
Abstract
Background and Aim:
Arteriovenous malformations (AVMs) are uncommon in the elbow, particularly within the triceps muscle. Due to their rarity and complex nature, they can be misdiagnosed as other soft-tissue conditions, leading to inadequate treatment and potential complications.
Methods:
This report presents a case of an intramuscular AVM in the triceps of a 19-year-old student.
Results:
The diagnostic process, which included physical examination and imaging studies, is outlined, along with the surgical technique used for AVM excision. The patient had a positive outcome at the one-year follow-up, with no recurrence.
Conclusions:
This case study offers clinicians a framework for diagnosing, evaluating and treating upper extremity masses suspected to be AVMs.
Keywords
Introduction
Arteriovenous malformations (AVMs) represent a distinct category of vascular anomalies characterised by direct connections between arteries and veins, thus circumventing the capillary system. While frequently observed in the head and neck, these lesions can occur less commonly in the extremities.[1] Intramuscular AVMs, especially those within the triceps brachii, are notably rare. The development of AVMs is believed to stem from disruptions in vascular morphogenesis during foetal development or abnormal blood vessel formation.[2] These vascular malformations, which are present from birth, can be aggressive, may lead to tissue destruction, have high recurrence rates, and are occasionally associated with genetic disorders like Rendu-Osler-Weber syndrome, which involves mutations in growth factor receptors.[2,3]
The clinical presentation of AVMs can vary widely, making diagnosis difficult as they can mimic other soft-tissue conditions such as lipomas, fibromas, haemangiomas or bursitis. Unlike haemangiomas, which are related to endothelial cell proliferation, AVMs result from the abnormal development of the vascular system during embryogenesis.[3] These lesions may not become apparent until there is growth or vascular congestion, potentially triggered by factors like thrombosis, trauma, infection or hormonal changes.[3] As such, these vascular malformations are usually not detected before adolescence.[2,3] Moreover, their behaviour can be unpredictable, with risks of enlargement, bleeding and skin breakdown. The infrequent occurrence of upper extremity AVMs, particularly in the triceps muscle, results in limited medical literature to assist clinicians in managing these cases effectively.[3-5] This report presents the unusual case of a benign intramuscular AVM in the triceps of a 19-year-old student, outlining the diagnostic process, surgical approach and favourable result.
Case Report
A 19-year-old male student presented to the clinic with a gradually enlarging, painless mass on the posterior aspect of his right upper arm, which had been noticeable for approximately one-year. He had no history of trauma, recent infections or systemic symptoms. Although he engaged in recreational sports, the mass caused no functional limitations. He denied any stiffness or weakness in the affected arm.
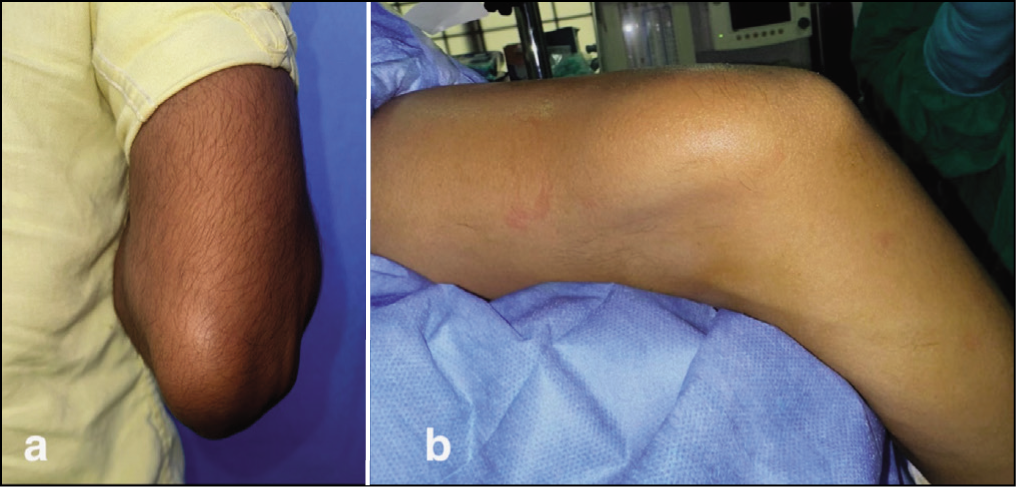
Physical examination revealed a soft, non-tender, mobile mass, approximately 4 cm × 3 cm, palpable in the posterior-medial distal arm, within the triceps muscle [Figure 1]. The mass was not pulsatile, and no bruit was detected on auscultation. The skin overlying the mass appeared normal, with no discolouration or visible dilated veins. The elbow and shoulder joints showed a full, painless range of motion. Neurological examination of the right upper limb was normal.
