
Abstract
Background and Aims:
Postoperative pulmonary complications (PPC) pose significant problems, especially in patients with chronic obstructive pulmonary disease (COPD). We aimed to assess the risk of developing PPC in COPD patients undergoing non-thoracic surgeries along with its correlation to the type of surgery, anaesthesia technique and patient-related factors.
Material and Methods:
We prospectively collected data such as the comorbidities, preoperative pulmonary risk scores, recent history of respiratory infection, investigations, surgical (type, duration, surgical urgency and site) and anaesthesia data (general or regional, airway intervention if any), American Society of Anaesthesiologists (ASA) scores, the Assess Respiratory Risk in Surgical Patients in Catalonia (ARISCAT) risk index scores and Global Initiative for Chronic Obstructive Lung Diseases (GOLD) classification of COPD in 196 patients. We tried to find a correlation between these factors to the development of PPC.
Results:
The risk of PPC in patients with an ASA category 3 was 3.24 times higher than in those with an ASA 2. It was 1.22 times higher in patients with COPD classified as GOLD criteria 3 compared with those classified as GOLD criteria 1 and 2. PPC in high-risk ARISCAT scores was 4.97 times higher than in patients with intermediate to low-risk ARISCAT scores. The risk factors which had a significant association with PPC were patients more than 65 years of age, patients with metabolic equivalent (MET) score less than 4, respiratory infection in the last 1 month, haemoglobin less than 10 gm/dl, pre-operative oxygen saturation (SpO2) less than 95% on room air, administration of general anaesthesia over regional anaesthesia, emergency surgery and surgical time more than 3 hours.
Conclusion:
ASA classification and GOLD criteria are useful to assess preoperative health status and the severity of COPD and reasonably predict the risk of PPC. The ARISCAT risk index, however, is a stronger modality to predict PPC.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a preventable and curable disease which is characterised by progressive airflow obstruction that includes smaller airway inflammation (obstructive bronchiolitis) and parenchymal destruction (emphysema) caused by significant exposure to noxious particles or gases. It should be considered in a patient who has persistent dyspnoea, chronic intermittent cough and recurrent wheeze, chronic sputum production, recurrent lower respiratory tract infection, exposure to risk factors and family history. Furthermore, in the presence of a bronchodilator, the ratio of the forced expiratory volume in 1 second (FEV1) to the forced vital capacity (FVC) of the lungs (FEV1/FVC) < 0.70 confirms the diagnosis.[1]
Pre-operative risk stratification in COPD patients can be done by various modalities.
The American Society of Anaesthesiologists (ASA) physical status classification predicts perioperative risk[2] and is a useful, widely accepted tool for predicting postoperative pulmonary complications (PPC).[3]
The modified British Medical Research Council (mMRC) dyspnoea scale is used for the assessment of breathlessness that anticipates future mortality risk.[1] It is divided into 5 grades, from grade 0 being breathlessness with strenuous exercise to grade 4, where breathlessness occurs at rest.
The Global Initiative for Chronic Obstructive Lung Diseases (GOLD) criteria[1] determine the severity of airflow limitation, which has 4 grades based on FEV1. The grades are mild (FEV1 ≥80% predicted), moderate (50% ≤ FEV1 <80% predicted), severe (30% ≤ FEV1 <50%) and very severe (FEV1<30%).
