
Abstract
Background:
Effective management of postoperative pain and postoperative nausea and vomiting (PONV) is crucial for patient recovery following laparoscopic hysterectomy. This study aims to compare the efficacy of paracetamol alone versus a combination of paracetamol-dexmedetomidine in reducing postoperative pain and PONV.
Patients and Methods:
This prospective, randomised, controlled study involved 104 patients scheduled for elective laparoscopic hysterectomy under general anaesthesia, randomly assigned into two groups. Group P received paracetamol (PCM) 4.5 mg/kg as a bolus dose over 15 minutes prior to extubation, followed by continuous infusion (0.5 mg/kg/hr) and demand doses (1 mg/kg) via patient-controlled analgesia (PCA) pump with a 30-minute lockout interval. Group PD received PCM 4.5 mg/kg and dexmedetomidine 1 µg/kg as a bolus dose over 15 minutes prior to extubation, followed by continuous infusion (PCM 0.5 mg/kg/hr and dexmedetomidine 0.05 µg/kg/hr) and demand doses via PCA pump with a 30-minute lockout interval. The primary outcome was the visual analogue score (VAS) at 1, 2, 4, 6, 12 and 24th hours and analgesic requirement in the first 24 hours postoperative period. The secondary outcome was the incidence of PONV experienced by the patients within first 24 hours postoperative period.
Results:
In the first 24 hours postoperatively, the VAS score and analgesic requirement were significantly less in Group PD. The incidence of PONV was also significantly reduced in Group PD.
Conclusion:
The combination of paracetamol-dexmedetomidine provided superior pain relief and reduced the incidence of PONV compared to paracetamol alone in patients undergoing laparoscopic hysterectomy (CTRI/2022/08/045086).
Keywords
Introduction
Laparoscopic hysterectomy, a minimally invasive procedure for uterus removal, offers benefits such as reduced postoperative pain, blood loss, and shorter hospital stays compared to open abdominal hysterectomy.[1] However, peritoneal insufflation exceeding 10 mmHg can trigger significant catecholamine release and diaphragmatic irritation, leading to notable postoperative pain.[2] This pain, often comparable to or more severe than that following open surgery, necessitates effective pain management strategies.
Pain management is crucial in Enhanced Recovery After Surgery (ERAS), and effective pain management involves using multimodal analgesics.[3,4] Opioids in patient-con-trolled analgesia (PCA) pumps have been used to alleviate postoperative pain, but they can cause adverse events such as increased postoperative nausea and vomiting (PONV), dizziness, constipation, and urinary retention.[5,6] Various strategies like regional nerve blocks, local analgesics, oral acetaminophen, selective and nonselective nonsteroidal anti-inflammatory drugs, pregabalin, and dexmedetomidine have been used to reduce opioid usage.[7–9] Various authors used paracetamol and dexmedetomidine individually during the perioperative period and showed improved visual analogue score (VAS) and reduced PONV through an opioid-sparing effect in different surgeries.[10,11]
Patient-controlled intravenous analgesia (PCIA) is a popular and effective postoperative analgesia method due to its rapid action, stable blood concentrations, and timely control of burst pain by bolus dose. Given this context, the purpose of this study was to compare the effects of paracetamol and paracetamol-dexmedetomidine combination in PCIA during laparoscopic hysterectomy to assess the VAS score, the need for analgesics, and PONV.
Methods
This experimental study was conducted from 15 June 2022 to 15 December 2023 (
Group P (n = 52) received paracetamol 4.5 mg/kg as a bolus dose over 15 minutes prior to extubation, followed by continuous infusion (0.5 mg/kg/hr) and demand doses (1 mg/kg) via PCA pump with a 30-minute lockout interval.
