
Abstract
Background:
Autism spectrum disorder (ASD) is a neurodevelopmental syndrome which results in intellectual disability, reduced speech or communication, unusual restricted, repetitive behaviours to functionally able children. Usually expressed in the toddler and preschooler age group. Early diagnosis of ASD helps to intervene earlier which will lead to the betterment of the children along with the family and indirectly the nation as well.
Methodology:
A prospective study was conducted on children between the age of 12–59 months attending a tertiary care hospital after obtaining a ethical clearance from institutional ethical committee. Assessment was done using MCHAT-R/F questionnaire. All the data collected were analysed using SPSS, Version 23.0.
Results:
Magnitude of ASD was 1.7% commonly affecting 24–30 months age group and upper lower socioeconomic status. Factors like increased maternal age, consanguinity, prolonged labour, foetal distress, low birth weight, birth asphyxia, neonatal seizures, neonatal sepsis, alteration in temperament, sleep disturbances, hyperactivity and delayed attainment of milestones were found to be positively associated with ASD.
Conclusion:
Autism does have association with prenatal, perinatal, neonatal and postnatal risk factors or conditions. Its pathogenesis is served by such momentous mediators. Hence presence of these factors should be considered to avoid the danger of autism onset in children.
Introduction
Autism spectrum disorder (ASD) leads to intellectual disability, restricted and repetitive behaviour, reduced speech or communication and functional or developmental disability. Thus ASD is also called as neuro developmental syndrome.[1,2] ASD usually presents in the first few years of life.[3] Majority of parents also notice behavioural abnormalities in their children during the first few years of life.[4–6] ASD is in a increasing trend worldwide and is estimated to be 61.9 per 10,000 globally in 2012.[7] Many indirect causes for autism has been identified which range from genetic causes to the direct insult. The genetic causes are mutation or defective expression of the gene. Environmental causes like pollutants, pesticides, prenatal factors like consanguinity or increased maternal or paternal age, antenatal factors like gestational diabetes, pregnancy induced hypertension, infections during pregnancy, smoking or alcohol in pregnancy, increased stress, perinatal factors like prolonged labour, premature rupture of membranes, preterm delivery, instrumental delivery, hypoxic insults, neonatal seizures, neonatal hyperbilirubinemia and neonatal sepsis are found to be indirectly leading to autism.[7] About 1 in 100 children in India under age 10 has autism, and nearly 1 in 8 has at least one neuro-developmental condition.[8] ASD has a male predominance as in 1 in 54 boys.[9] ASD is either under-diagnosed or diagnosed very late which may be due to various reasons like less knowledge or lack of awareness regarding the availability of screening tools for diagnosing ASD.[10,11]
These various risk factors are seen to contribute to autism either independently or they combine with the other factor and have a synergistic cause which could possibly be a reason for the broad spectrum of characteristics which are seen in a child or individual with autism. Screening and detecting ASD earlier is important as it helps to intervene earlier which will lead to the betterment of the children along with the family and indirectly the nation as well. The present study was done in view of finding the incidence of ASD, the most common early signs of autism and to assess the factors influencing and their association with the ASDs among preschoolers and toddlers who visit the tertiary care hospital, Kanchipuram district.
Methods
A Prospective study was conducted on children between the age of 12–59 months attending a tertiary care hospital in a period of 18 months from January 2020 to June 2021. Inclusion criteria included all children between 12–59 months visiting Shri Sathya Medical College and Research Institute, whose parents are willing to participate in this study and exclusion criteria were those whose parents were not willing and children diagnosed with other neurological disorders. Sample size was calculated based on Practical Manual by WHO (where the safest choice for the population proportion since the sample size required is largest) P = .5 (50%) and is estimated to be 2,400 [with the formula N = z2p(1-p)/d2]. Study was done after obtaining informed consent from the parents or guardians (written in the local language). Ethical clearance was obtained from institutional ethical committee, and confidentiality was maintained throughout the study.