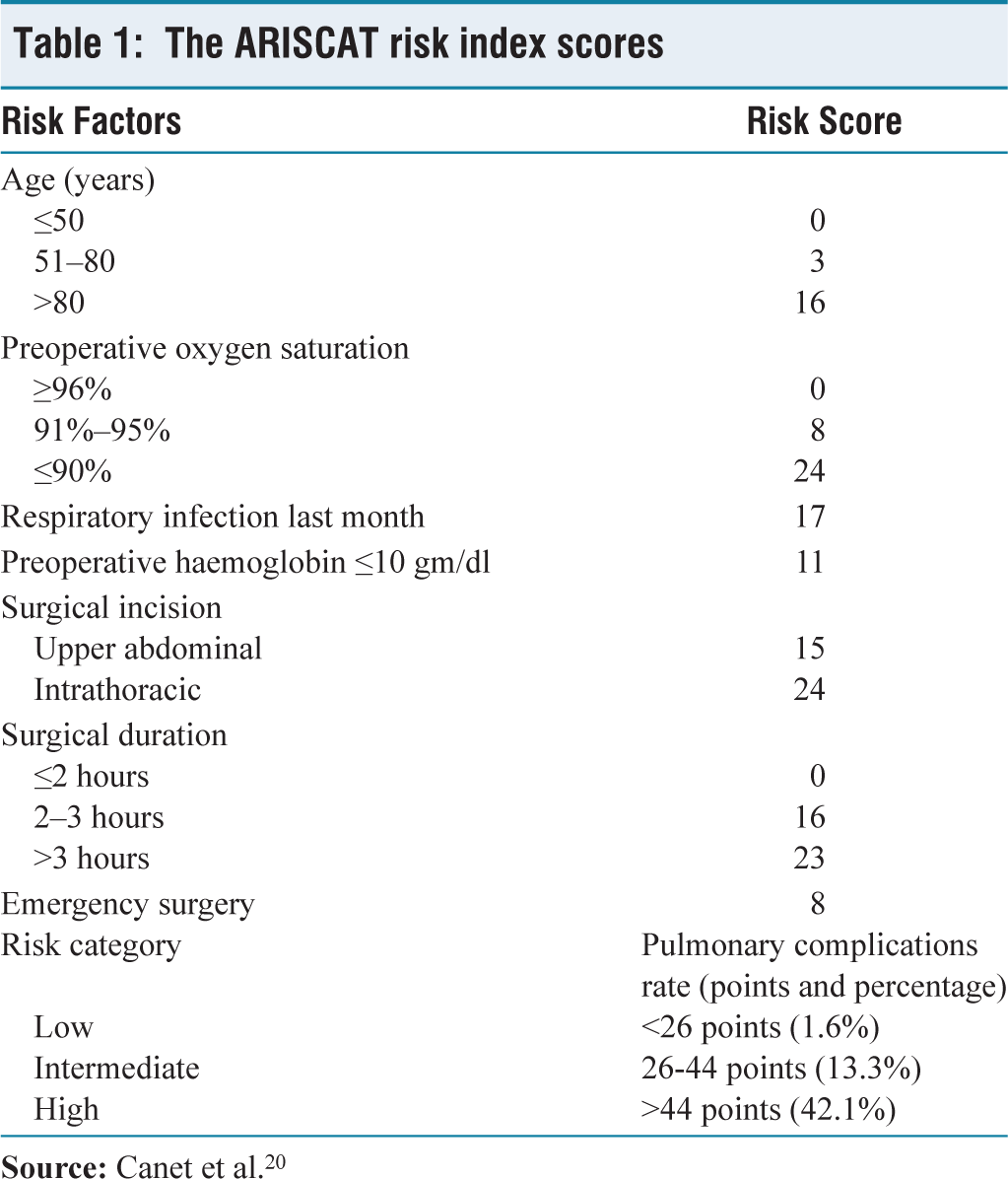
The Assess Respiratory Risk in Surgical Patients in Catalonia (ARISCAT)[4] risk index is another scoring method to evaluate the likelihood of developing PPC using 7 factors, which include age, SpO2 on room air, respiratory infection in the previous month, haemoglobin level, type and duration of surgery and emergency or elective surgery [Table 1].
The ARISCAT risk index scores
Despite advances in anaesthesia and surgical management, PPC still poses considerable problems in clinical practice. Postoperative respiratory failure is the most common form of PPC and the incidence of PPC in major surgeries can be as high as 23%. Length of hospital stay (LOS) has been shown to be prolonged by 13–17 days.[5]
Patients with suspected or known pulmonary diseases should have a careful pre-operative evaluation. Positive pressure ventilation, patient positioning and drugs used during general anaesthesia can alter pulmonary status. Robust models of pulmonary risk stratification[6] to predict PPC are yet to be used widely. There is also no consensus on the measures that can be employed to mitigate the risks of the development of PPC in patients who may be at risk.[7]
Evaluation of risk factors for the development of PPC in patients with COPD has been done globally by the Global Initiative for Asthma and GOLD criteria. The ARISCAT score as a risk prediction model for predicting PPC has been studied in India as well. However, not many investigators have tried to compare ASA PS categories, GOLD criteria and ARISCAT together in the same cohort to predict PPC.
We aimed to predict postoperative outcomes in COPD patients in a tertiary care hospital by preoperative risk stratification using ASA classification, ARISCAT score and GOLD criteria in patients undergoing non-thoracic surgery.
Material and Methods
This time-framed prospective observational study, conducted in a tertiary care centre from November 2020 to November 2021 (duration of 1 year), was approved by the institute ethics committee (IEC/2020/DNB/11/32, 21 November 2020).
Patients above 18 years of age of both genders who were chronic smokers and patients having a history of cough, expectoration and shortness of breath, undergoing elective and emergency non-thoracic surgical procedures with general, neuraxial or regional anaesthesia were included in the study.
Patients who could not perform the spirometry test or had any recent history of cardiac, cerebral, pulmonary or thoracic ailments were not enrolled.
The primary objective of our study was to assess the risk of developing PPC, its incidence and severity in COPD patients undergoing non-thoracic surgeries. We also assessed the correlation of other associated factors, such as the type of surgery and anaesthesia, along with other patient factors, in developing PPC. The study population was 196.
The formula used for the calculation of sample size was:
[where n = Sample size
z = The standard normal deviate, which is 1.96 at a 95% confidence interval
p = Prevalence in the population of the factor under study]
Here p = 15% = 0.15 (from a previous study[8])
q = 1−p = 0.85
d = Absolute precision

We prospectively reviewed the patient’s demographic data, comorbidities, preoperative pulmonary risk score, history of respiratory tract infection within 1 month before surgery, laboratory results, surgical data (type, duration, surgical urgency and site), anaesthesia-related data (general or regional, airway intervention if any), ASA scores, ARISCAT scores and GOLD classification of COPD. The type of surgery was classified into high-risk (cavity surgery) and low-risk (surface surgery).