Group PD (n = 52) received paracetamol 4.5 mg/kg and dexmedetomidine 1 µg/kg as a bolus dose over 15 minutes prior to extubation, followed by continuous infusion (paracetamol 0.5 mg/kg/hr and dexmedetomidine 0.05 µg/kg/hr) and demand doses (paracetamol 1 mg/kg and dexmedetomidine 0.1 µg/kg) via PCA pump with a 30-minute lockout interval.
After conducting a thorough history, clinical examination, and investigations for all patients, informed and written consent was obtained from each participant. All patients were familiarised with the pain VAS scores and the use of PCA pumps in the preoperative care area. Every patient received the same anaesthetic treatment. A 5-lead electrocardiogram (ECG), pulse oximeter (SpO2), non-invasive automated blood pressure (NIBP), end-tidal carbon dioxide (ETCO2) and anaesthesia depth index (BIS) were used to monitor each patient as they entered the operating room. Both groups underwent preoxygenation with 100% oxygen for 3 minutes. Induction was achieved using inj. midazolam 0.04 mg/kg, inj. fentanyl 1.5 µg/kg, and titrated dose of inj. propofol 1–2 mg/kg body weight. Muscle relaxation was facilitated with vecuronium 0.1 mg/kg body weight, followed by adequate-size cuffed endotracheal intubation. Maintenance of anaesthesia was carried out with mixture of oxygen and air (FiO2 0.5), sevoflurane titrated to less than 1 MAC, propofol infusion adjusted according to the patient’s requirements. Additional doses of vecuronium for muscle relaxation and fentanyl for analgesia were administered as needed. Ventilation was maintained to keep ETCO2 levels between 35 and 40 mmHg. During the pneumoperitoneum in laparoscopic surgery, intra-abdominal pressure was maintained at 14 mmHg. Both groups used the same surgical procedure. A bolus dose of fentanyl 0.5 µg/kg was given to patients who had hypertension (mean arterial pressure > 20% higher than baseline) or tachycardia. The PCA pump was started 15 minutes prior to completion of surgery, and both groups received an inj. ondansetron 4 mg. Patients were reversed with neostigmine (40 µg/kg) and glycopyrrolate (10 µg/kg) after completion of surgery, and the endotracheal tube was removed and the patient was shifted to PACU. The patients in both groups were given paracetamol (10 mg/ml) and dexmedetomidine (1 µg/ml) as a postoperative analgesic via a PCA pump (Smith Medical ASD, Inc., USA). The dose and timing of drugs were administered as described above.[12]
The primary outcome was the VAS score at 1, 2, 4, 8, 12, and 24 hours postoperatively, and the analgesic requirement in the first 24 hours. The secondary outcome was the incidence of PONV in the first 24 hours. PONV was defined as at least one episode of nausea, vomiting, or retching, or any combination of these, within the first 24 hours following surgery. A four-point rating system (0 = none, 1 = mild, 2 = moderate, and 3 = severe) was used to ask patients to rate their level of nausea. At least one episode of vomiting or retching was considered postoperative vomiting, and the PONV score was 4.[13] Patients with VAS >4 were given a bolus dose of diclofenac aqueous (75 mg i.v. infusion) as a rescue analgesic. The second rescue analgesic inj. ketorolac 30 mg was used if the pain was not relieved by diclofenac. For moderate to severe episodes of nausea or vomiting, metoclopramide 10 mg i.v. was administered as a rescue antiemetic.
Atropine 0.6 mg i.v. was used to treat any episode of bradycardia (HR < 50/min). Any hypotension (MAP < 20% preoperative value) was managed with a 200–300 ml fluid bolus of normal saline. An intravenous injection of mephentermine 5 mg was administered if the fluid bolus was unable to relieve the hypotension. If the blood pressure remained low after two doses of mephentermine, a dopamine infusion was initiated to maintain blood pressure.
