
Abstract
Objectives:
Effective, high-quality communication remains a cornerstone in the management of diabetes mellitus (DM). This review addresses how effective communication is crucial in navigating patients’ changing demands over time and how diabetes-specific communication can address the unique facets of patient-provider interactions and improve the long-term outcome of the disease. There is also emphasis on the importance of re-evaluating the way we discuss diabetes and the much-needed integration of communication skills in the medical curriculum.
Methodology:
The literature and information regarding this topic were collected from different original articles, review articles, systematic reviews and meta-analysis available on various platforms such as Google Scholar and pubmed.
Results:
Current available literature reveals that effective communication between an individual with diabetes and their healthcare provider has a pivotal role in improving the quality of care and also in mitigating the incidence of diabetic complications. As bi-directional communication is often missed in a busy outpatient clinic, the unmet need for improving communication skills in healthcare providers right from the undergraduate medical curriculum has to be addressed by implementing systematic and cost-effective strategies.
Conclusion:
As the prevalence of diabetes is increasing in alarming trends, training medical students regarding communication skills, availing multidisciplinary teams at diabetic clinics and implementing cutting-edge technologies like artificial intelligence will be the way forward in the quality management of diabetes.
Introduction
Effective communication and engagement between the care seeker and their provider is a major factor influencing the quality of care and long term outcome in any chronic illness.[1] This especially holds true for individuals living with diabetes mellitus (DM), a chronic disease affecting around 537 million people worldwide, that warrants constant and complex self-management activities, including monitoring, follow-up, education, including behavioural adjustments to ensure better quality of life.[2-4] As it is a complex multisystemic disease, there is more to diabetes than just glycaemic control, amongst which psychosocial factors play a very significant role.[5] Hence, a clear and open type of communication between the healthcare provider and the care seeker is very crucial for holistic management of the disease. This article provides an overview of the importance of effective health communication, types of communication styles, interventions to improve communication skills, the unmet needs to be addressed in improving communication skills among health care professionals (HCPs) and the current literature available on communication in diabetes. This review concludes with a comprehensive summary regarding the future directions aimed at improving health communication.
Current Literature
In the context of DM, communication focused on the person with diabetes is associated with improved disease knowledge, self-care, quality of life and better measures of metabolic control.[6] Numerous studies have emphasised the significance of effective communication between the care seeker and the physician in promoting the individuals’ adherence to treatment decision and improving their self-management goals. Consistent with this evidence, leading organisations, including the American Diabetic Association and the International Diabetes Federation, currently advocate for better communication in the management of diabetes.[7,8] A multinational diabetes attitudes, wishes and needs study-DAWN, with data from around 13 countries concluded that individuals with diabetes encountered psychosocial issues, particularly diabetes-related worries and concerns that severely mitigated their self-management goals.[9] Despite various recommendations, the results from the DAWN2 study suggest that individual-centric care is often unavailable and that the psychosocial needs of people with diabetes worldwide are not being addressed. This study also highlighted the risk of depression, relationship issues, poor physical health and an overall impaired quality of life.[10] A position statement noted that appropriate use of words influenced people’s view on their diabetes and recommended the use of motivated collaborative language, and to avoid terms such as diabetic patient, kidney failure, poorly controlled, poor complaint, emphasising the need for a strength-based language approach, as opposed to the deficit-based approach.[11]
An Indian study[12] analysed the communication of physicians with their care seekers who were not adherent with their medications, focusing on ways to promote adherence in such individuals. Survey questions were used to examine the ways of communication with non-adherent individuals, examined attitudes towards common communication cues, and explored communication approaches to encourage diabetes adherence. Findings were interpreted on the basis of qualitative and quantitative findings. The quantitative findings showed that the majority of the physicians engaged in negative communication strategies (threatening words) to improve adherence. The qualitative findings revealed that they used paternalistic (authoritative, educational, authoritarian) approaches more than collaborative (multistakeholder, patient-centred) approaches with non-adherent individuals.
Another study[13] explored the possibilities of the constraining and facilitating factors to care seeker focused communication in individuals with diabetes and the providers who were involved in their treatment. People with diabetes focused on the relationship with their provider, while providers emphasised more on the constraining factors when exchanging information. Diabetic individuals perceived aggressive attitude as a barrier to communication but providers perceived it as a facilitator. Only providers mentioned the role of macro-level interventions and diabetic individuals’ socioeconomic position as essential factors.