Clinical photographs (a,b) demonstrating the mass located on the posterior and medial aspect of the right distal arm
Investigations
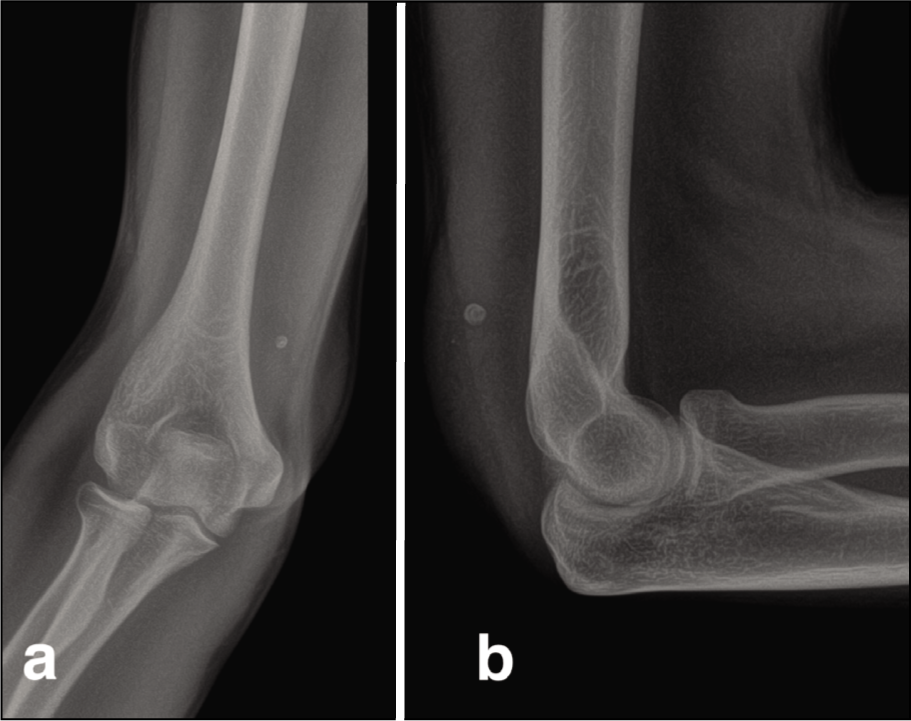
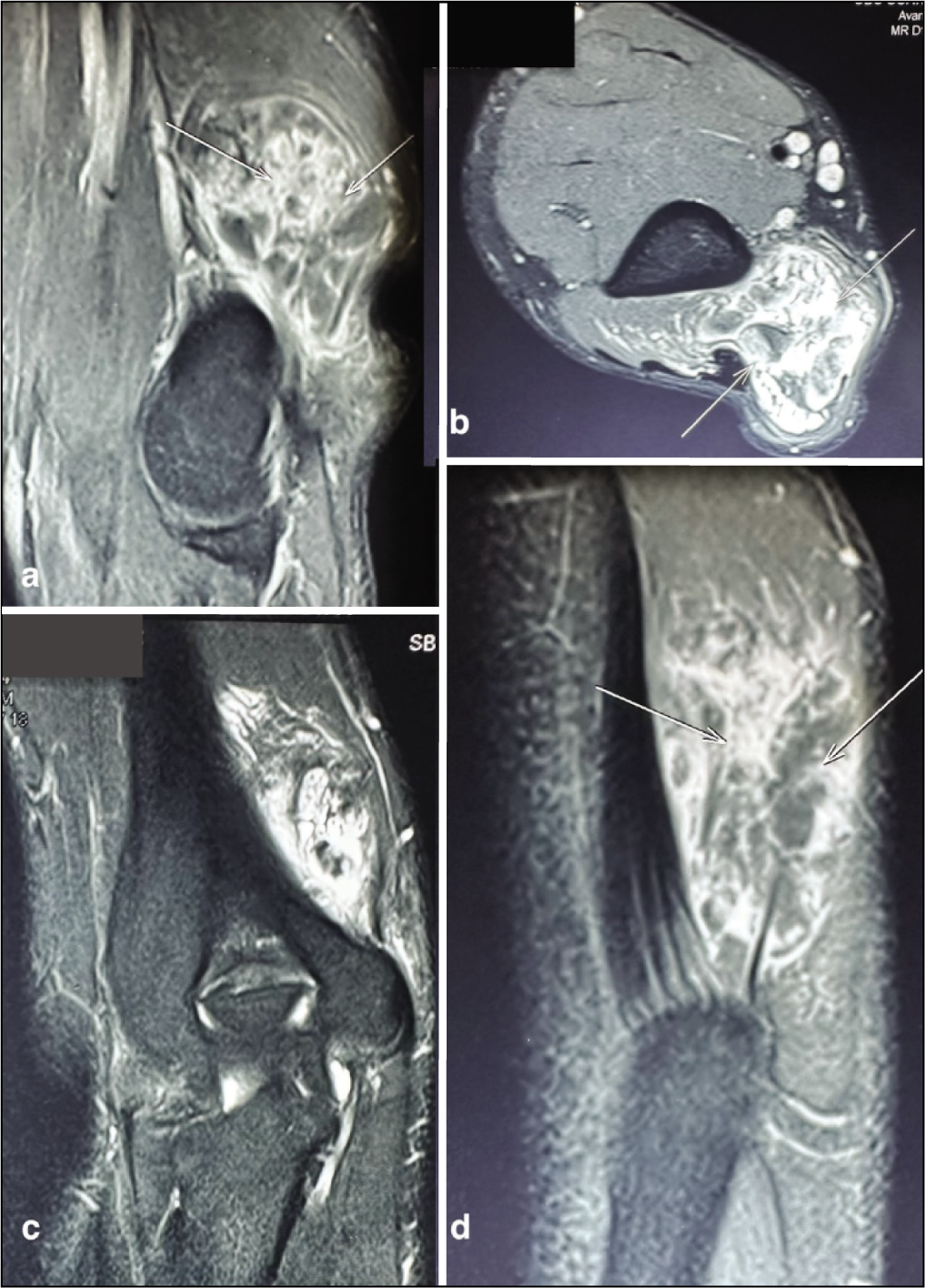
Initial radiographs of the right elbow revealed a phlebolith (a small, often venous calcification) without any signs of fractures or bone involvement [Figure 2]. An ultrasound showed a well-defined, heterogeneous mass within the triceps, with significant internal blood flow visible on colour Doppler. Magnetic resonance imaging (MRI) was conducted for further characterisation. The MRI revealed a poorly defined, lobular, intramuscular mass in the distal triceps, primarily on the medial side, measuring about 5.1 × 4.4 × 4.1 cm. The mass displayed mixed signal intensity, with hyperintensity on both T1- and T2-weighted images and internal heterogeneity. Flow voids within the mass indicated high-flow vessels and small phleboliths were noted [Figure 3].