The sample size was estimated using a two-sided P level. Based on previous study,[11] the mean VAS score for patients receiving paracetamol is 5, with a standard deviation of 2. The expected mean VAS score for patients receiving the paracetamol-dexmedetomidine combination is 3.5, with a standard deviation of 1.5. Assuming a two-sided test with a significance level of 0.05 and a power of 0.8, the required sample size is approximately 48 patients per group. To account for potential dropouts, 52 patients were enrolled in each group.
Statistical analysis was performed using GraphPad Prism 7.0 software. Data were presented as Mean ± SD (standard deviation) or absolute numbers. The student’s t-test was used to analyse demographic data and the 24-hour paracetamol requirement. The Mann–Whitney test was used to analyse VAS scores. Fisher’s exact test was used to compare the incidence of PONV between groups. A P value of < 0.05 was considered statistically significant.
Results
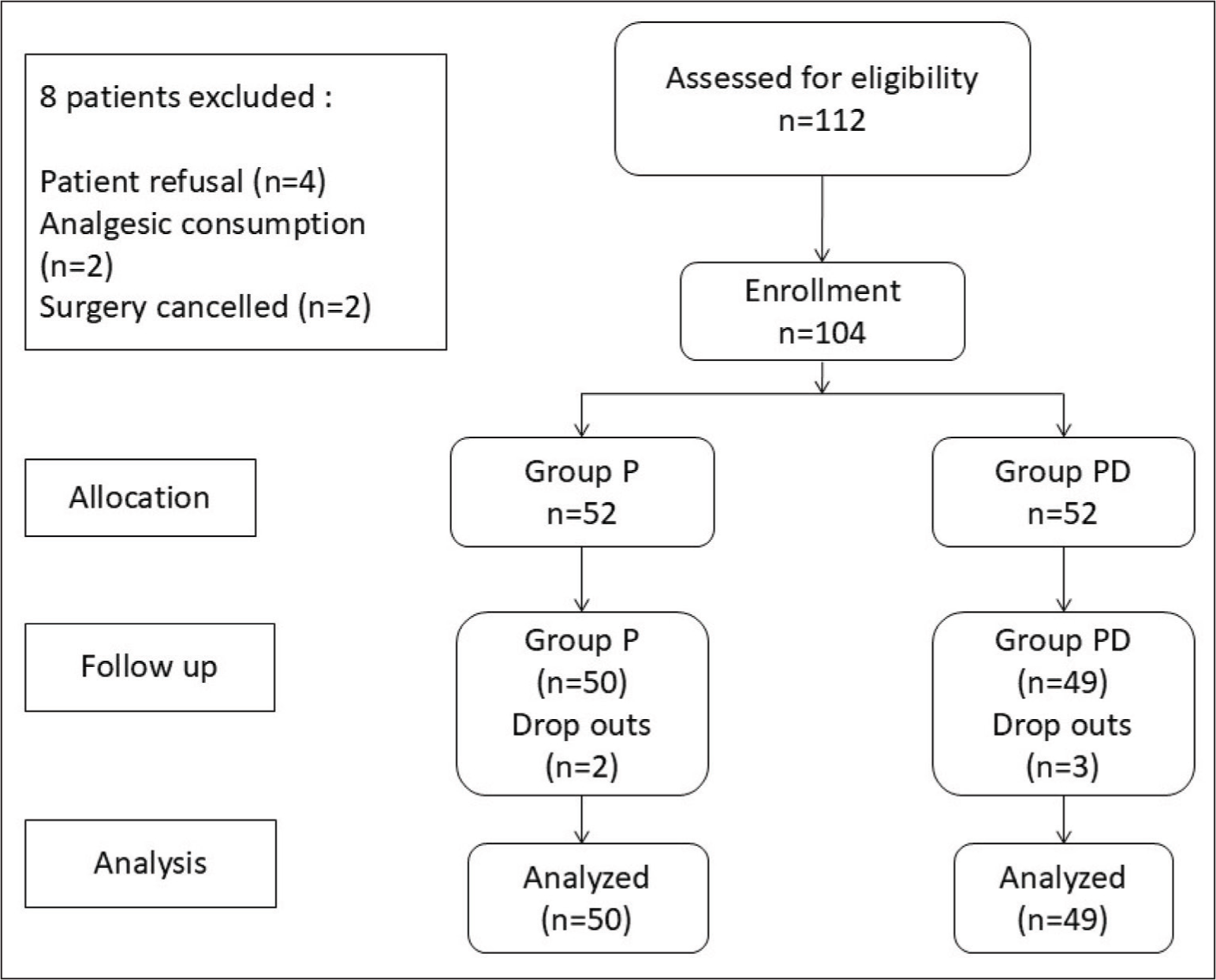
A total of 112 participants were initially assessed for eligibility. Eight participants were excluded: four refused to participate, two had consumed analgesics, and surgery was cancelled for two. This left 104 participants who were enrolled in the study and randomly assigned into two groups of 52 each (Group P and Group PD). During the follow-up phase, two participants dropped out from Group P and three from Group PD, leaving 50 and 49 participants, respectively, for analysis [Figure 1].