PPC was defined by the presence of any 3 of the following 4 criteria, which included fever with temperature >38.0°C postoperatively, leucocytosis with white blood cell count > 12 × 109/L, lung consolidation or increasing patchy opacity on chest imaging and purulent sputum or positive sputum culture.[9]
We also looked for objective findings like respiratory rate >20/min, SpO2, auscultatory findings, chest X-ray, arterial blood gases (ABGs), LOS, intensive care unit (ICU) stay and oxygen requirement in the postoperative period (nasal cannula, face-mask, high flow nasal cannula, non-invasive ventilation or invasive ventilation).
Oxygen was not routinely prescribed to all patients in the postoperative period.
Oxygen was administered when SpO2 was less than 90% on room air.
Abnormal ABGs were described by the presence of postoperative partial pressure of oxygen (PaO2) <60mmHg on room air and the ratio of PaO2 to inspired oxygen fraction <300 mmHg.
Statistical analysis was performed with the help of Epi InfoTM 7.2.2.2 (trademark of the Centres for Disease Control and Prevention).
Descriptive statistical analysis was performed to calculate the means with corresponding standard deviations. A test of proportion was used to find the standard normal deviate (Z) to compare the different proportions and a chi-square (χ²) test was performed to find the associations. P < .05 was taken to be statistically significant.
Results
The risk of PPC in patients aged greater than 65 years was 2.36 times higher than that of patients aged less than 65 years (Odds ratio [OR]-2.36 [1.33, 4.20]; P = .0031). The risk of PPC among the patients with a metabolic equivalent (MET) score less than 4 was 2.02 times more than those who had scores less than 4 (OR-2.02 [1.12, 3.66]; P = .0187).
In our cohort, we had more obese patients (87.2%) than those with normal body mass index (12.8%) (Z = 10.46; P < .0001). Most of our patients had a low-risk of obstructive sleep apnoea (OSA) (Z = 11.87; P < .0001). However, there was a remarkable association of OSA with post-operative oxygen requirements and abnormal ABGs.
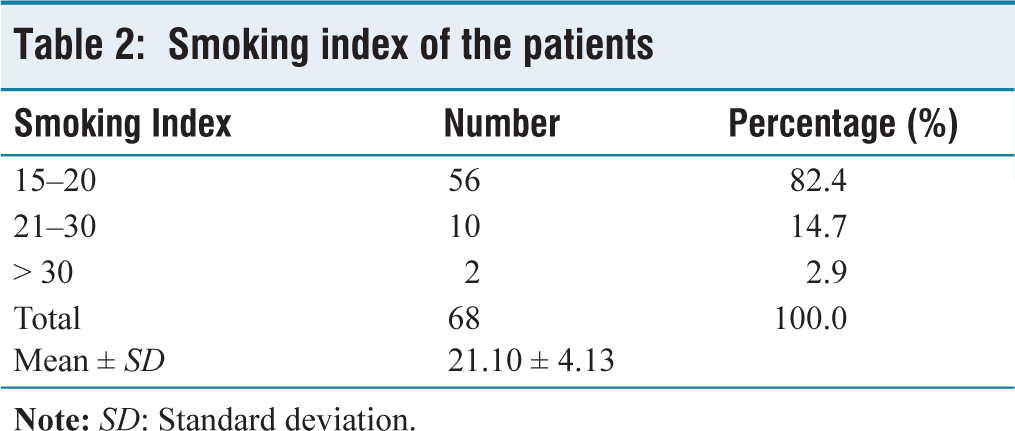
About 34.7% of the patients were smokers (Z = 6.51; P < .0001). The smoking index (cigarettes smoked per day multiplied by the smoking time in years divided by 20) of 82.4% of the patients was between 15–20, which was considerably high (Z = 9.47; P < .0001) [Table 2].
Smoking index of the patients
Around 62.2% of the patients had an mMRC score 1 (Z = 3.96; P < .0001).