Demographic details (age of the child, gender of the child) and details regarding presence of any risk factors like prenatal factors (maternal or paternal age at conception, consanguinity, socioeconomic status, education of parents), antenatal factors (antenatal Hormones, thyroid profile, hypothyroidism, GDM, PIH, gestational infection like respiratory or urinary), perinatal factors (prolonged labour, foetal distress, gestational age during delivery, premature rupture of membranes, delivery at government or private hospital, mode of delivery, birth asphyxia, birthweight) or neonatal factors (alteration in temperament, sleep disturbances, delayed milestones, hyperactivity, breastfeeding, immunisation, child’s thyroid status, neonatal seizures) were obtained from parents.
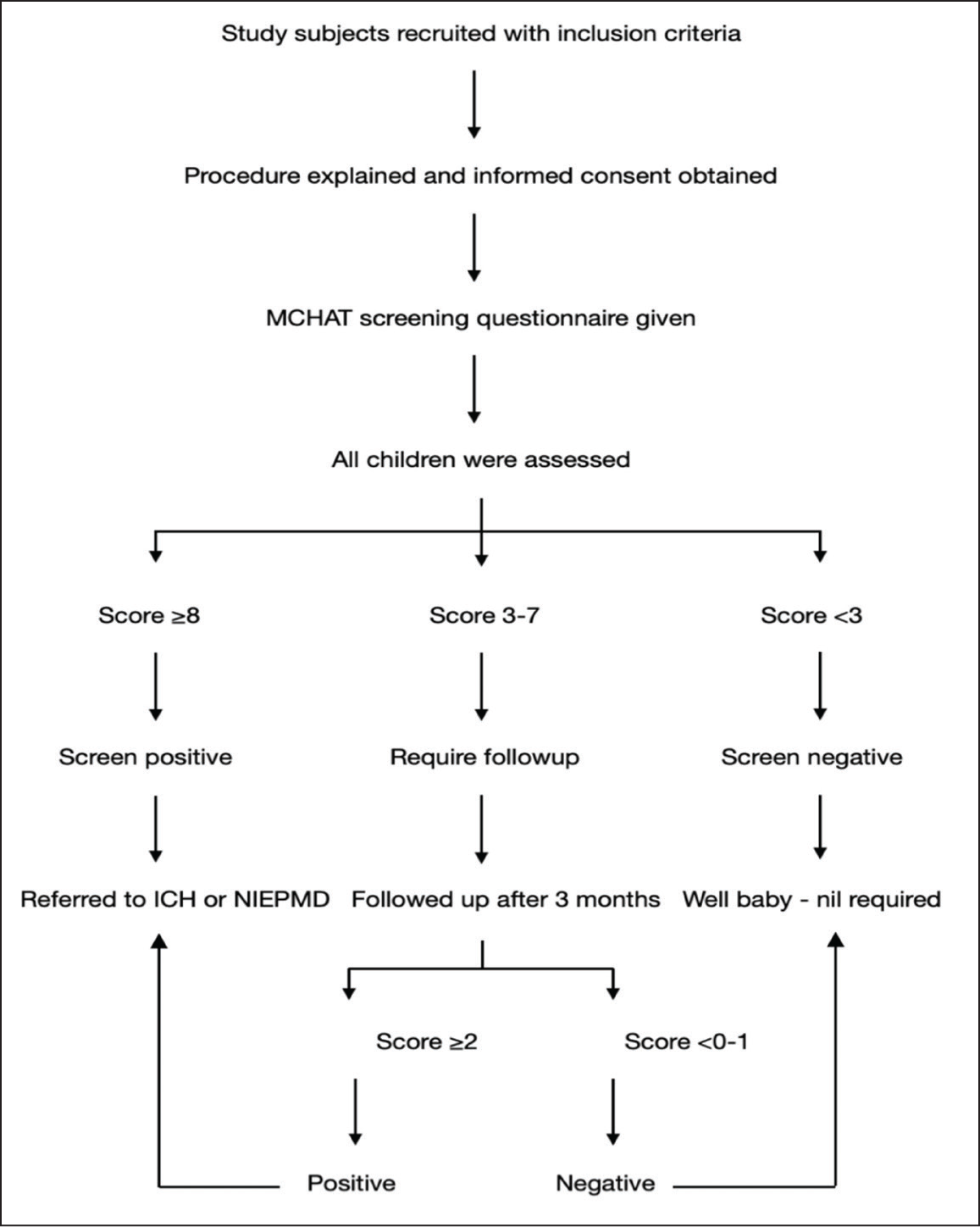
Assessment of children were done by interviewing parents using MCHAT-R/F questionnaire (M-CHAT-R/F; Robins, Fein, & Barton, 2009). All the children were also assessed for eye contact, pretend play, ability to follow a point, producing a point, ability to hear or turn towards sound sources, response to their names, expression of their face and language and communication and impressions were marked as Normal, abnormal or possibly abnormal. MCHAT questionnaires were given to the parents, which were translated into local language (after a pilot study). Questionnaire consists of 20 yes/no response format questions. All questions except 2, 5, and 12 indicate “YES” which means towards ASD risk. The total score is calculated and is again graded as low (a score of 0–2) or medium (a score of 3–7) or high risk or screen positive (score ≥8) for ASD. In case of children falling in medium risk, they are asked review after three months and reviewed using MCHAT-R/F, which has same items with pass/fail format. On follow up the child has screened positive if M-CHAT-R/F score remains at 2 or higher, whereas child is considered screen negative if score is 0–1. The screened positive children are further referred for diagnostic evaluation for early intervention. Methodology is shown in Figure 1.