Study design
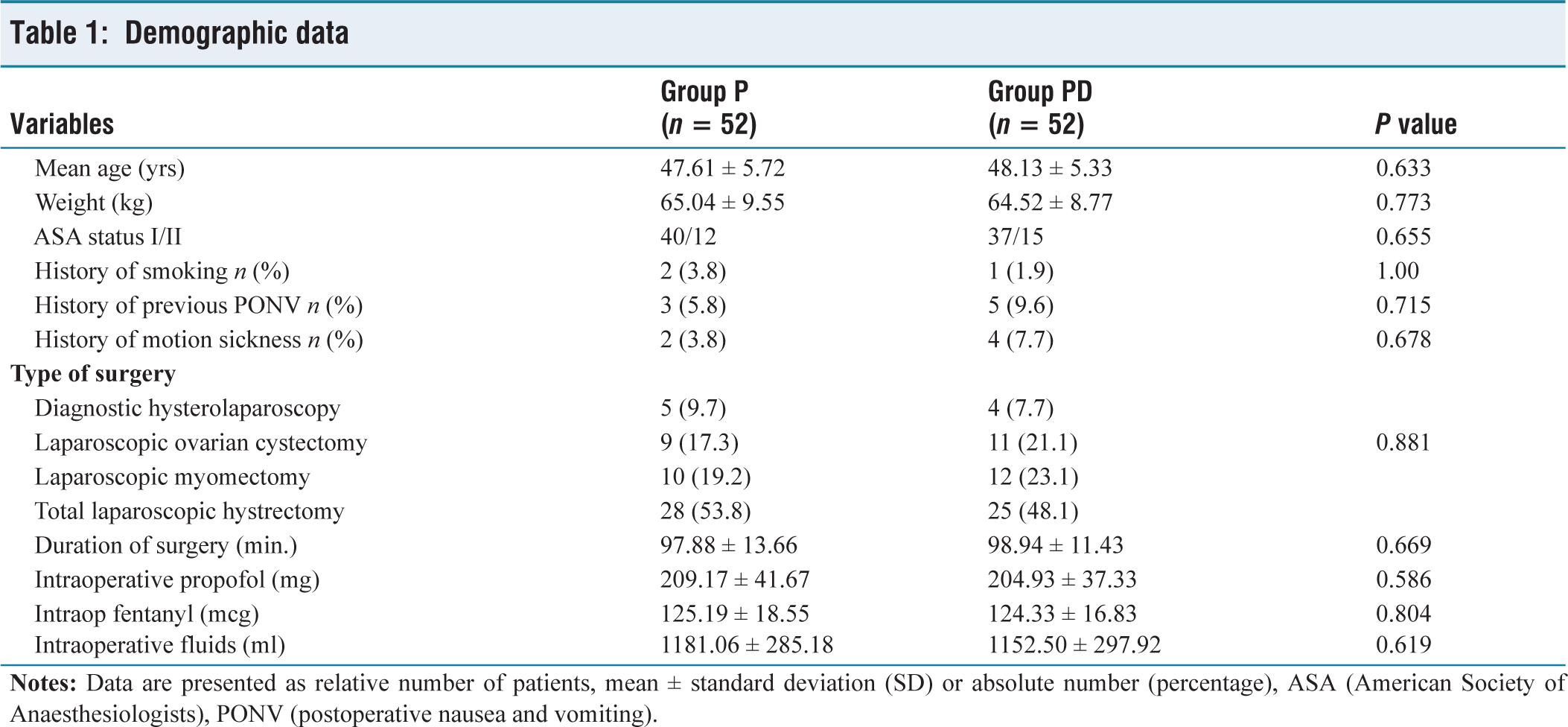
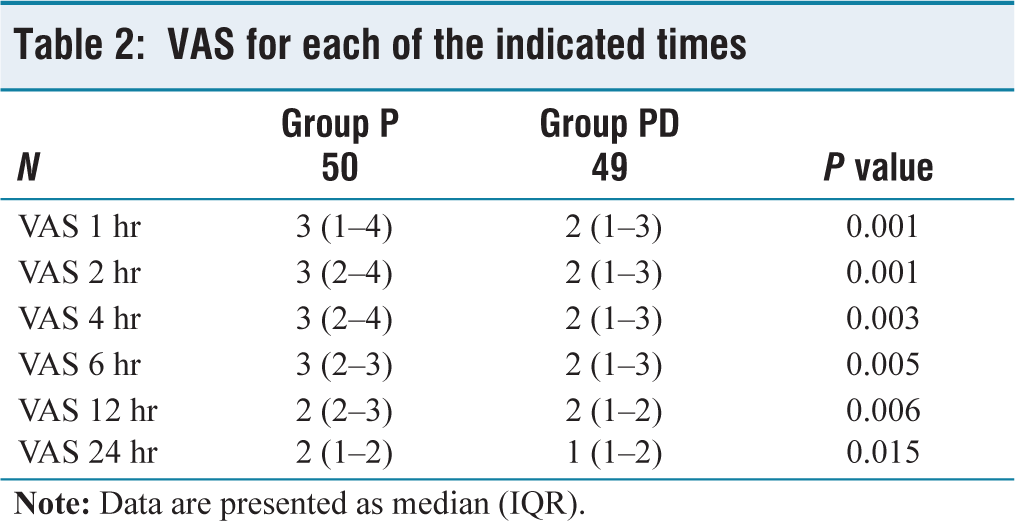
There was no significant difference in the demographic data (age, weight, ASA grade, Apfel score, type and duration of surgery, intraoperative propofol and fentanyl requirement and intraoperative fluid consumption) between the two groups (P > 0.05) [Table 1]. The primary outcome, VAS at 1, 2, 4, 6, 12 and 24 hours, was significantly lower in the Group PD compared with that in the Group P (P < 0.05) [Table 2]. Additionally, Group PD required significantly less paracetamol (1699.24 ± 329.90 mg) compared to Group P (2276.62 ± 405.51 mg) in the first 24-hour postoperative period (P < 0.0001) [Table 3].
