, it can underestimate tumour burden in post-radiation settings where metabolic activity is altered.
This disconnect between imaging and actual histopathologic findings reinforces the need for intraoperative frozen section analysis of the doughnut margin. Nonetheless, the accuracy of such analyses is inherently challenged by the same post-therapy tissue changes that affect imaging, thereby necessitating a more nuanced interpretation of intraoperative findings.
Intraoperative Frozen Section Analysis and Doughnut Margin Evaluation
Rationale and Methodology
In the context of circular stapled anastomosis, the doughnut specimen encapsulates the entire circumferential margin of the distal bowel. Intraoperative frozen section analysis is performed on this specimen to promptly detect the presence of microscopic tumour cells. The rapid turnaround offered by frozen section evaluation provides essential feedback, enabling the surgical team to make timely decisions about whether to proceed with additional resection.[5,6]
The procedure involves freezing the doughnut tissue, sectioning it into thin slices, and applying special stains to allow for immediate histopathological review. While the process is designed to be efficient, its reliability is often compromised by the tissue alterations induced by neoadjuvant therapy.
Challenges Associated with Irradiated Tissue
One of the major challenges of intraoperative frozen section analysis is the altered state of irradiated tissue. Post-radiation changes such as fibrosis, oedema, and cautery artefacts can mimic the appearance of residual tumour cells, thereby increasing the risk of false-positive interpretations. Conversely, these same changes might obscure viable tumour cells, resulting in false negatives. Furthermore, the heterogeneous nature of post-irradiation tissue raises the issue of sampling error, as the section examined may not be representative of the entire margin.[4,6]
Prognostic Implications of Positive Doughnut Margins
The clinical relevance of a positive doughnut margin remains a topic of debate. Some retrospective studies have shown that when the primary resection margins are negative, an isolated positive doughnut margin does not necessarily portend a higher risk of local recurrence.[3,4] Conversely, other studies have linked any residual tumour at the margin with a more aggressive disease phenotype, arguing in favour of a more radical surgical approach.[7] This divergence in findings underlines the importance of considering the broader clinical context when interpreting frozen section results.
Detailed Management Strategies for Positive Doughnut Margins
Intraoperative Decision-making
Recognition and Verification
The first step in managing a positive doughnut margin is to verify the intraoperative findings. Given the interpretative challenges posed by irradiated tissues, many institutions advocate for repeating the frozen section or obtaining a second pathological opinion when uncertainty exists.[5,6] This confirmation is vital, as it directly influences the subsequent surgical strategy.
Surgeon–Pathologist Collaboration
Robust communication between the surgeon and the pathologist is essential during the procedure. Real-time discussions about tissue quality, potential artefacts, and the adequacy of sampling can provide valuable insights. In some cases, an impromptu multidisciplinary consultation, such as an intraoperative tumour board review, may be warranted to guide the decision-making process.
Immediate Re-resection Versus a Conservative Approach
Once a positive doughnut margin is confirmed, the surgical team must quickly determine whether to proceed with additional resection or to manage the case more conservatively.
For patients with favourable anatomy, extending the resection to obtain clear margins is typically the recommended approach. This may involve resecting an additional segment of the distal colon and, when necessary, converting from a circular stapled anastomosis to a hand-sewn technique to ensure optimal tissue approximation.[3,7]
In scenarios where further resection is deemed too risky—such as in patients with compromised sphincter function or significant comorbid conditions—a more conservative approach may be adopted. This strategy often includes additional intraoperative sampling to better define the extent of margin positivity, followed by intensified adjuvant therapy postoperatively. Such decisions are usually made when the primary resection margins are negative, thereby mitigating the overall risk of local recurrence.[7]
Postoperative Management and Adjuvant Therapies
Adjuvant Therapy
When additional resection is not feasible or when re-resection yields ambiguous margins, postoperative management becomes paramount. Intensified adjuvant chemotherapy is frequently recommended to target any residual microscopic disease. While re-irradiation is generally constrained by tissue tolerance limits, salvage radiotherapy may be considered in selected cases, particularly when the risk of local recurrence remains high.[5,8]
Surveillance and Follow-up
Patients who do not undergo further resection must be managed with a rigorous postoperative follow-up regimen. This typically includes the following:
Salvage Procedures
In cases where local recurrence is detected during follow-up, salvage procedures, such as an abdominoperineal resection or local excision—may be warranted. Recent advancements, including fluorescence-guided surgery and confocal laser endomicroscopy, are being explored to improve intraoperative margin assessment and potentially reduce the incidence of positive doughnut margins in future procedures.[7]
Minimally invasive transanal approaches such as transanal minimally invasive surgery (TAMIS) and transanal endoscopic microsurgery (TEMS) have emerged as effective salvage options for select patients with localised recurrence or isolated positive margins. These techniques enable precise excision while preserving pelvic function, and may be particularly valuable when reoperative pelvic surgery poses elevated morbidity risks. TAMIS/TEMS are best considered in multidisciplinary discussions, especially when imaging confirms isolated mucosal or submucosal involvement without deep or nodal disease.