Methodology
Also history or presence of any features of autism like no one meaningful word, no two meaningful words, no interaction, no pointing, or meaningful gestures, no social smile, no babbling, not responding to name, not responding to sounds, voices, or name, reduced expression, rejection of cuddles, reduced Eye Contact, reduced joint attention, regression of language, repetitive stereotypic movements, unusual attachment to one toy or object are noted to detect what are the common early signs of autism. All the data collected were entered in Excel sheet and analysed using SPSS, Version 23.0. Test of significance used were Chi-square test and Fisher’s exact test and P value of < .05 was considered statistically significant.
Results
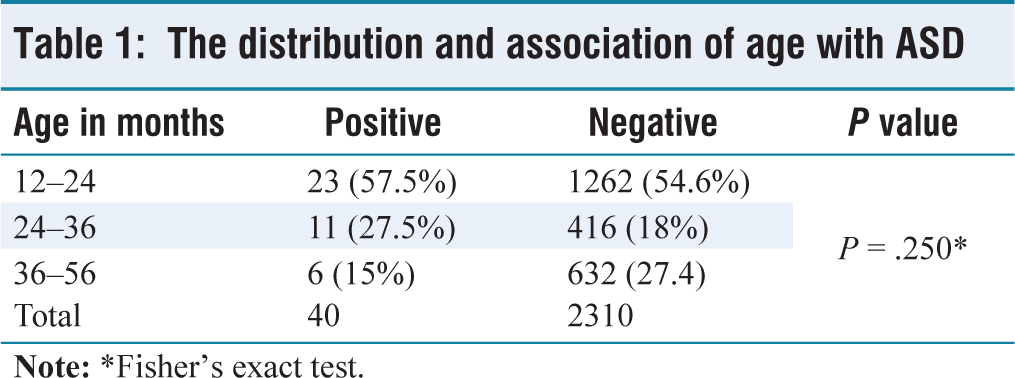
Out of the 2400 children screened, 25 children scored ≥8 and we considered screen positive and 146 children fell in the follow-up category, out of which 50 children did not turn up in follow up hence they were excluded. Out of the 96 children who were followed up after a three-month period, 15 children failed to score ≤2 in the M-CHAT-R/F questionnaire and were considered as screen positive. Hence, around 40 children were considered to be screen positive among the total 2,350 children included. In our study, the incidence of ASD was 1.7%. The mean age group of the children included in the study was 28.55 ± 11.82 months, and the incidence of ASDs was observed to be more in 24–30 years age group (6 out of 151 had autism) and was statistically significant. But overall, no statistically significant difference was observed between the ASD and age. The distribution and association of age with ASD are shown in Table 1. Most of the children screened were females (51.2%) and gender did not have significant association with incidence of ASD. 54% of screened population belonged to middle class, 24.7% belonged to lower middle class, 16.8% belonged to upper middle class. Incidence of ASD was more among those who belonged to upper lower class and socioeconomic status was observed to be statistically significant. Based on parents’ education till 12th standard, at least one parent was educated (42%), both parents (31%), both were not educated (26%). Parents’ education was not statistically significant with incidence of ASD. Around 5.4% had consanguineous marriages, out of which majority of consanguineously married mothers fell in age group of 18–22 years. There was a statistically significant association between consanguinity and ASD. The distribution and association of gender, socioeconomic status, parents’ educational status and consanguinity with ASD are shown in Table 2.