Demographic data
VAS for each of the indicated times
Analgesics and rescue antiemetic requirement
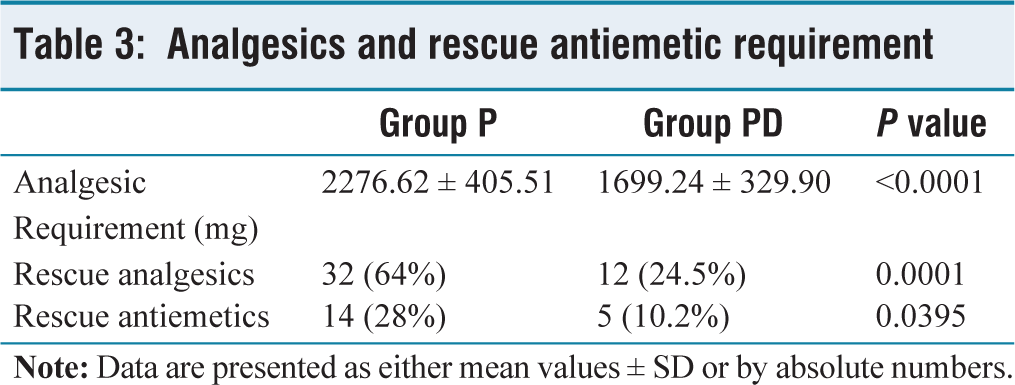
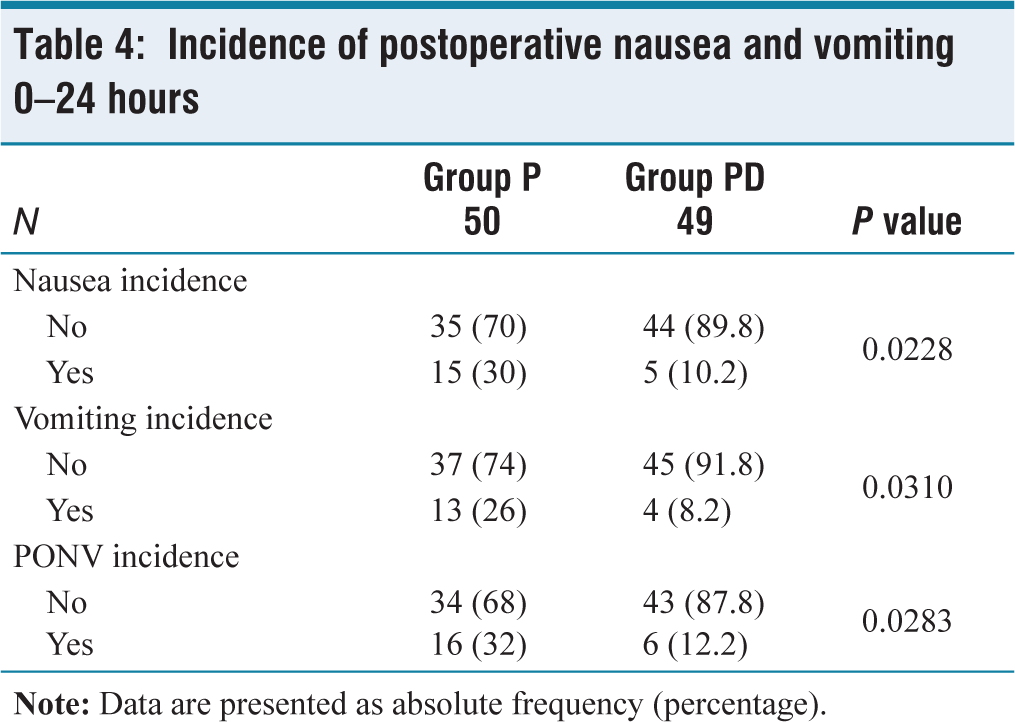
The secondary outcome, incidence of PONV in the first 24 hours post-surgery, was significantly lower in Group PD compared to Group P. Specifically, Group PD had a significantly lower overall incidence of nausea (10.2% vs. 30%, P = 0.0228), vomiting (8.2% vs. 26%, P = 0.0310), and PONV (12.2% vs. 32%, P = 0.0283) [Table 4]. Group PD also needed fewer rescue analgesic interventions [12(24.5%) vs. 32(64%), P = 0.0001] and antiemetic interventions [5(10.2%) vs. 14(28%), P = 0.0395] than Group P [Table 3]. In Group P, 20% patients also require a second rescue analgesic.