Factors Influencing Management Decisions
Multiple factors inform the decision between pursuing additional resection versus adopting a conservative approach:
A positive doughnut margin may serve as a marker for aggressive tumour behaviour, especially when accompanied by high-risk features such as poor differentiation or lymphovascular invasion.[5] In such cases, an aggressive surgical approach is generally favoured.
A poor radiological response to neoadjuvant therapy, coupled with a positive intraoperative margin, typically leans toward further resection. Conversely, if imaging indicates a robust response and the primary margins are negative, conservative management may be considered.[3]
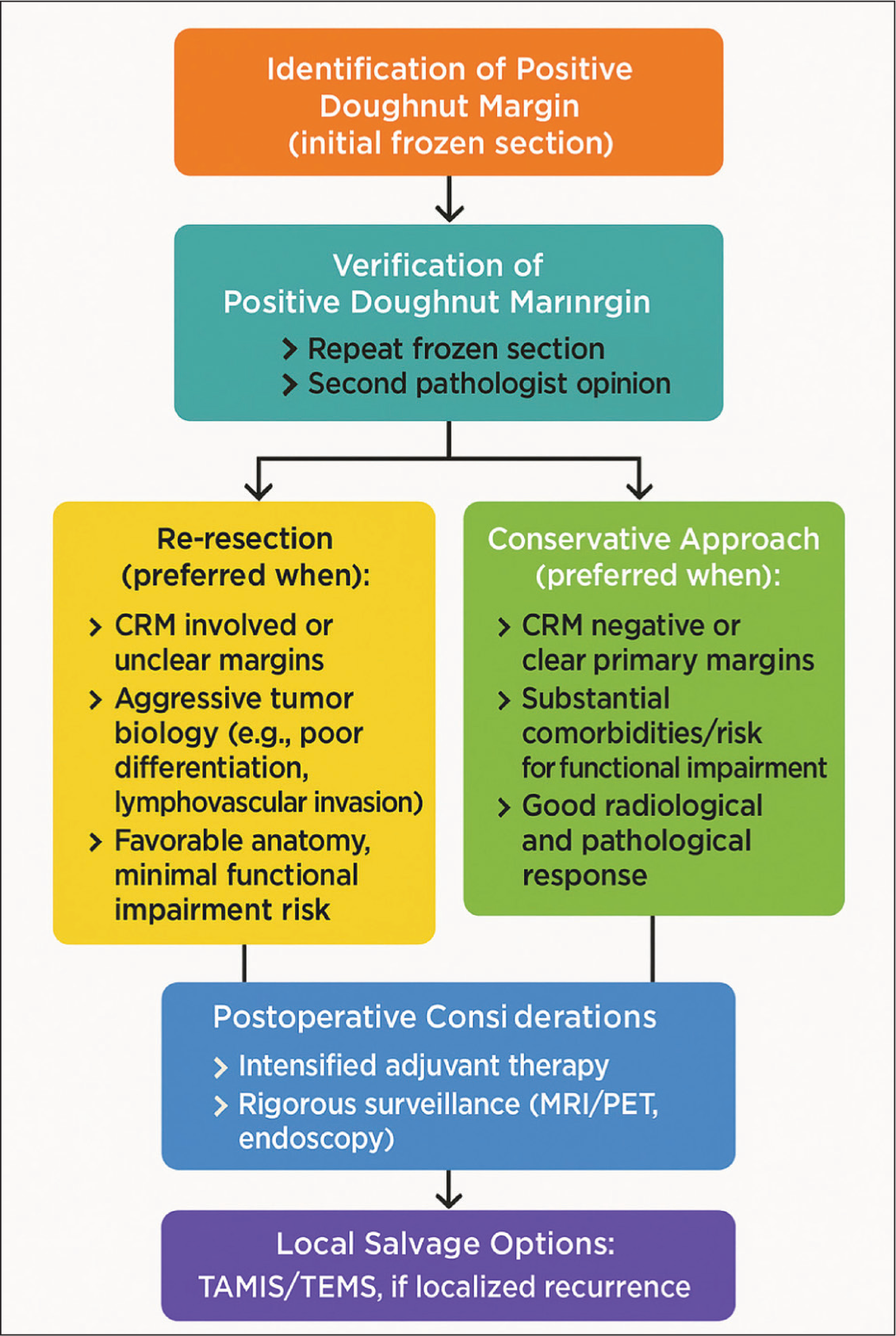
The patient’s overall health status, comorbidities, and the potential impact on quality of life—especially with respect to sphincter function—play crucial roles in guiding the management strategy. For patients at higher risk for functional impairment, a conservative approach supplemented with adjuvant therapy may be preferable.[4] A practical approach to surgical decision-making in cases of positive doughnut margins—incorporating margin status, response to neoadjuvant therapy, and patient-specific factors—is illustrated in Figure 1.