These results underscore the importance of communication skill training programs for Indian physicians focusing on empathetic, supportive and inclusive techniques so as to promote individuals’ adherence with the additional use of role-playing, video recording and peer feedback methods.
Importance of Effective Communication in Diabetes
Medicine being both a science and an art, a delicate balancing of the scientific skills with the establishment of a good rapport and trust with each other is very crucial. Effective communication is fundamental in the management of diabetes due to several reasons:
Awareness and education Diabetes self-management often requires awareness about the natural history and disease course from the care seekers’ side. Studies conducted in South India have revealed a pervasive deficiency in knowledge and awareness about diabetes, with scores particularly lower among women and individuals with poor literacy.[14] Clear exchange of information helps individuals to understand the diagnosis, importance of lifestyle interventions, medication adherence and helps them to agree upon an action plan, empowering a better decision-making process. Provide individualised care As the needs of each individual vary, it is foremost to address their priorities, preferences and day-to-day challenges. Open communication and discussion enables the HCPs to individualise the diabetic management plan for a person based on their dietary preferences, lifestyle and other needs.[15] Address emotional needs/psychosocial concerns Managing life with diabetes can cause significant emotional distress. Emotional trauma related to living with diabetes is often not acknowledged by HCPs. Addressing the psychosocial aspects empowers them to build confidence and mitigate their fear and stress.[16,17] Empathetic communication and psychological support through active listening can help address stress, anxiety, and other emotional barriers.
