
Abstract
Background and Aims:
Emphysema is a type of chronic obstructive pulmonary disease caused primarily by smoking. Early detection of emphysema in asymptomatic smokers is challenging, as conventional methods such as chest radiography and spirometry are not effective for identifying early-stage disease. High-resolution computed tomography (HRCT) has become a sensitive tool for detecting early emphysematous changes, particularly in smokers.
Methodology:
This hospital-based cross-sectional study included 50 asymptomatic smokers aged 25–50 years, all of whom smoked at least 5 cigarettes daily for over 5 years. Participants underwent clinical examination, chest radiography, spirometry, and HRCT scans (inspiratory and expiratory). The aim was to detect early emphysema in smokers with normal spirometry and radiographs.
Results:
Out of 50 subjects, 30 (60%) showed evidence of emphysema on HRCT. Air trapping was the most common finding (77%), followed by bullous emphysema (56%). Emphysema was predominantly found in the upper lung zones (60%). Air trapping was more frequent in subjects with a smoking history of more than 10 pack-years, while no emphysema was detected in subjects with fewer than 5-pack years.
Conclusion:
HRCT is a valuable tool for detecting early emphysema in asymptomatic smokers. The presence of air trapping on expiratory scans can serve as an early marker of emphysema, even when chest radiographs and spirometry appear normal. Early detection may help prevent further disease progression and improve patient outcomes.
Keywords
Introduction
According to the American Thoracic Society, emphysema is pathologically defined as an abnormal, permanent expansion of the airspaces beyond the terminal bronchioles, along with the destruction of their walls, without any evident fibrosis. On computed tomography (CT) imaging, emphysema appears as regions with unusually low density and altered vascular patterns. Smoking significantly elevates the risk of illness and death due to chronic obstructive pulmonary disease (COPD), although this risk is generally lower with cigarettes than with pipes or cigars. Additionally, approximately 20% of COPD cases are unrelated to smoking.
The inflammation model suggests that smoking and other inhaled irritants trigger the accumulation of inflammatory cells in the lungs and airways. The substances released by these cells damage lung tissue and interfere with the normal repair processes. This heightened inflammatory response can lead to excessive mucus production (chronic bronchitis), tissue damage (emphysema) and impaired repair and defence functions, resulting in inflammation and scarring of the small airways (bronchiolitis).[1] Thus, COPD is a disease representing the complex alterations in the structure and function of the airways, lung parenchyma and pulmonary vasculature.[2]
Pre-COPD is said to be present in individuals with structural lung lesions (e.g., emphysema) and/or physiological abnormalities (including low forced expiratory volume in 1 s (FEV1), gas trapping, hyperinflation, reduced diffusing capacity of the lungs for carbon monoxide and/or rapid FEV1 decline) without airflow obstruction. Although they are susceptible to developing airflow obstruction over time, not everyone does so.[3] Accurately evaluating the presence and severity of emphysema during a patient’s lifetime is challenging, as clinical examinations, pulmonary function tests and chest X-rays often do not reliably correspond with the actual pathological changes.[4]
Hence, a non-invasive method with the ability to detect pathological changes at an early stage is extremely valuable, as it enables physicians to address risk factors in asymptomatic individuals—especially since emphysema often begins years before any symptoms appear in susceptible smokers. Traditional chest X-rays are poor indicators of disease severity and are not effective in identifying COPD in patients without noticeable emphysema. However, high-resolution CT (HRCT) has recently proven to be a highly sensitive tool for detecting early-stage emphysema. This study aims to identify early, symptomless emphysema in current smokers using both inspiratory and expiratory HRCT scans—changes that typically remain undetected through standard chest X-rays and spirometry.