Incidence of postoperative nausea and vomiting 0–24 hours
Hypotension was observed in only two patients (4%) within 1 hour after surgery in Group PD, which was managed with a single dose of mephentermine 5 mg i.v., and two patients (4%) in Group PD developed bradycardia within 30 minutes after surgery, which required atropine 0.6 mg i.v.
Discussion
Laparoscopic hysterectomy has become the preferred, acceptable, and safe approach for patients with progressive uterine abnormalities due to its advantages, such as quicker return to normal activities, early resumption of nutrition, enhanced postoperative mobility, and reduced postoperative complications. However, labile haemodynamics can occur due to positional changes during laparoscopic surgery, exacerbated by surgical stress, especially following pneumoperitoneum establishment.[2] General anaesthesia with muscle relaxation and tracheal intubation is preferred for lower abdominal laparoscopic procedures.[14]
A primary concern for anaesthesiologists is selecting an optimal drug regimen to manage exaggerated intraoperative haemodynamic responses and to alleviate postoperative pain and PONV in patients undergoing laparoscopic hysterectomy. Uncontrolled postoperative pain can lead to anxiety, depression, patient dissatisfaction, haemodynamic instability and PONV. The ideal analgesic regimen for postoperative care should minimise side effects, have negligible effects on major organ systems, and avoid significant drug interactions, while providing rapid and effective pain relief.
There are various studies with a single analgesic drug or multimodal analgesics for postoperative pain management in laparoscopic surgery.[3,4] Wang X et al.[10] use dexmedetomidine alone for intravenous PCA after gynaecological laparoscopic surgery and confirmed that dexmedetomidine PCIA is as effective as fentanyl PCIA for reduction of VAS scores at different times after surgery. Similarly, a study in patients undergoing laparoscopic abdominal hysterectomy found that intraoperative dexmedetomidine, administered as a continuous infusion at 0.4 mcg/kg/h, significantly improved postoperative analgesia with reduced dose of morphine in PCIA.[15] Paracetamol alone was more effective than dexmedetomidine alone for control of postoperative pain in laparoscopic cholecystectomy demonstrated by various authors.[16,17] In contrast to this, another study demonstrated superior efficacy of PCIA dexmedetomidine compared to paracetamol at all time intervals postoperatively.[11]
In view of the advantages and disadvantages of these studies, we used a new combination of paracetamol-dexmedetomidine for the first time in laparoscopic surgery for postoperative pain management. In our current study, we administered intravenous paracetamol (Group P) and the paracetamol-dexmedetomidine combination (Group PD, multimodal analgesic) as a postoperative analgesic via a PCA pump and revealed that VAS scores were significantly decreased with the paracetamol-dexmedetomidine combination compared to paracetamol alone at all time points during the first 24 hours postoperatively. Additionally, paracetamol requirements in the first 24 hours postoperative period were also decreased with the addition of dexmedetomidine. The result of our study is consistent with Imani F et al.[18] who conducted a study on caesarean patients and found that adding dexmedetomidine to PCIA reduces the amount of paracetamol needed by up to 2 gm for sufficient postoperative pain relief within the first 24 hours.
The different sites of action of paracetamol and dexmedetomidine in the nervous system may be the cause of superior analgesia in Group PD. While paracetamol works by inhibiting prostaglandins and activating descending serotonergic inhibitory pathways, dexmedetomidine’s analgesic effect is believed to be mediated by α2-receptor binding in both central and spinal cord α2-receptors. Hyperpolarisation of interneurons and decreased release of pronociceptive transmitters like glutamate and substance P inhibit the transmission of pain.