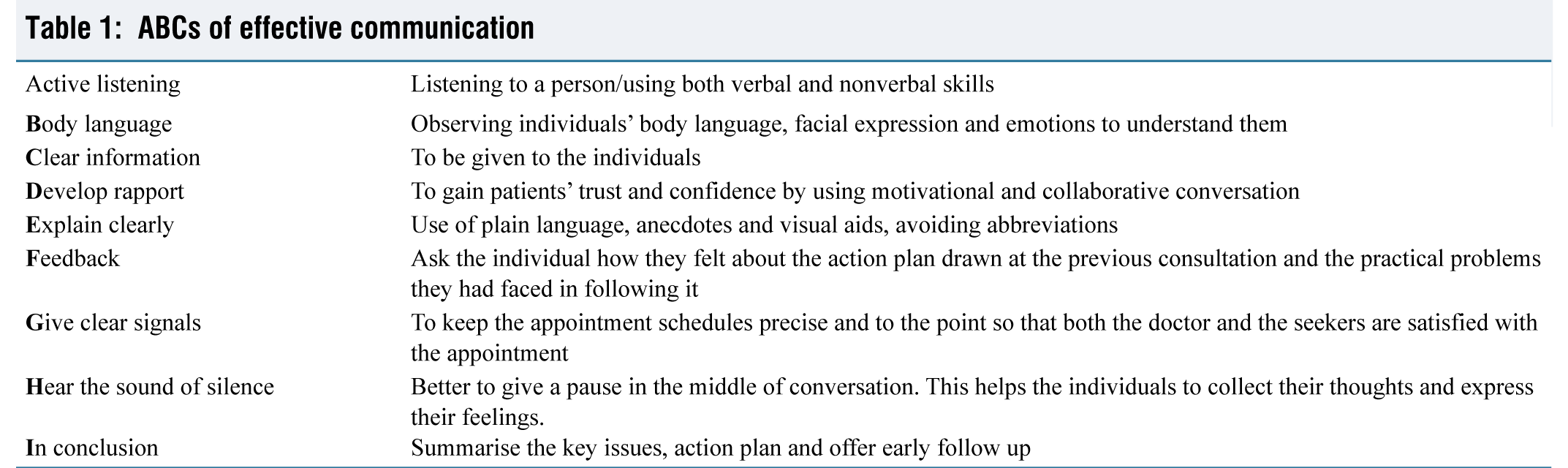
ABCS of effective communication
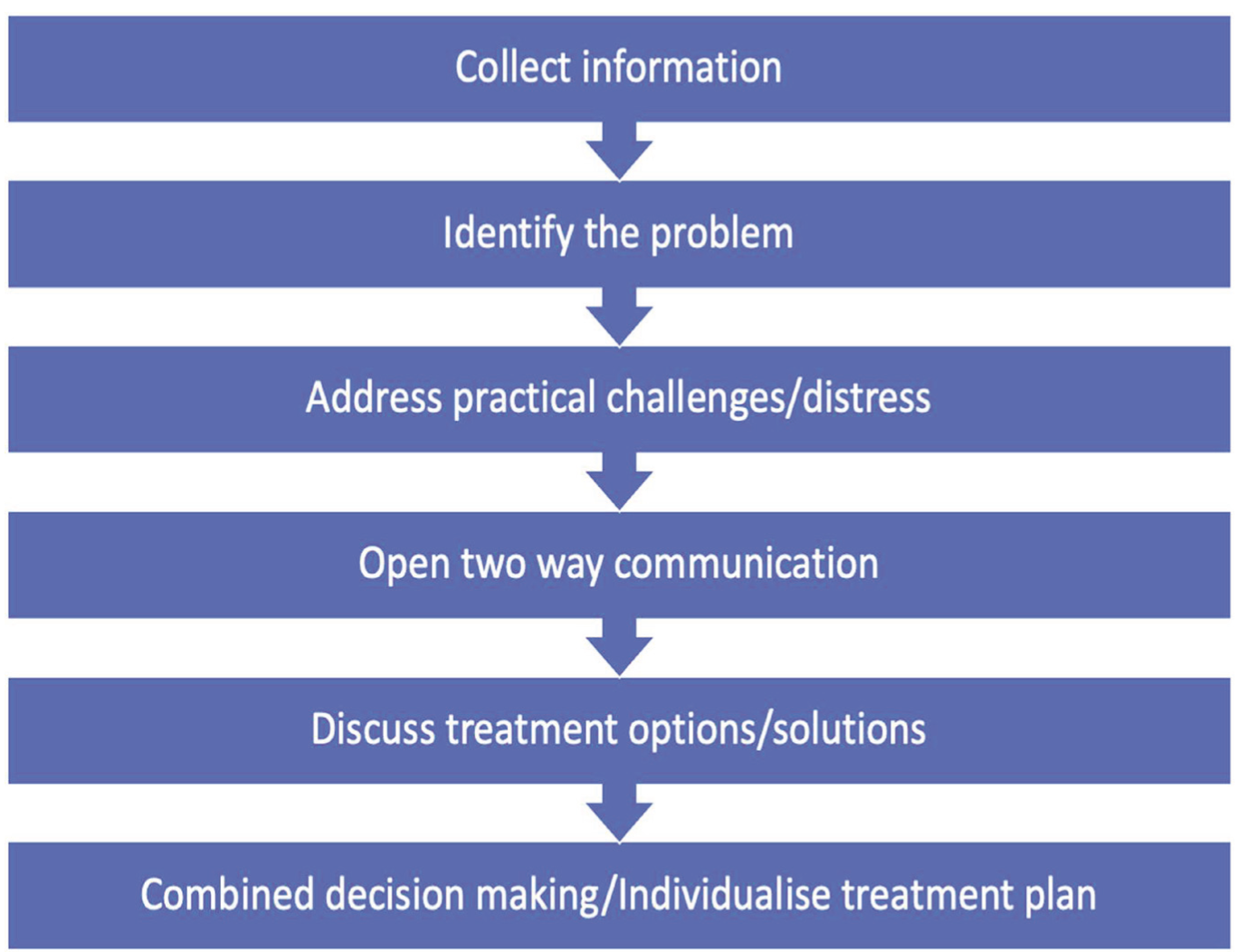
The general techniques for effective communication, though widely applicable, are not necessarily intuitive and hence it requires time and effort to integrate them in routine clinical practice [Table 1].[18] Below are certain ways that can be incorporated to improve the effectiveness of communication during the careseekers’ appointments with the HCPs.
Flow of effective communication
ABCs of effective communication
Facilitators of Effective Communication These include factors that strengthen or improve communication between an individual with diabetes and his provider.[19]
Provider relationship with careseeker
Provider accessibility: This refers to careseekers’ opportunities to follow up with their providers and to get engaged with them with questions or doubts in between their clinic visits. This can be carried out through various communication means such as telephoning, mailing, and direct messaging through online portals. Increasing partnership: Willingness to partner with the careseeker in the decision-making process in a supportive manner and allowing them to discuss their diabetes management more comfortably with providers is a major facilitating factor. Appropriate analogies: The entire team have to use the same language to build the careseekers’ confidence as they reinforce each other. Consistency has to be maintained throughout the process.