Radiographs of the right elbow show a phlebolith (a small calcification often found in veins) in the posteromedial aspect of the distal arm, without evidence of fractures or bone involvement
Pre-operative MRI of the right arm. (a) Sagittal view illustrating a poorly defined, lobular mass with mixed signal intensity within the distal triceps, predominantly medially, with small phleboliths (arrows). (b) Axial T2-weighted image revealing a hyperintense, lobulated mass in the long head of the triceps, with phleboliths (arrows). (c) Coronal T1-weighted image showing varied signal intensity within the mass on the medial side. (d) The mass appears mainly hyperintense on both T1- and T2-weighted images, with internal heterogeneity. Multiple flow voids within the mass suggest high-flow vessels and small phleboliths are visible (arrows)
Post-contrast imaging showed varied enhancement of the lesion. It extended inferiorly to the triceps attachment, near the humerus’s posterior cortex and olecranon, but without cortical erosion or bone marrow oedema. There was no joint involvement. The lesion exerted minimal pressure on the ulnar nerve near the elbow. These findings raised a strong suspicion of a vascular malformation.
Other Differential Diagnoses Considered
Based on the investigations, particularly the MRI findings of a heterogeneous, enhancing mass with flow voids, several differential diagnoses were considered. These included:
Haemangioma: While the MRI suggested a vascular lesion, haemangiomas typically have a more homogeneous appearance and different enhancement patterns. Lymphatic malformation: These lesions usually have a more cystic appearance on MRI and lack the prominent flow voids seen in this case. Soft-tissue sarcoma: Although less likely given the patient’s age and lack of other concerning features, sarcomas can sometimes present as heterogeneous masses. The presence of flow voids and phleboliths made this less probable. Lipoma: Lipomas are common soft-tissue masses, but they typically have a characteristic fatty signal intensity on MRI, which was not observed in this case. The presence of flow voids also argued against a lipoma. Fibroma: Fibromas are also possible, but they generally do not show the same degree of vascularity on imaging as seen in this case.
The presence of flow voids and phleboliths on MRI, along with the ultrasound findings of significant internal blood flow, strongly favoured a vascular malformation, specifically an AVM.
Treatment
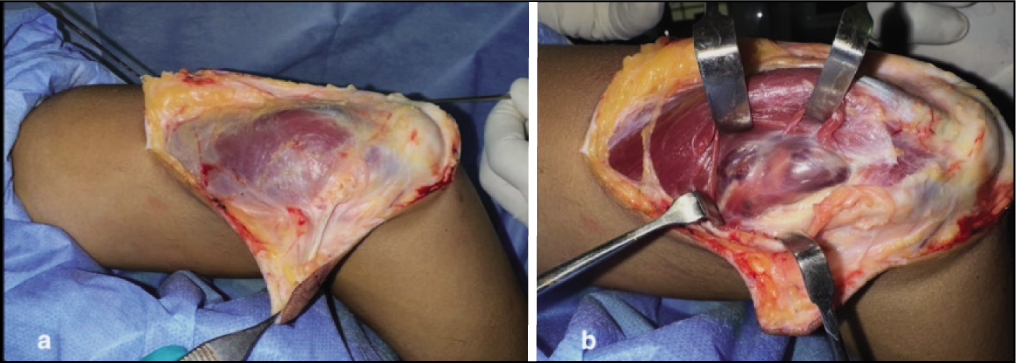
Following an extensive discussion with the patient regarding the diagnosis and treatment options, a decision was made to proceed with surgical excision of the AVM. The patient was positioned in the left lateral decubitus position, with the right arm supported, elbow flexed and positioned upwards. Anaesthesia was administered via a supraclavicular brachial plexus block. A tourniquet was placed on the upper arm to control bleeding. A curvilinear incision, with a zig-zag element for better exposure, was made over the posterior right arm above the mass. Careful dissection through subcutaneous tissues was followed by an incision in the triceps fascia. The AVM, located within the long head of the triceps, appeared as a well-defined mass of twisted, enlarged vessels [Figure 4].