The distribution and association of age with ASD
The distribution and association of gender, socioeconomic status, parents educational status and consanguinity with ASD
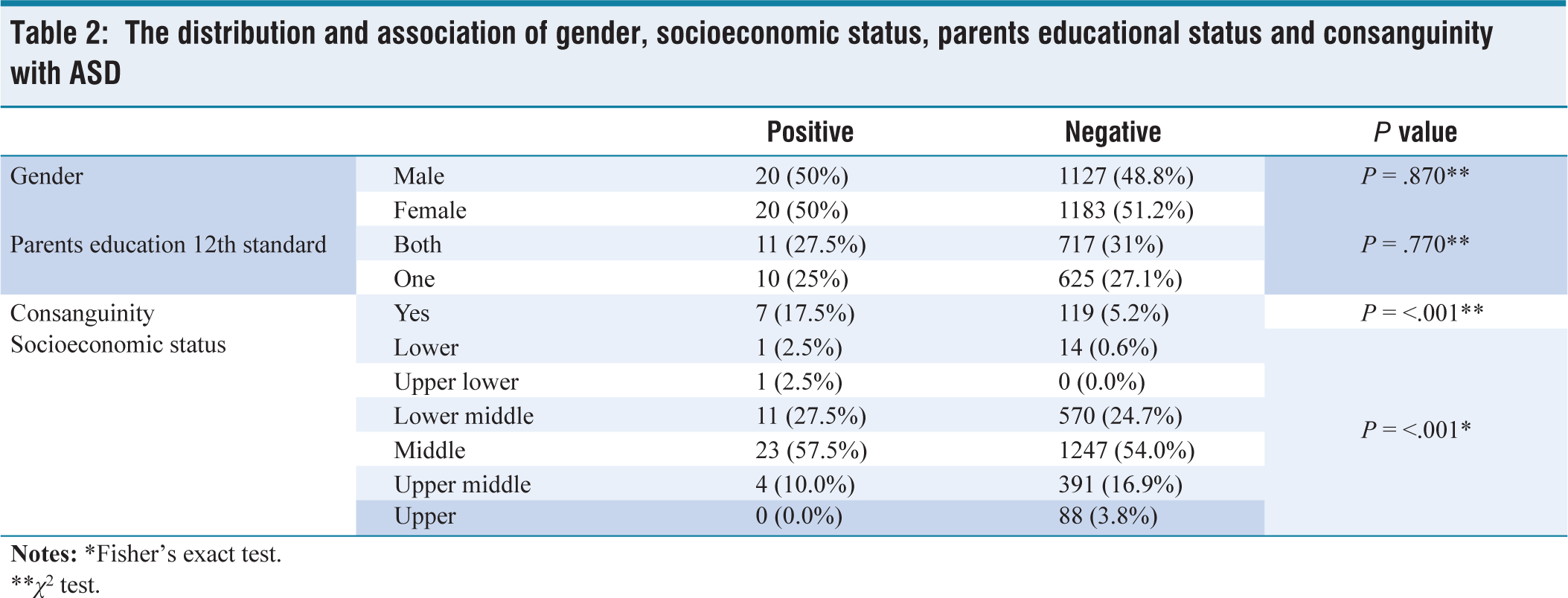
**χ2 test.
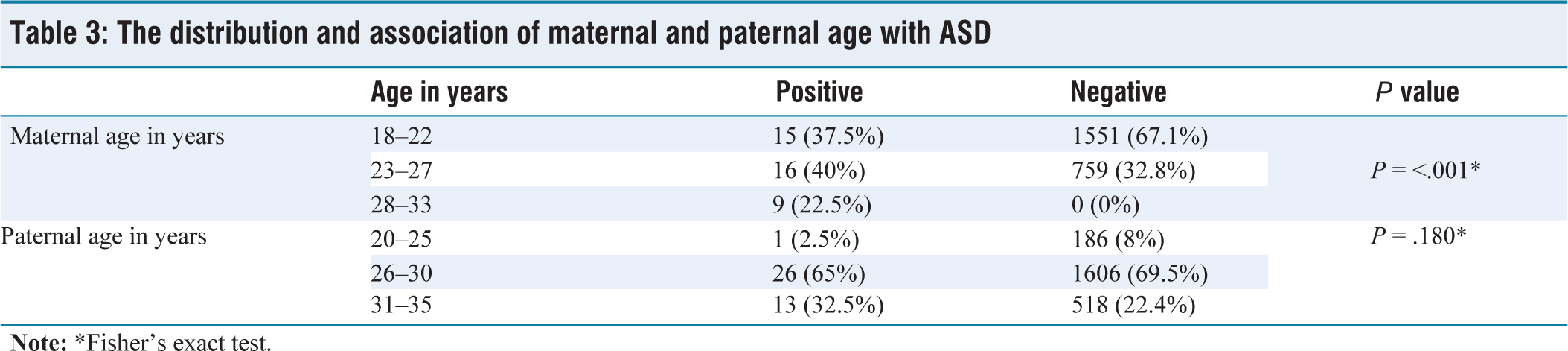
The maternal age was segregated into three divisions 18–22 years, 23–27 years and ≤28 years. The mean maternal age was 21.81 ± 2.71 years, with the majority in 18–22 years (66.6%). The incidence of autism was seen more in mothers falling in age group of ≥28 years and was statistically significant. The mean