Disease and treatment-related behaviour
Provide practical, tailored information: Diabetic education programmes can improve their knowledge and provide a better understanding of their condition. Further, this also empowers them to discuss their disease management. Family support: Family members can help individuals with diabetes regarding meal-planning, medication reminders, glucose checking and engaging in exercise for self. Investing in diabetes educators: Well-trained diabetic educators play a crucial role in enhancing the quality of care in individuals with diabetes and ensure the efficient use of HCPs’ time and expertise Macrolevel interventions: Wider community networking has to be strengthened with adequate social support interventional programmes.
Barriers to Effective Communication
Constraining factors are broadly categorised on the basis of provider relationship with person seeking care, treatment-related behavioural aspects and information exchange process [Table 2].[19]
Barriers to communication and strategies to overcome
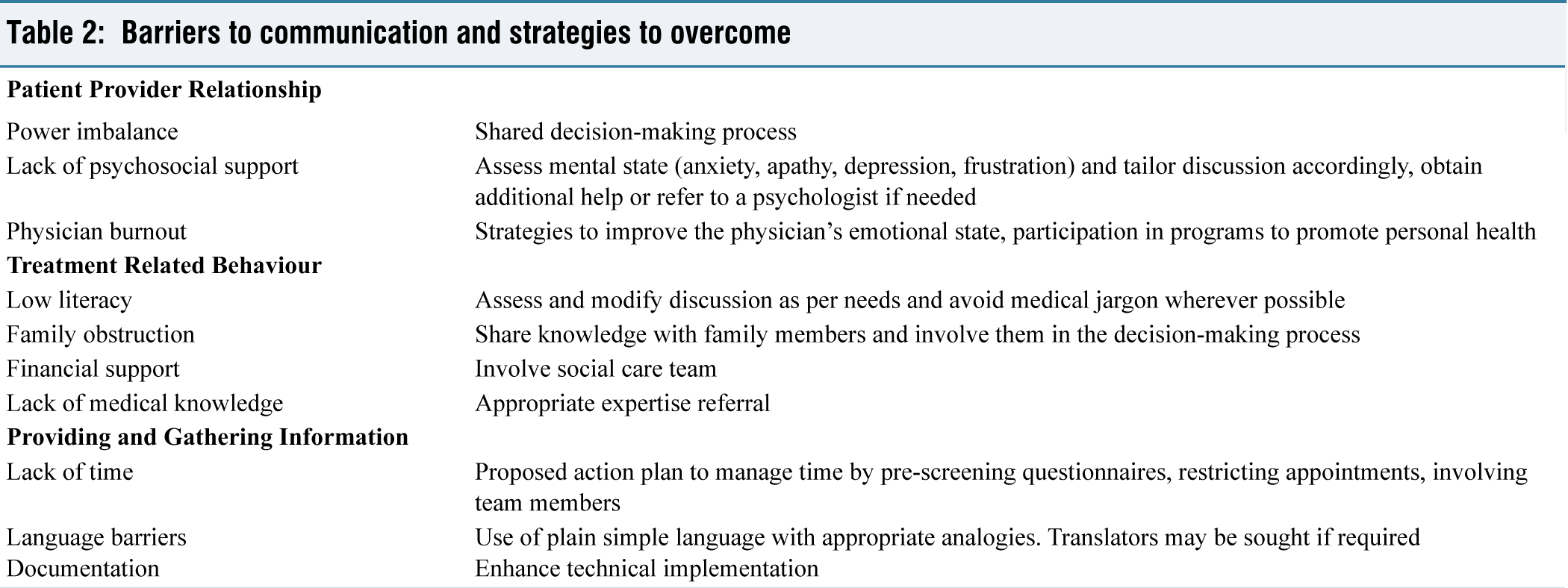
The first barrier identified was ‘Diabetic individuals’ Lack of Preparation for Appointments’. Specifically, participants mentioned that their clinic visits with providers are not as productive when they would forget to ask questions or bring their recent glucose logs, etc. Another participant described how the length of time between appointments can make it difficult to remember questions or challenges that they should discuss with their provider. Another barrier to communication that was identified in the analysis was ‘Providers’ Focusing on “Numbers” Rather than their Concerns’. This theme was described by participants as a major barrier to communication. Specifically, participants described communication difficulties if they felt that their providers were only concerned about their HbA1c, weight, etc. (i.e., ‘the numbers’). The final barrier to diabetes-specific communication identified in this study was ‘Providers “Talking Down to” careseekers regarding their diabetes care and self-management’. Although the majority of participants described positive relationships with their providers, some described interactions with providers that made them feel disrespected and thus less likely to openly communicate about their condition and concerns.