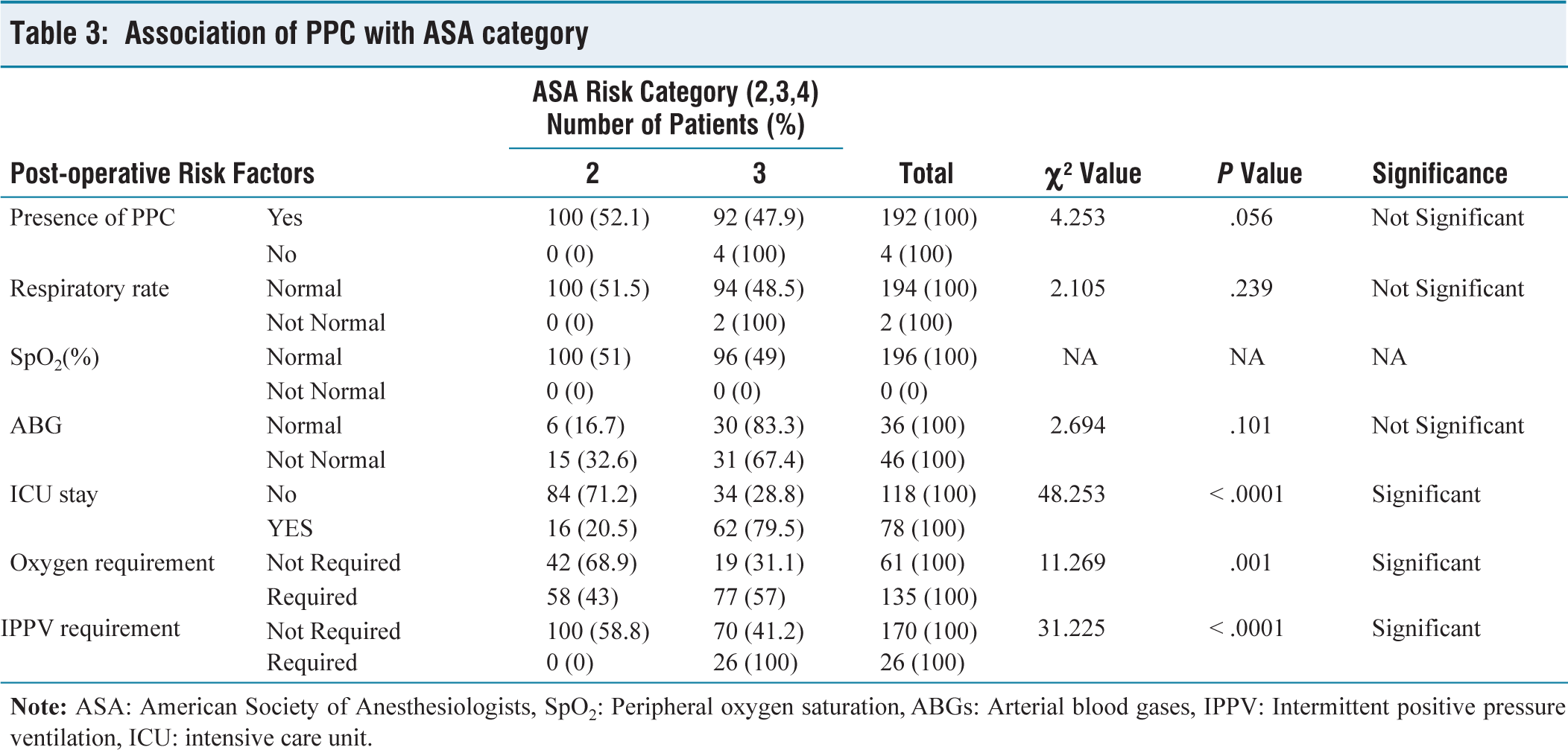
Patients with ASA risk category 3 had 3.24 times more risk of developing PPC than those with ASA risk category 2 (OR-3.24 [1.80, 5.83]; P < .0001) [Table 3].
Association of PPC with ASA category
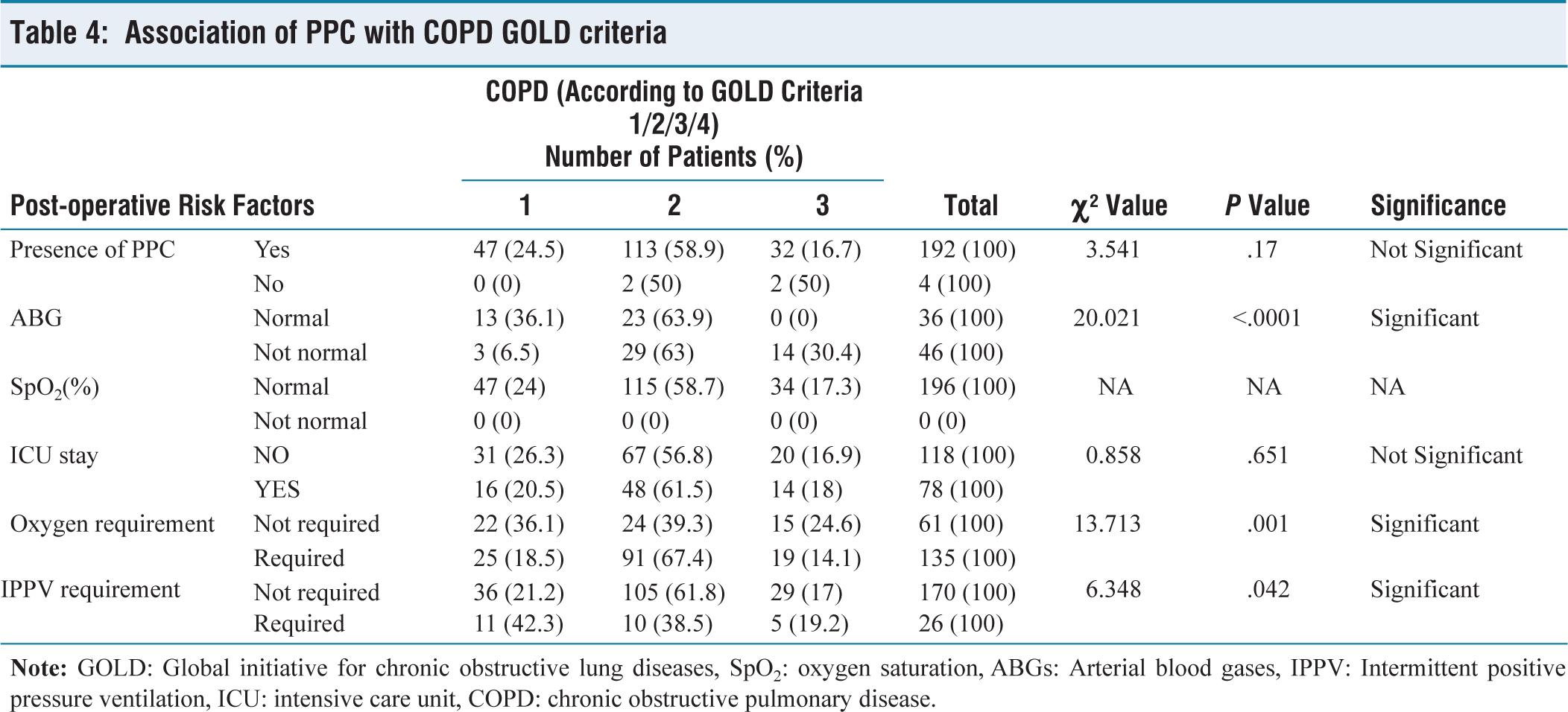
The majority of our patients (58.7%) belonged to GOLD criteria grade 2 COPD (Z = 5.02; P < .001). Risk of PPC amongst the patients with COPD GOLD criteria 3 was 1.22 times more than in patients with COPD GOLD criteria 1 and 2. The risk association was not significant (OR-1.22 [0.58, 2.55]; P = .59) [Table 4].