Paternal age in the present study was 28.89 ± 2.70 years, with the majority in between 26 and 30 years (69.4%). There was no statistically significant association observed between ASD and paternal age, as the P value calculated to be > .05. The distribution and association of maternal and paternal age with ASD are shown in Table 3.
The distribution and association of maternal and paternal age with ASD
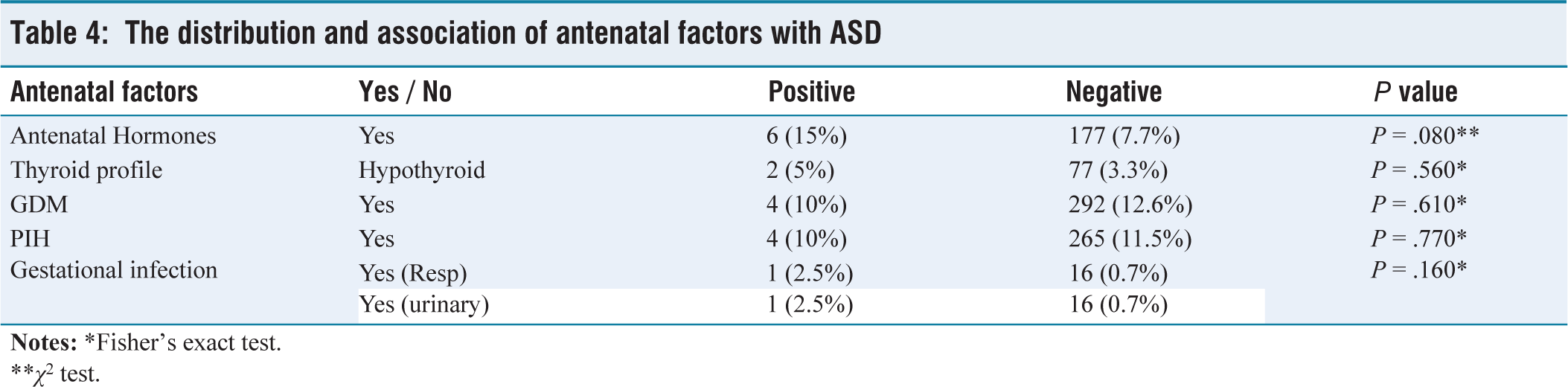
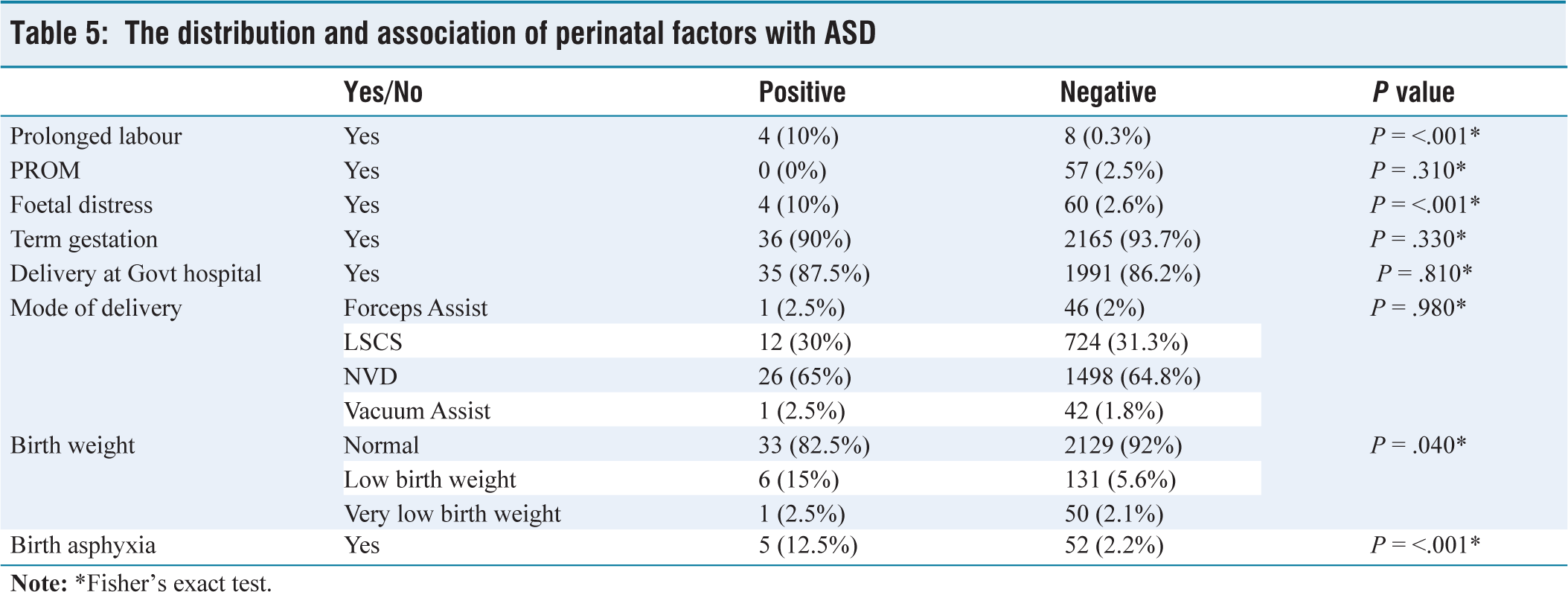
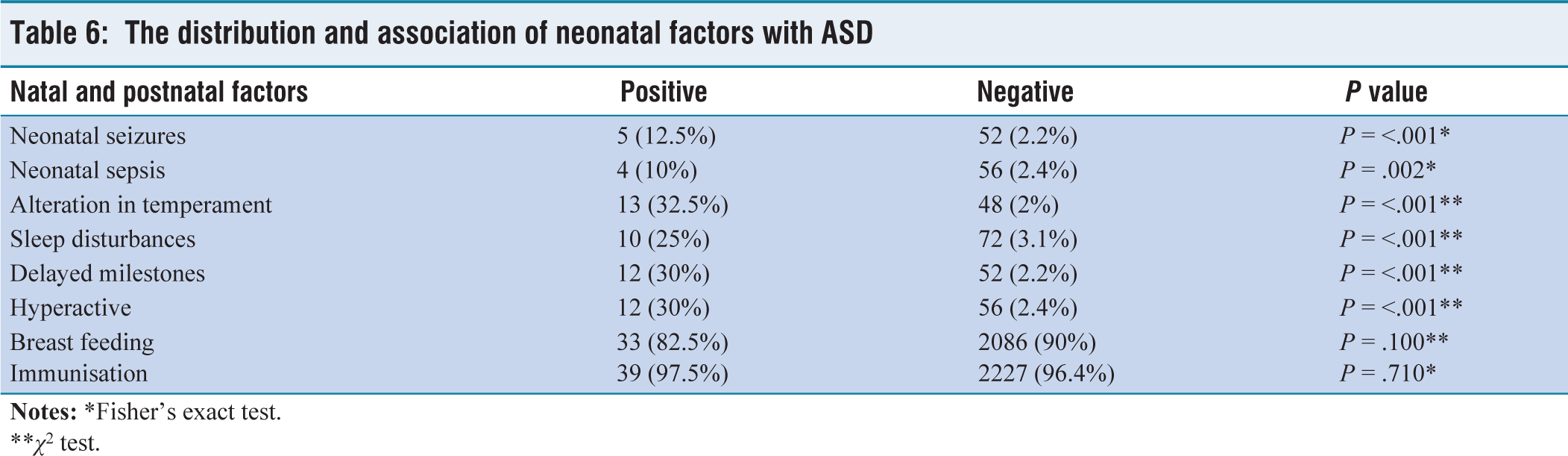
There was no significance of incidence of autism with antenatal factors in our study. The distribution and association of antenatal factors are shown in Table 4. There was a statistically significant incidence of autism with prolonged labour, foetal distress, birth weight and birth asphyxia in our study. The distribution and association of perinatal factors are shown in Table 5. Factors such as neonatal seizures, neonatal sepsis, alteration in temperament, sleep disturbances, delayed milestones and hyperactivity were positively associated with ASD. The distribution neonatal factors is shown in Table 6.