One study found that 24% of careseekers wanted more information after receiving a diabetes diagnosis and 23% wanted more psychological support and reassurance.[20] Hence it is important to talk about multiple topics in each healthcare visit, suiting the needs of the individuals.
Diabetes Self-management Education (DSME)
DSME provides the information, skill and ability needed for diabetes self-care. Individual empowerment is the cornerstone of modern diabetes management.[21] Structured DSME is the principal driver of self-empowerment. DSME is most applicable and mandatory at initial diagnosis of diabetes, when not meeting therapeutic goals, when complications develop, during transition at various phases of life and every year.
Topics to consider in diabetes communication
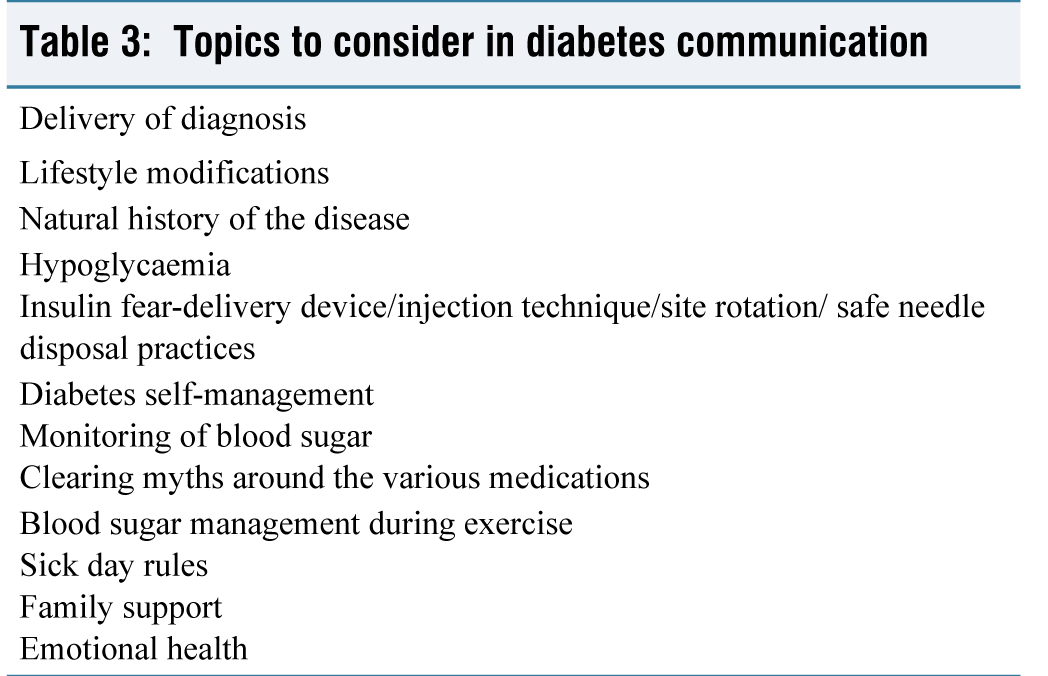
The principles and key elements of DSME recommended in a joint position statement of the American Diabetes Association, the American Association of Diabetes Educators (AADE), and the Academy of Nutrition and Dietetics include [Table 3]:
Information sharing: Provide ‘need-to-know’ information; take advantage of ‘teachable moments’ Assess individual/family needs for the behavioural and psychosocial aspects Psychosocial and behavioural support Integrating with other therapies
Diabetes Distress, Burnout
Diabetes distress is defined as the frustration and feeling of defeat in an individual with diabetes due to the disease, daily self-management and (the prospect of) its long-term complications.[22] It can also arise from the social impact of diabetes (e.g., stigma, discrimination or dealing with other people’s unhelpful reactions or their lack of understanding) and the financial implications of the condition. MILES 2 study has shown that 25% with Type 1 diabetes, 20% with insulin-treated Type 2 diabetes and 10% with non-insulin treated Type 2 diabetes suffer from diabetes distress.[23]
Greater diabetes distress is associated with suboptimal diabetes self-management, A1C, decreased self-management behaviours and impaired general emotional well-being. People with diabetes who experience psychological problems often prefer to talk about this with their diabetes health professionals or their primary care provider (PCP) rather than with a mental health specialist.[24] The problem areas in diabetes (PAID) scale and diabetes distress scale (DDS) are used to identify diabetes distress and to guide conversations about diabetes distress.[25,26] Diabetes distress can turn into depression if left unaddressed. Hence it is important from the physician’s perspective to address this.