Association of PPC with COPD GOLD criteria
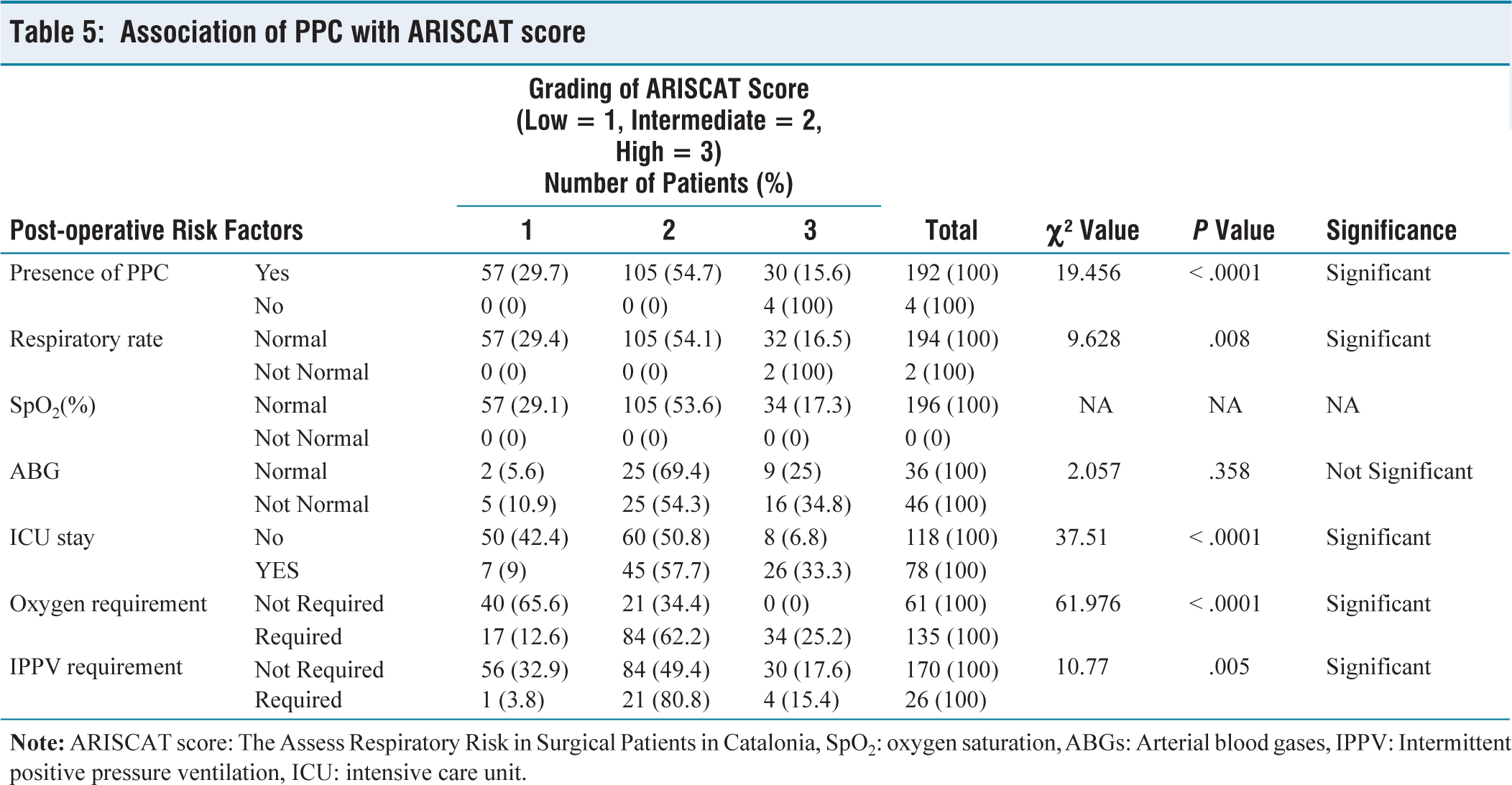
In our study population, most of our patients (53.6%) had an intermediate ARISCAT risk index score (Z = 3.58; P < .001). The risk of PPC among the patients with high-risk ARISCAT scores was 4.97 times higher than those with intermediate to low-risk ARISCAT scores. The risk of association was very significant (OR-4.97 [2.12, 11.67]; P < .0001) [Table 5].