Intraoperative photographs. (a) The initial appearance of the mass within the muscle. (b) The AVM is exposed within the long head of the triceps, presenting as a well-defined mass of intertwined vessels
The AVM was dissected from distal to proximal within the triceps muscle. The main arterial feeders, branching from an intramuscular section of the deep brachial artery, were carefully identified, cauterised with bipolar forceps and tied off with sutures. The associated veins were similarly treated. The mass extended to the posterior elbow joint capsule, and during its mobilisation, a minor tear in the capsule was promptly repaired with absorbable sutures. The ulnar nerve was identified, protected and gently moved aside as needed. The AVM was removed entirely in one piece without substantial bleeding during the operation [Video 1]. The removed tissue was sent for pathological examination [Figure 5].
Gross pathology specimen showing a well-circumscribed, subcutaneous fatty mass measuring 5 × 4 × 3 cm with scattered haemorrhagic areas
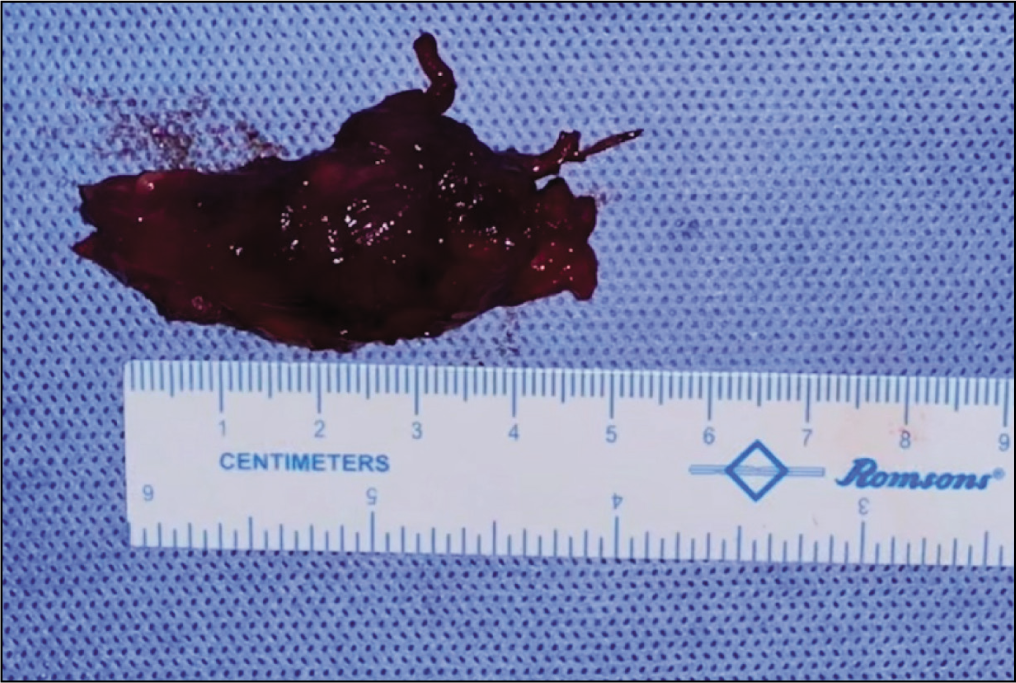
Histopathology
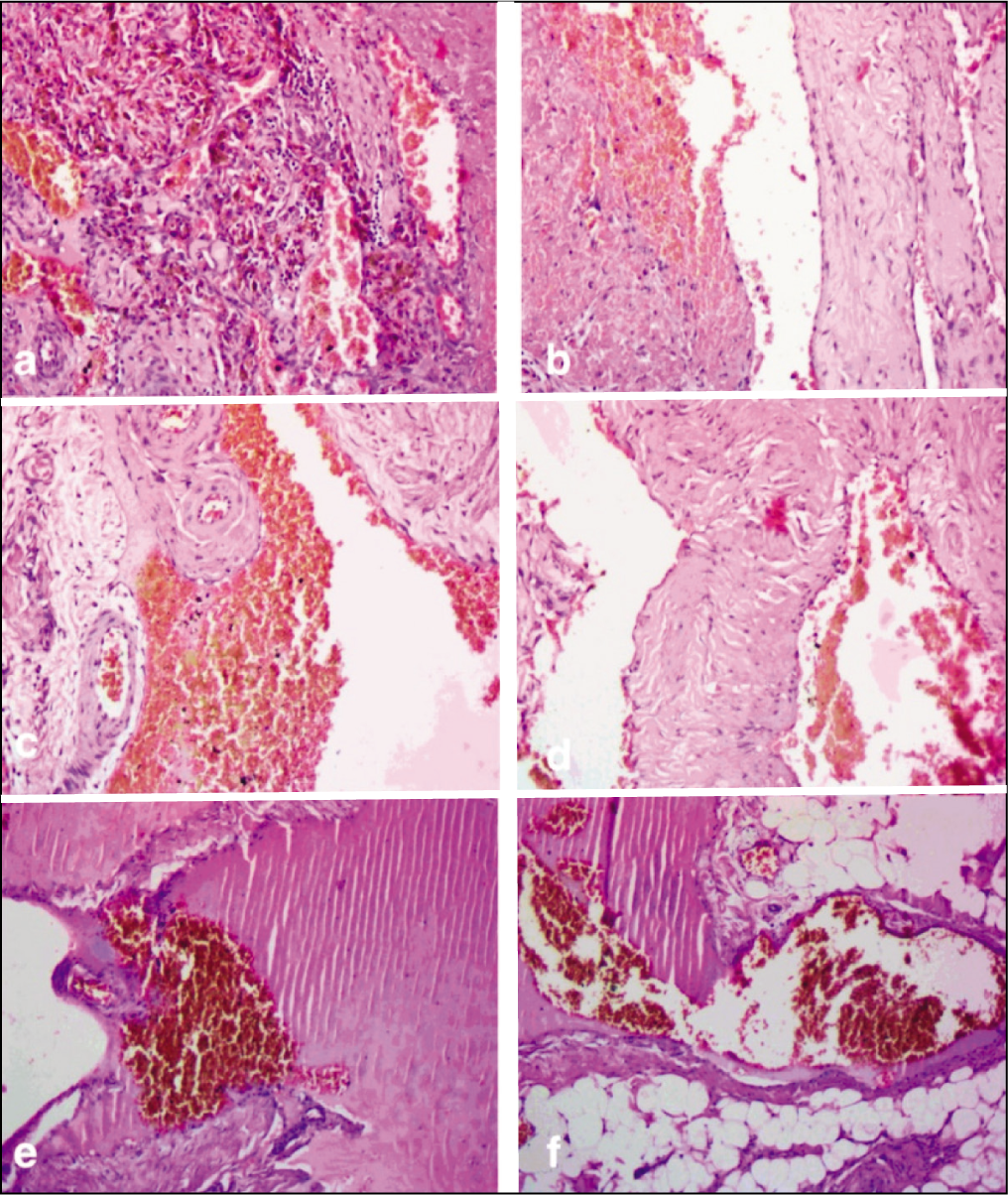
Histopathological examination confirmed the diagnosis of a benign AVM. Gross examination revealed a well-defined, subcutaneous fatty mass measuring 5 × 4 × 3 cm, with scattered haemorrhagic spots. Microscopic sections showed a complex vascular lesion within adipose tissue, fascia and muscle. The lesion comprised numerous blood-filled vascular channels of varying sizes, including thick-walled arteries and thin-walled veins, consistent with an AVM [Figure 6]. These vessels formed an interconnected network. The smooth muscle and elastic fibres in the vessel walls were disorganised. No signs of endothelial atypia, pericytic proliferation, viral inclusions, dysplasia or malignancy were found. These findings confirmed a benign AVM.