A study was published in the ERS journal in 2024, which examined the effect of <10 pack-years on the development of emphysema. The study showed that even low levels of smoking, below the critical threshold of 10 pack-years, can elevate the risk of developing COPD in middle-aged adults within 5 years. These individuals also face a higher likelihood of experiencing severe flare-ups and premature death over the following four decades.[5]
Considering that a growing number of individuals smoke occasionally or at low levels, our study has important public health implications. As compared with never-smokers, low-rate smokers demonstrated increased disease risk, despite a relatively low threshold of lifetime smoking exposure (6.4 pack-years).[6]
The United States Preventive Services Task Force recommended against screening for COPD in asymptomatic adults. However, this is not applicable to populations at increased risk for COPD.[7]
Aim
The present study aims to detect early emphysematous changes in asymptomatic smokers by HRCT with normal spirometry and chest radiography.
Objectives
The main objectives of this study were as follows:
To establish HRCT as a diagnostic modality. To detect emphysema at its early stage of development in asymptomatic current smokers. To correlate the severity of emphysematous changes with the duration of smoking and the number of pack-years.
Materials and Methods
Study Design
Hospital-based observational cross-sectional study.
Study Duration
Six months, from August 2024 to February 2025.
Sample Size
Fifty (consecutive sampling method).
Study Place
Department of Pulmonary Medicine, Government Hospital for Chest and Communicable Diseases, Andhra Medical College, Visakhapatnam.
Inclusion Criteria
Current smokers without symptoms, individuals who have smoked at least five cigarettes a day for more than 5 years and have normal spirometry results.
Different forms of tobacco smoking, such as cigarettes, beedis and chuttas.
Smokers aged 25–50 years.
Exclusion Criteria
Obvious evidence of emphysema or any pulmonary disorder on standard chest radiography.
Previous history of recurrent respiratory tract infections.
Known asthmatics.
Patients on steroid or bronchodilator therapy.
Presence of skeletal abnormalities of the vertebral column, such as kyphosis, scoliosis, etc.
Coexistent cardiac, endocrine or renal disease.
Any patients who, in addition to air trapping, show other features of interstitial lung diseases or small airway diseases.
All patients with suspected HRCT findings indicative of bronchiolitis were excluded.
Methodology
A detailed questionnaire addressing the symptoms of chronic obstructive airway disease and associated conditions was completed by all participants, followed by a thorough clinical evaluation. Informed consent was obtained from all participants prior to conducting any investigations.
The participants were subjected to the following diagnostic procedures:
Routine frontal and left lateral chest X-rays were taken and assessed for indications of emphysema and other abnormalities. Pulmonary function assessments, such as forced vital capacity (FVC), FEV1, FEV1/FVC ratio, forced expiratory flow at 25% and 75% of forced vital capacity and peak expiratory flow rate, were carried out using the Vitalograph Alpha device. According to the 2024 GOLD guidelines, emphysema is functionally defined as having an FEV1 below 80% of the predicted value and/or an FEV1/FVC ratio below 70%. Participants with FVC or FEV1 values below 80% were excluded from the study. HRCT scans will be performed, capturing 1-mm-thick sections at 2-mm collimation intervals from the apex to the base of the lungs. The images were obtained at full inhalation while the subjects were lying on their backs. Expiratory imaging was performed at three anatomical levels: the aortic arch, the carina and the bases of the lungs. Two independent observers evaluated the chest X-rays and CT images.
The images were examined using a window level between −600 and −700 HU and a window width ranging from 1,500 to 1,700 HU. The region of the lung above the carina was designated as the upper zone, while the area below the carina was considered the lower zone. Emphysema was diagnosed based on specific criteria on CT scan described by Remy-Jardin et al.[8] and Çolak et al.[5] which were utilised in the present study.
Results
Sex Distribution
All 50 participants in the study were male; no female participants were included.