Association of PPC with ARISCAT score
The risk of PPC among patients with a history of respiratory infection in the last 1 month was 13.12 times higher than those without such an affliction (OR-13.12 [1.64, 104.65]; P = .002). Haemoglobin level was greater than 10 gm/dl in 69.9% of the patients (Z = 5.65; P < .0001). There was a significant association between pre-operative level of haemoglobin and PPC (P = .013). Around 70.4% of the patients had SpO2 ≥ 95% on room air (Z = 5.65; P < .0001). The risk of PPC among the patients with SpO2 ≤ 95% on room air was 1.53 times higher than those who had higher values (OR-1.53 [0.83, 2.84]; P = .17).
Nearly 80.6% of the patients had normal respiratory rate (Z = 8.76; P < .0001) and normal breath-holding time was noted in 54.6% of the patients (Z = 8.76; P < .0001).
On auscultation, in 80.6% of the cases, no added sound was observed (Z = 8.76; P < .0001).
In the chest radiogram, the majority of the patients had increased broncho-vascular markings (65.8 %) (Z = 8.15; P < .0001). However, the post-operative chest radiogram was normal in 90.8% of the patients (Z = 11.59; P < .0001).
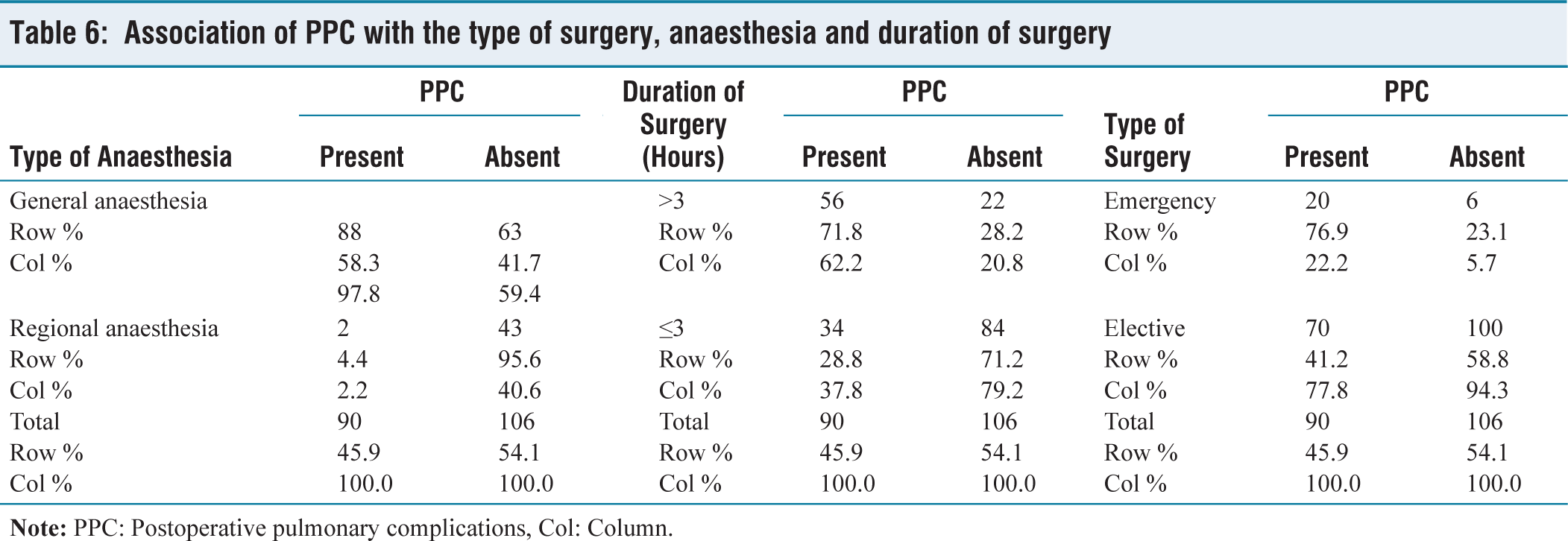
Elective surgeries (86.7%) were more than emergency surgeries (13.3%) (Z = 10.46; P < .0001). The risk of PPC in emergency surgeries was 4.76 times higher than in elective surgeries. This association too was significant (OR-4.76 [1.81, 12.46]; P < .0001).