Controversies and Future Directions
Debated Issues in Current Literature
A central point of debate in the literature concerns the significance of an isolated positive doughnut margin when the primary resection margins are clear. The majority of evidence currently informing management strategies for positive doughnut margins is derived from retrospective studies, representing level 3–4 evidence. The absence of robust prospective, randomised controlled trials constitutes a significant research gap. Additionally, the lack of universally standardised criteria for doughnut margin interpretation following neoadjuvant chemoradiation further complicates clinical decision-making and underscores the critical need for structured prospective studies. Several studies have suggested that an isolated positive finding does not independently correlate with increased local recurrence or worse survival outcomes.[3,4] These observations imply that the overall status of the primary resection margins might be a more critical determinant of oncologic outcomes than the doughnut margin alone.
In contrast, other investigators contend that any evidence of tumour cells at the margin is indicative of a biologically aggressive disease and warrants a more assertive treatment strategy.[7] The lack of uniformity in these findings underscores the need for standardised diagnostic criteria for interpreting frozen sections in the post-neoadjuvant setting.
Future Directions in Management
Advanced Intraoperative Imaging
Technological advances, such as fluorescence-guided surgery and confocal laser endomicroscopy, are showing promise in improving the real-time assessment of surgical margins. These tools could potentially enhance the detection of microscopic residual disease, thereby reducing the reliance on traditional frozen section analysis and minimising sampling errors.[7]
Molecular and Genetic Predictors
There is growing interest in identifying molecular markers that can predict the response to neoadjuvant therapy and the likelihood of residual disease. Biomarkers that correlate with aggressive tumour biology may help stratify patients according to risk, thereby guiding decisions regarding the need for additional resection versus conservative management.[5]
Standardisation of Reporting
Developing uniform reporting systems for doughnut margin status in the context of neoadjuvant therapy is a critical next step. Standardised protocols would not only improve the reproducibility of intraoperative assessments but also facilitate meaningful comparisons across studies. Ultimately, such standardisation may lead to evidence-based guidelines that improve clinical decision-making and patient outcomes.[4]
Summary and Clinical Implications
Neoadjuvant chemoradiation is indispensable in the management of low rectal cancer, yet it introduces significant challenges in the histopathologic evaluation of surgical margins. Although intraoperative frozen section analysis of the doughnut specimen remains an essential tool, its utility is hampered by radiation-induced tissue changes that can obscure or mimic residual tumour cells. The decision to pursue further resection versus adopting a conservative management strategy is multifactorial, hinging on the reliability of intraoperative findings, tumour biology, radiologic response, and individual patient considerations.
Current evidence suggests that an isolated positive doughnut margin, in the presence of clear primary resection margins, may not necessarily lead to poorer outcomes. However, it should trigger a careful reassessment, and, where feasible, additional resection should be considered. In cases where further surgery poses significant risks, intensifying adjuvant therapy and implementing a rigorous follow-up protocol can help mitigate the risk of local recurrence. A multidisciplinary approach, integrating the expertise of surgeons, pathologists, radiologists, and oncologists, is critical to balancing the immediate risks of aggressive resection with the long-term benefits of oncologic control.
As the field advances, emerging imaging modalities and molecular diagnostics are likely to refine our understanding of residual disease and improve intraoperative decision-making. Such innovations will contribute to more personalised surgical strategies, ultimately enhancing both oncologic outcomes and quality of life for patients with low rectal cancer.
Concluding Remarks
The management of a positive doughnut margin following neoadjuvant chemoradiation in low rectal cancer remains a multifaceted challenge. While many centres advocate for aggressive re-resection to secure negative margins, a subset of patients may derive benefit from a conservative approach, particularly when further surgery risks significant functional impairment. The integration of adjuvant therapy and strict postoperative surveillance plays a crucial role in such cases. Continued research into advanced intraoperative imaging, molecular predictors, and standardised reporting will be essential in optimising treatment protocols and improving patient outcomes.
This review has outlined the current evidence and controversies surrounding positive doughnut margins, providing a comprehensive framework for surgical decision-making. By balancing immediate surgical risks with long-term oncologic benefits, clinicians can tailor their approach to each patient’s unique circumstances. As our understanding of post-neoadjuvant tissue changes deepens, more precise and individualised management strategies are likely to emerge, ultimately contributing to better clinical outcomes in low rectal cancer.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Not applicable. This is a literature review and does not involve human participants or clinical data.
Credit author statement
Supreet Kumar: Conceptualization, drafting of the manuscript, literature synthesis, final approval.
Aishwarya Bhalerao: Literature review, critical revision, formatting and referencing.
Vivek Tandon: Supervision, technical input, manuscript review.
Deepak Govil: Senior mentorship, final editing, overall direction and approval.
All authors reviewed and approved the final manuscript and agree to be accountable for all aspects of the work.
Informed Consent
Not applicable. This is a narrative literature review that does not involve direct patient data.
Data Availability
Not applicable. No new data were generated or analyzed in this study.
Use of artificial intelligence
Not used in this study.