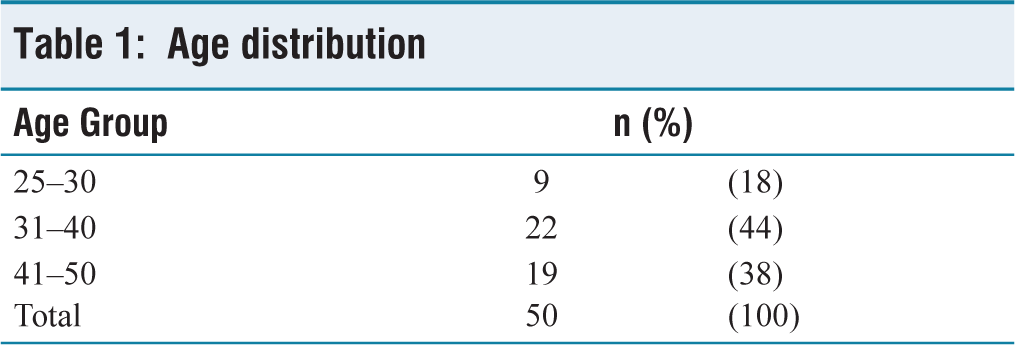
Distribution of Age
The participants had an average age of 38.41 years, ranging from 27 to 50 years. Table 1 displays the age distribution of the study subjects.
Age distribution
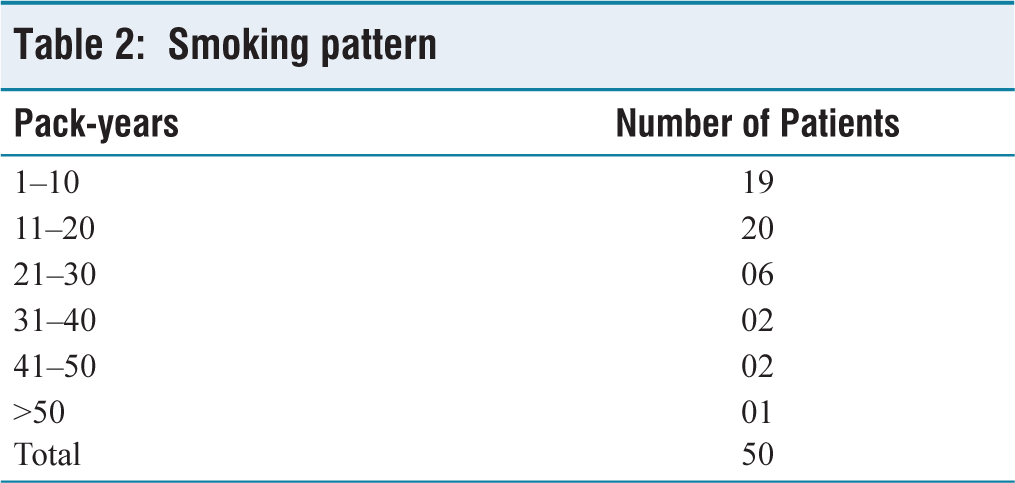
Smoking Pattern
The smoking pattern among the participants included in the study is summarised in Table 2. Pack-years were calculated from the number of packs of cigarettes or beedis smoked per day multiplied by the number of years of smoking.
Smoking pattern
Pulmonary Function Tests
All participants in the study exhibited normal values for FVC, FEV1 and the FEV1/FVC ratio, indicating overall normal spirometry across the group.
CT Findings
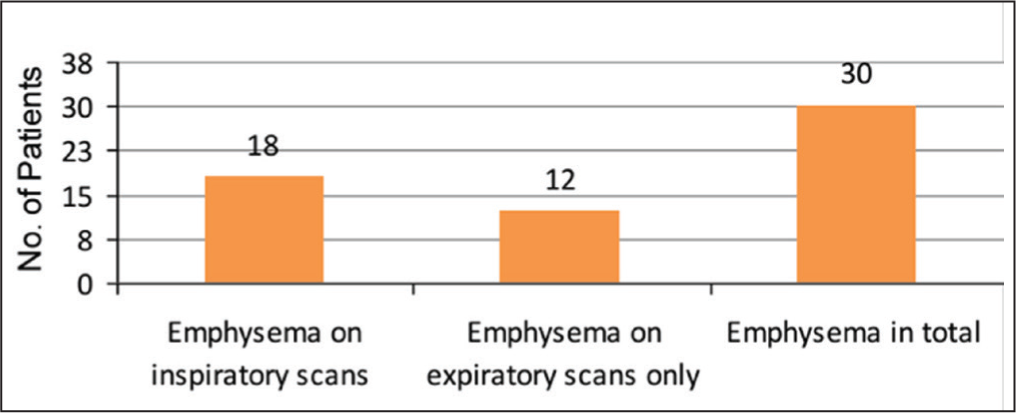
Out of 50 subjects, 30 (60%) showed CT evidence of emphysema. Among these 30 cases, 12 displayed signs of air trapping exclusively on expiratory scans, with their inspiratory HRCT scans appearing normal. In contrast, 20 individuals (40%) showed no signs of emphysema on either inspiratory or expiratory HRCT scans [see Figure 1]. The occurrence of emphysema was found to increase with age and the number of pack-years. The youngest patient diagnosed with emphysema was 33 years old, and no cases were identified in individuals younger than 30. A significant proportion of those with a smoking history exceeding 10 pack-years showed evidence of emphysema.