The distribution and association of antenatal factors with ASD
**χ2 test.
The distribution and association of perinatal factors with ASD
The distribution and association of neonatal factors with ASD
**χ2 test.
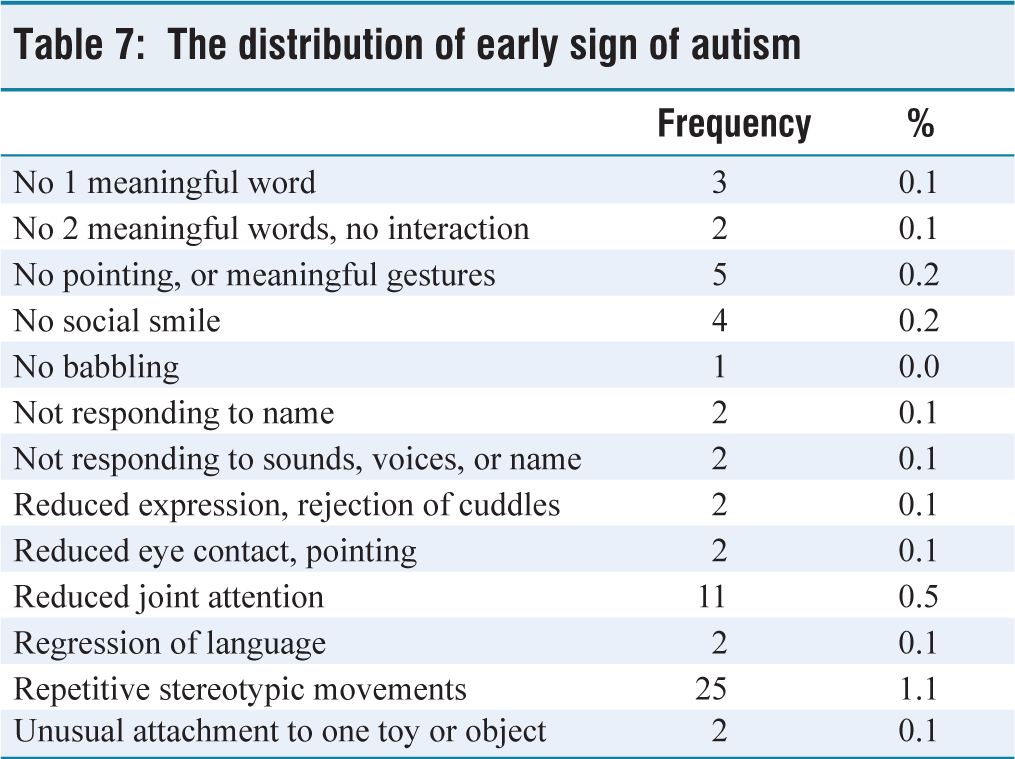
Among the early signs of autism, the most common were repetitive stereotypic movements, followed by reduced joint attention and then by no social smile and no pointing, or meaningful gestures. The distribution of early signs of ASD is shown in Table 7.