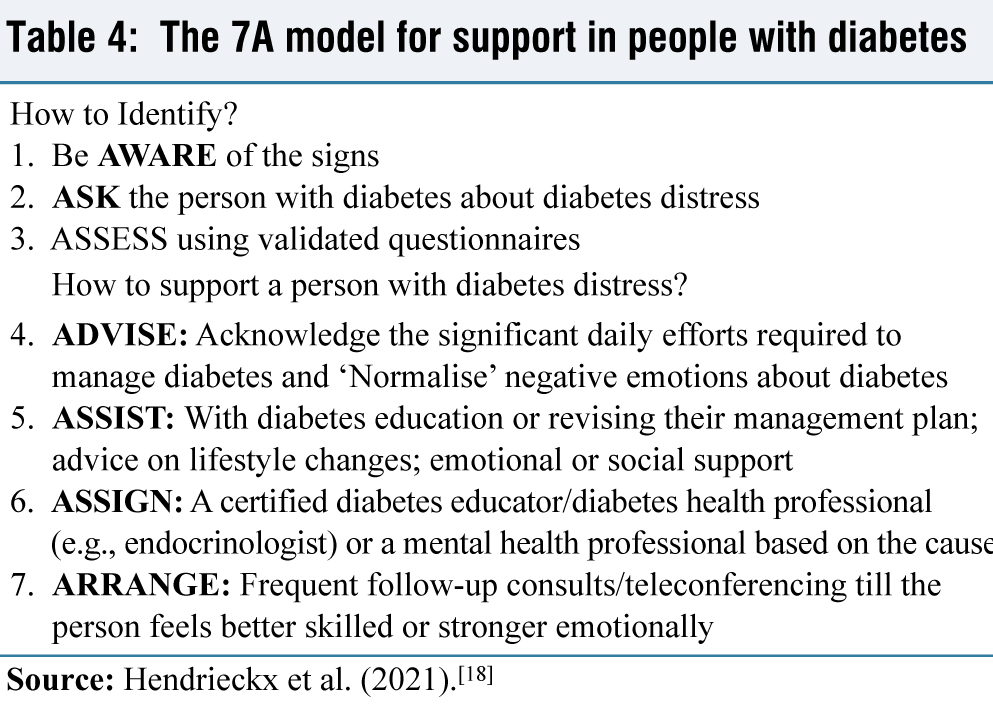
The 7A model helps us to identify and support an individual with diabetes distress (AWARE/ASK/ASSESS/ADVISE/ASSIST/ARRANGE) [Table 4].
The 7A model for support in people with diabetes
Ways of Improving Communication
Retrospective data reveals an imbalance between the needs and preferences of individuals with diabetes and providers in clinical communication. Careseekers often prefer values of interaction including trust, respect, use of analogies, and supportive relationships, and health care providers tend to concentrate more on system-level factors (e.g., limited time, diabetes educators and nurses, cultural and socioeconomic position of individual person and macro-level interventions and lack of time).[27]
A study by Khurana et al. has revealed that people with diabetes (81%) were interested in using electronic methods (e.g., app on a smartphone, email or text messages) to interact more with HCPs between visits. The majority of subjects were interested in using technology to help manage their Type 2 diabetes, including 62% favouring communicating with their health-care providers via email and a considerable fraction interested in using smartphones to be provided medication reminders (56%), clinical visit scheduling (55%) and text messaging (49%).[28]
Recommendations support motivational interviewing as a valuable technique that can be used by providers. It involves a nonconfrontational style with empathy to increase the motivation for behaviour change, with aspects of self-management, treatment and also to build therapeutic relationships.[29]
Strategies to Improve Communication Skills in Medical Practice
Medicine being a people-centred profession, communications skills are very essential for medical practice. Traditional medical teaching in India imparts students with theoretical and practical knowledge of disease processes and trains them about the diagnostic and treatment modalities, but does not focus on the need for communication skills.[30]
Communication skills increase the clinical competence, and the training should commence at the earliest, probably during the clinical medicine teaching.[31] Deveugele et al. in their efforts to teach communication skills to medical students used various methods like group discussions in small groups (10-15 students), with focus on role playing with colleagues, simulated people living with diabetes, showing videotapes of real consultations and observed a positive effect in the communication skills of students.[32]