The risk of PPCs where the surgical duration was more than 3 hours was 6.28 times more than in (OR-6.28 [3.33, 11.85]; P < .0001). General anaesthesia was administered in 77.0% of the patients (Z = 7.63; P < .0001) and the risk of PPC after general anaesthesia was 30.03 times more than that of the patients who underwent a procedure under regional anaesthesia. This association risk too was significant (OR-30.03 [7.01, 128.57]; P < .0001) [Table 6].
Association of PPC with the type of surgery, anaesthesia and duration of surgery
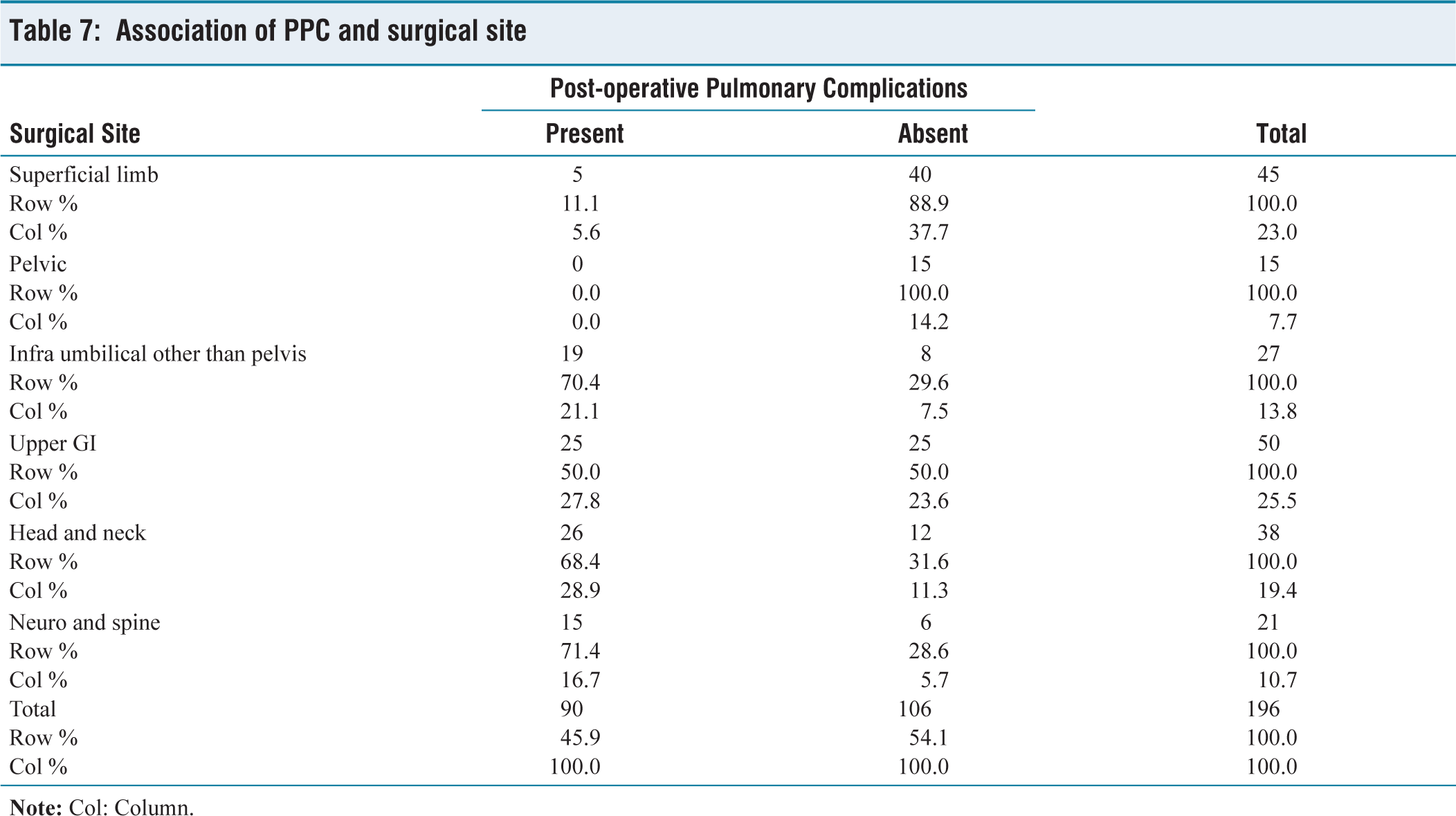
χ² test showed that there was a significant association between the surgical site and PPC (P < .0001) [Table 7].