Histopathology of the excised specimen. (a-d) Low-power images showing multiple thick-walled arteries and veins. (e,f) High-power images demonstrating disorganised smooth muscle and elastic fibres in the vessel walls, consistent with an AVM
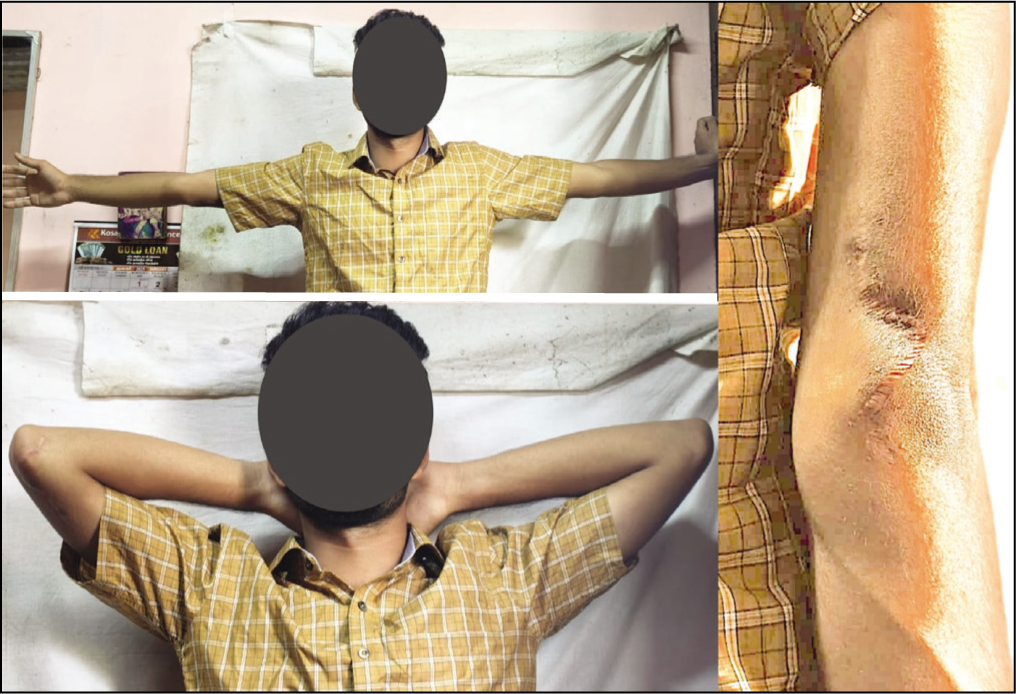
Postoperative Course
The patient’s postoperative recovery was smooth. The surgical drain was taken out on the second day after surgery. He was discharged with instructions for wound care and to start gentle exercises to maintain range of motion. At a two-week check-up, the wound was healing well, and he reported no pain or difficulty with movement. He was encouraged to resume normal activities gradually. One-year later, he remained symptom-free, had regained full elbow and shoulder mobility, and had resumed all previous activities, including sports, without any issues. There was no clinical or radiological indication of recurrence [Figure 7].
Discussion
AVMs are vascular anomalies that make up about 7% of all benign tumours and are relatively common in infants and children.[5] While they can develop anywhere in the body, they are most commonly found in the pelvis, within the skull, and in the lower limbs.[6] Intramuscular AVMs in the triceps, as seen in this patient, are quite rare, with only a few documented cases.[4,5] This scarcity, combined with the diverse ways AVMs can present, makes their diagnosis and management challenging.
Diagnosing AVMs typically involves a combination of physical examination, imaging and sometimes angiography. MRI is useful for showing the lesion’s extent and identifying the characteristic flow voids. Digital subtraction angiography (DSA) is considered the most accurate method for outlining the vascular structure and blood flow dynamics, though it was not used in this case due to its invasive nature and limited availability.[2]
Treatment for AVMs varies depending on the individual case, considering factors like size, location, blood flow and symptoms. Options include conservative approaches (observation, compression) or more invasive procedures like endovascular embolisation or surgical removal. Various agents have been used for embolisation, including ethanolamine oleate, absolute ethanol, polidocanol, n-butyl cyanoacrylate, coils, polyvinyl alcohol foam powder and superabsorbent polymer microspheres, with mixed results and potential risks like pain, complications and tissue damage.[7,8] Given the clear boundaries of the AVM in our patient and his symptoms, surgical removal was deemed the best option.