The distribution of early sign of autism
Discussion
In our study, the incidence of ASD was 1.7%. Hidalgo et al. conducted a study in 2021 that showed an overall estimated prevalence was 1.53% (1.78% in preschoolers; 1.30% in primary school children).[12] A cross-sectional two-phase study on children of 1–10 years of age was conducted by Raina et al. showed a prevalence rate of 0.9/1,000.[13] Nair et al. conducted a cross-sectional study in Kerala in 2014, which showed an incidence of 17 autistic children.[14] Poovathinal et al. conducted a prospective study and showed a prevalence of ASD as 23.3/10,000.[15] Rudra et al. also conducted a study in 2017, and in their study, six people were screened positive.[16] Joseph et al. conducted a study of children aged 18–36 months and calculated prevalence with screen positive of autism, that is, M-CHAT-R score >7, and the rate was 0.55%.[17] In relation to gender, our study reported an equal distribution. Ts J et al. and Akhter et al. reported an incidence rate of 1.3% and 1.24% using MCHAT questionnaire.[18,19] Biard et al. and Mandy et al. reported 4:1 (male:female).[20,21] Majority of studies like Bhatt et al. reported a male predominance with a ratio of 3.6:1 (males:females).[22]
In view of maternal age and autism, our study showed a positive relation. Sandin et al. conducted a Meta-Analysis which included almost 25,687 ASD cases, which showed younger the mothers, lesser is the risk for autism.[23] One more study, which was done by Lisa et al. reported every 10-year increase in maternal age more is the risk of autism.[24] Regarding consanguineous marriage, our study showed more incidence in consanguineously married parents; similarly, a study done by Fouad et al. showed that marriages between 1st and 2nd cousins reported a higher risk for ASD.[25] Al Salehi et al. also reported that the higher the rate of consanguinity higher is the incidence of ASD due to the high incidence of autosomal recessive genes.[26] Regarding socio-economic status our findings were similar to Raina et al. A risk of autism on GDM mothers was shown by Xiang et al.[27] A systematic review of all the observational studies (40 cohort studies) was conducted by Gardener et al.[28] They assessed all the risk factors for autism and reported that there are many factors which lead to autism like abnormal presentation during delivery or foetal distress or injuries during birth or multiple gestation or antepartum or postpartum haemorrhage or low or very low birth weight or congenital abnormalities or difficulties in feeding or neonatal anaemia or hyperbilirubinemia. Leavy et al. concluded that lower the gestational age higher is the incidence of autism.[29] There are not many studies done on analysing the association of autism with the multiple possible risk factors. In our study, many risk factors such as increased maternal age, consanguineous marriage, foetal distress, prolonged labour, birth asphyxia, birth weight, neonatal sepsis and seizures, hyperactivity, alteration in temperament, developmental delay, sleep disturbances were positively associated with incidence of ASD.
Conclusion
Given that autism is an epigenetic disorder in which multiple risk factors, like antenatal or prenatal or perinatal or neonatal risk factors, are the most momentous mediators in its pathogenesis. Thus, earlier detection of these factors or considering these factors to screen for autism in children might prevent the danger of autism onset in children.
Recommendations
Prevention of risk factors might help in reducing the autism in children, like increased maternal or paternal age, consanguinity, paying attention to the child’s developmental milestones and behaviour, avoiding mental stress, scheduled screening of babies born to mothers with risk factors and improving mother-infant interactions more.
Limitations
Although our study shows a positive association between the incidence of autism and certain risk factors, it was still unclear whether these factors play a primary or secondary role in the development of autism, as they lack the evidence of etiopathogenesis. Also, in our study, all the factors were examined individually, and hence we are unaware whether there is more chance of autism if these factors have synergistic role in incidence. Other factors like parenting style or behaviour, stress and emotion during and after pregnancy, environmental factors like pollutants and their impact on a child’s development for incidence were not included in the study. Further studies are required to correlate other factors which can lead to ASDs.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Approval No. 2019/541.
Informed consent
Patient information sheet, Questionnaires: Attached as annexures.
Credit author statement
LB participated in conceptualisation, data analysis, literature search, investigations, and draft preparation, review and editing. SPD and SP participated in conceptualisation, investigation, supervision, data analysis and manuscript editing. KSV participated in methodology and draft editing All the authors reviewed and approved the manuscript.
Use of artificial intelligence
Nil.