Opioids are commonly used for postoperative analgesia, but complications were also a concern, particularly PONV, respiratory depression and constipation. According to Kim et al.[6] patients of laparoscopic hysterectomy experienced a 30.3% incidence of PONV when receiving fentanyl PCIA. Similarly, Wang X et al.[10] compared dexmedetomidine and fentanyl PCIA and demonstrated that dexmedetomidine PCIA has decreased incidence of PONV (5% compared to 31% in fentanyl group) following gynaecological laparoscopic surgery. In view of the high incidence of PONV in laparoscopic surgery by using opioids, we successfully used an opioid-sparing technique. In our study, we used paracetamol-dexmedetomidine combination and observed a significant reduction in PONV during the first 24 hours postoperative period (12% vs. 32%).
Our study aligns with the findings of Massad et al.[19] who assessed the effect of adding dexmedetomidine to a balanced anaesthetic technique on PONV after laparoscopic gynaecological surgeries and found that combining dexmedetomidine with other anaesthetic agents resulted in more balanced anaesthesia and a significant decrease in the incidence of PONV. Possible explanations for the lower incidence of PONV in the dexmedetomidine group may be related to several factors. First, dexmedetomidine reduces the consumption of intraoperative and postoperative opioids. Second, it avoids the use of nitrous oxide and inhaled anaesthetics.[20] Furthermore, dexmedetomidine binds to alpha-2 presynaptic inhibitory adrenoceptors in the locus coeruleus, reducing noradrenergic activity, which may explain its antiemetic effect.
According to Apfel et al.’s comprehensive review and meta-analysis, paracetamol can decrease the incidence of PONV by either a direct antiemetic action or a reduction in post-surgical pain, which may be the cause of PONV.[21] The possible mechanism of direct antiemetic effect of paracetamol is as follows. The brain metabolises acetaminophen into AM404, a metabolite that can prevent anandamide, a well-known cannabinoid CB1 and CB2 receptor agonist, from being reabsorbed. Reduced anandamide levels have been linked to a higher incidence of nausea and vomiting in people.[22] Acetaminophen may therefore just increase anandamide levels, which would have a direct influence on PONV. Cok et al.[23] also confirmed that paracetamol significantly reduced PONV during the first 24 hours after strabismus surgery in children.
In our study, we selected metoclopramide as a rescue antiemetic and diclofenac as a rescue analgesic in patients who complained of PONV and a higher VAS score, because their mode of action differs from the study drugs. The second rescue analgesic, ketorolac, is also required by 20% patients in Group P. This signifies paracetamol alone is not effective for pain management in laparoscopic surgery. To improve analgesia and lessen adverse effects associated with individual classes, Schwenk ES et al. also defined the use of multiple analgesic medications that target distinct receptors along the pain pathway.[24]
We limited our study’s assessment to the first 24 hours postoperatively, but a longer-term follow-up could reveal delayed complications, sustained pain relief, and potential adverse effects of study drugs. This is a single-centre study, so its external validity is limited; if collaborative efforts across multiple centres were included, then it would strengthen the conclusions.
In conclusion, our study demonstrated that paracetamol-dexmedetomidine combination as a PCIA in laparoscopic hysterectomy decreased VAS score, analgesic requirement, along with a reduction in PONV in the first 24 hours postoperative period compared to paracetamol alone. So, dexmedetomidine can be a useful adjuvant when used with paracetamol in PCIA in laparoscopic hysterectomy surgery.
Supplemental material
Supplemental material for this article available online.
Footnotes
Acknowledgements
The authors thank Mr Melu Ram Sahu and the surgical staff for all their assistance and suggestions during the current study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
AHB/CR/15/30-06-2022.
Informed consent
Informed consent was obtained from all patients.
Credit author statement
All authors contributed to the study conception and design.
VKS: Data analysis, Manuscript preparation, Manuscript editing, and review.
HG: Literature search, Data acquisition, Manuscript preparation.
SB: Literature search, Manuscript preparation, Manuscript review.
KB: Data acquisition, Manuscript preparation, and editing.
KB: Literature search, Manuscript review.
NT: Literature search, Data acquisition, Manuscript editing.
Data availability
Data should be available as required.
Use of artificial intelligence
None.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.