Association of PPC and surgical site
In the postoperative period, oxygen requirement was observed in 68.9% of the patients (Z = 5.37; P <.0001) and 13.2% required intermittent positive pressure ventilation. ICU admission was not required in 60.2% of the cases (Z = 2.82; P = .0046). Overall, 71.4% of the patients were discharged within 7 days (Z = 5.93; P < .0001).
Discussion
Multiple studies have previously illustrated an association of ASA classification with PPC. The American College of Physicians has revealed that a higher ASA classification is associated with a substantial increase in the chance of pulmonary complications. Hall and colleagues[10] found that the ASA classification was the single-most important variable predictive of the development of PPC. Fernandez-Bustamante[11] et al. concluded that PPC is common in patients with an ASA PS 3 category. In our study, we observed that the proportion of patients with PPC was significantly higher among the patients with ASA risk category 3 (64.4%) as compared to the patients with ASA risk category 2 (35.6%).
The severity of COPD plays a part in the development of PPC. Kim[12] et al. concluded that GOLD groups C and D were significantly associated with postoperative complications. Jiao[13] et al. noticed that severe COPD (FEV1<50% predicted) was associated with more PPCs than moderate (FEV1 50%–80% predicted) and mild grade (FEV1 ≥80% predicted). In our study, we found that the risk of PPC among the patients with COPD GOLD criteria 3 was 1.22 times higher than that of the patients with COPD GOLD criteria 1 and 2.
The ARISCAT risk score index is a good tool for predicting PPC. Mazo[14] et al. externally validated the ARISCAT score for predicting PPCs. A study by Kara[15] et al. revealed that the ARISCAT score was a better modality than the ASA classification for predicting PPCs. In our observation, there was a significant association between ARISCAT score and PPC and the risk among the patients with high-risk ARISCAT score was 4.97 times more than that of the patients with intermediate to low-risk ARISCAT score.
Multiple factors besides the severity of COPD are associated with PPC. Smetana and colleagues[16] have mentioned multiple patient-related factors, procedure-related factors and investigations in their study. Verma[17] et al. revealed that the incidence of PPCs was higher in emergency abdominal surgeries. Kumar[18] et al. found a significant association between emergent surgery and increasing age with the incidence of PPCs. In our study, the risk of PPC among patients with emergency surgery was found to be 4.76 times higher than in patients undergoing elective surgery.
Taylor[19] et al. mentioned ASA 2 or greater, limited functional status, old age, anaemia, preoperative lower SpO2, respiratory infection within 1 month, surgical incision near the diaphragm, longer duration of surgery and emergency surgery as risk factors for developing PPC. Canet[20] et al. mentioned 7 independent risk factors for developing PPC. In our study, the risk of developing PPC among patients older than 65 years was 2.36 times more than those who were younger. The risk of PPC among the patients with a MET score less than 4 was 2.02 times higher than those who had higher scores. The risk of PPC among patients with respiratory infection in the last 1 month was 13.12 times higher than those who did not have such a recent problem. The occurrence of PPC among the patients with a lower level of haemoglobin (<10 gm/dl) was 2.17 times more than in patients with a higher haemoglobin level. The development of PPC among the patients with pre-operative low SpO2 (below 95%) was 1.53 times higher than those with higher SpO2 values.
Jammer[21] et al. concluded that if the duration of surgery is less than 3 hours and when regional anaesthesia techniques were used, the incidence of PPC was lower. In our study, we found that the risk of PPC among the patients who underwent general anaesthesia was 30.03 times higher than that in the patients who received regional anaesthesia. There was a significant association between the surgical site and the duration of surgery with PPC.
Conclusion
The occurrence of PPC not only depends upon the severity of COPD, but is also associated with patient factors, surgery and the anaesthesia technique. ASA classification is commonly used to assess the preoperative physical status and GOLD criteria help in assessing the severity of COPD and they too can predict the development of PPC. We found that the ARISCAT risk score index is a stronger predictor of PPC. We suggest that the incorporation of this may improve the ability to predict PPC in patients with COPD undergoing non-thoracic surgeries.
Footnotes
Acknowledgements
We thank Dr Suresh Ramasubban, Chief of Critical Care and Pulmonary and Sleep Medicine.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Institutional Ethics Committee Apollo Gleneagles Hospitals, Kolkata IEC/2020/DNB/11/32.
Informed consent
The consent waiver was provided by the institute’s ethics committee.
Patient consent
The consent waiver was provided by the institute’s ethics committee.
Credit author statement
All five authors were associated with conception and design of the study, acquisition of data and its analysis and interpretation of data. They have all been responsible for drafting the article and revising it critically for important intellectual content. Final approval of the version to be published has been ratified by all five authors.
Data availability
Not applicable.
Use of artificial intelligence
No.
Manuscript presentation
None.
Registration no. of clinical trial
Not registered.