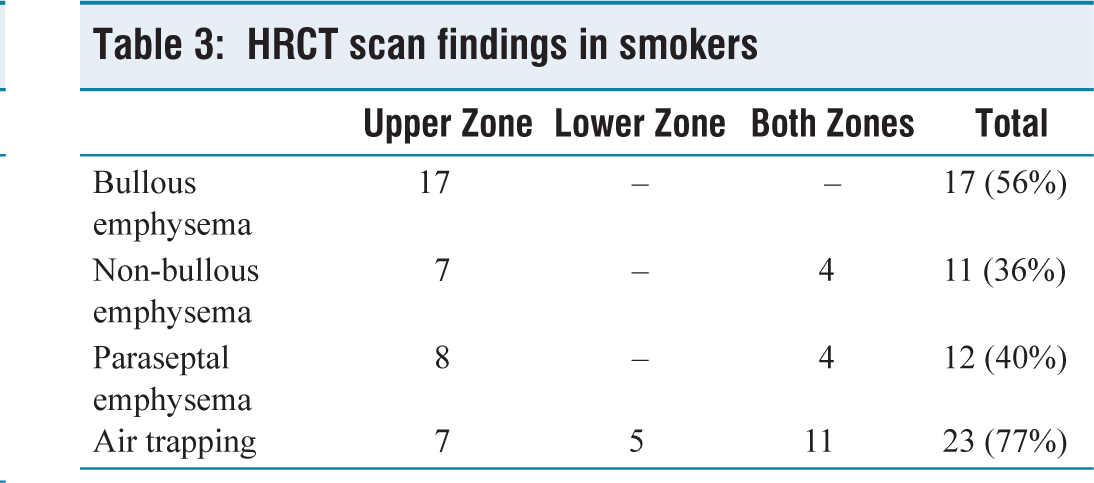
Air trapping was more commonly observed in individuals with a smoking history exceeding 10 pack-years. However, those with a smoking history of over 30 pack-years did not exhibit air trapping on expiratory CT scans. The most frequently noted HRCT finding was air trapping (77%), followed by bullous emphysema (56%), as detailed in Table 3.
HRCT scan findings in smokers
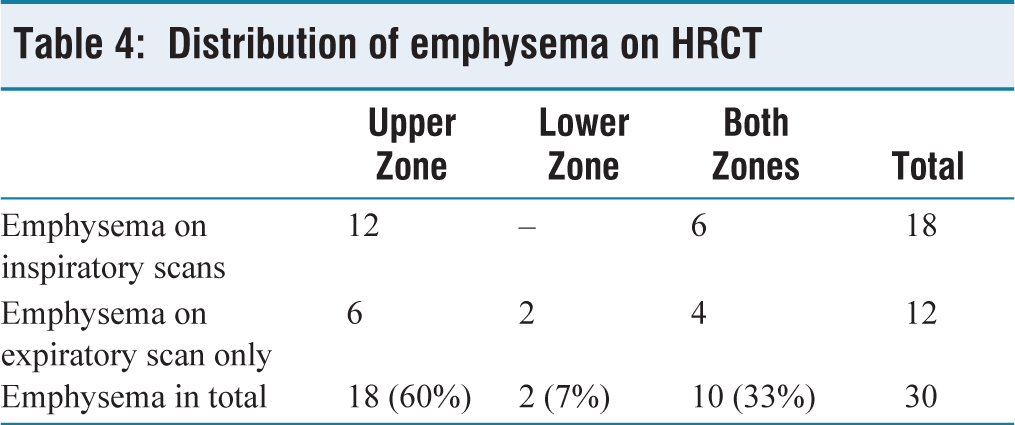
Emphysematous changes were distributed in both zones in 10 patients (33%), while in 18 patients, it was seen in the upper lung zones (60%). Lower zone predominance was seen in only two patients (7%) [see Table 4].