Haq et al. in their paper describe the content and methods used to teach communication skills to medical students. Curricular themes/projects focusing on conflict resolution, delivery of bad news, addressing individual preferences, community health education, communicating with families, and working effectively with people from diverse backgrounds. Students’ communication skill competencies were assessed through a variety of methods including objective structured clinical examinations, focused observation and feedback, and debriefing sessions based on recall, audiotapes, or videotapes of encounters. Curriculum projects should be designed to improve medical students’ communication skills during the undergraduate years, which they can refine and practice throughout the MBBS course and later [Figure 1].[33]
A Structured skill training (CST) for medical students and HCPs should be preferred. A Cochrane meta-analysis of 91 studies analysed the effect of CST interventions among medical students on five outcomes, namely overall communication, empathy, rapport, gathering and sharing of information, which showed an overall improvement in communication. The meta-analysis also observed that programs that included personalised feedback were more helpful in improving communication skills, whereas online or self-directed programs made no difference.[34]
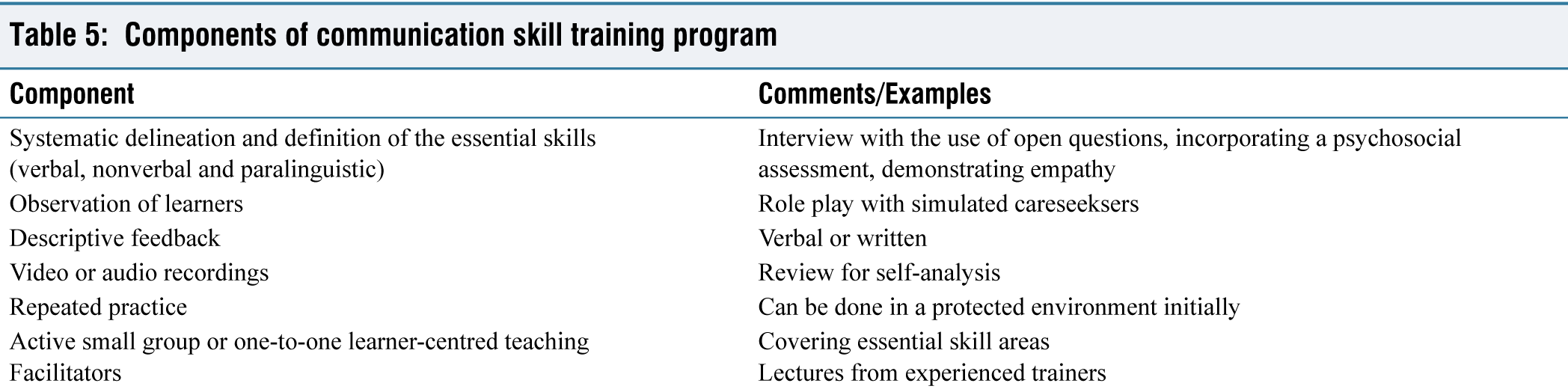
The CST module focuses more on building a relationship, the structuring of an interview, initiating discussion, gathering information, explaining, planning and closure. The fundamental components of a CST are mentioned in Table 5.[35]
Components of communication skill training program
Conclusion
The exponential rise in the prevalence of diabetes necessitates the need for patient-centred communication and fosters a better relationship between the careseeker and provider. The incorporation of skills and strategies for effective communication should be integrated right from medical training of HCPs. A multidisciplinary synergistic teamwork, including individuals with diabetes, a primary care physician, a diabetic educator, a dietician and an endocrinologist, can overcome the complexities in the management of the person with diabetes. The emergence of digital health technologies with mobile applications and artificial intelligence-based tools can be implemented to address the unmet needs and facilitate effective communication.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Not applicable.
Credit author statement
TL conceptualised the ideas and supervised the writing of paper.
GL and NK drafted the paper and contributed to the text.
TL and CS provided revisions to the scientific content of the document.
Data availability
Not applicable.
Use of artificial intelligence
Not applicable.