Distribution of emphysema on HRCT
Discussion
This study aimed to evaluate emphysema in 50 asymptomatic current smokers using HRCT. The mean age of participants was 38.4 years. The study revealed that 60% (30 out of 50) of subjects had emphysema, with air trapping (77%) being the most commonly observed finding. Other emphysematous changes included bullous emphysema in 56%, paraseptal emphysema in 40% and non-bullous emphysema in 36%. The study found a positive association between emphysema and age, as well as pack-years.
When compared to other studies, the findings of this study were consistent in several areas but showed some differences. In the study by Gurney et al., emphysema was detected in 61% of the patients, a rate comparable to the 60% found in the current study, while Remy-Jardin et al. found a much lower rate of 20%.[9,10] Air trapping was significantly higher in this study (77%) compared to the study by Gurney et al. (33%), emphasising the importance of air trapping as a key radiological feature for early emphysema detection. The use of expiratory scans played a crucial role in identifying additional cases, with 24% of patients showing emphysema that was missed in inspiratory scans alone.
Zonal distribution of emphysema showed upper zone predominance in 60% of cases, which is consistent with the study by Gurney et al. (58%), but higher than that reported by Sashidhar et al. (48%) and lower than that reported by Remy-Jardin et al. (65%).[11] The study also observed no significant difference in emphysema occurrence between cigarette smokers and those using other forms of tobacco, such as beedis or cigars, suggesting that smoking type might not influence emphysema development significantly.
The study had several limitations, including a small sample size of 50 subjects, the absence of pathological correlation, and reliance on subjective HRCT interpretation. Additionally, the study did not conduct objective quantification of emphysematous or include long-term follow-up to assess disease progression. Despite these limitations, the study highlighted the utility of HRCT, particularly with expiratory scans, in detecting early emphysema changes in asymptomatic smokers. Furthermore, the study underscored the significance of air trapping as an early marker of emphysema in smokers, which has not always been fully considered in previous studies.
Overall, the study contributes valuable insights into the early detection of emphysema in smokers, showing that HRCT has an important role in identifying changes before symptoms develop. Future studies with larger sample sizes, pathological correlation and objective quantification could further validate these findings and improve our understanding of emphysema in asymptomatic smokers.
Conclusion
Smoking is a key risk factor for the development of emphysema. Detecting emphysema early in smokers through non-invasive techniques could help slow the usual progression of the disease. This study included 50 asymptomatic smokers, and HRCT scans revealed emphysematous changes in 30 of them. These 30 individuals represent a high-risk group who may develop more severe symptoms in the future.
Supplemental material
Supplemental material for this article available online.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
IEC No.: 230/IEC AMC/AUG 2024.
Informed consent
Informed consent was obtained from all participants.
Credit author statement
D.V. Pratapa Reddy: Conceptualisation, methodology, investigation and writing.
V. Vijayakumari: Validation and supervision.
B.M.S. Patrudu: Supervision and project administration
R. Sunil Kumar: Supervision and project administration.
CH.R.N. Bhushana Rao: Supervision and project administration.
Aardra Dutt: Data curation, writing and visualisation.
Data availability
Non-digital data were curated at the Department of Pulmonary Medicine, Andhra Medical College, Visakhapatnam.
Use of artificial intelligence
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.