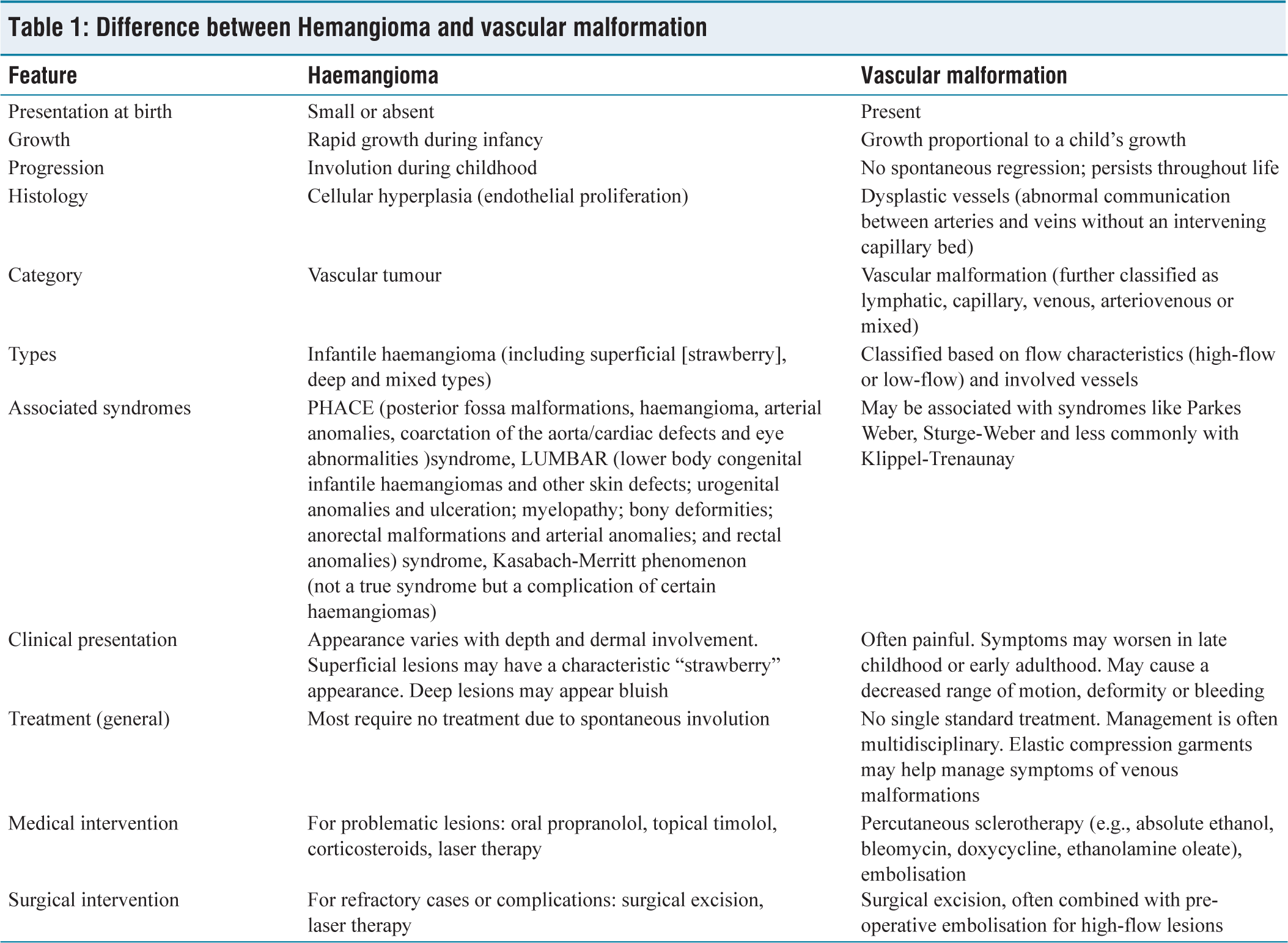
Distinguishing AVMs from other vascular growths, such as haemangiomas, is vital for proper treatment [Table 1]. As noted above, in this case, the differential diagnosis included haemangioma, lymphatic malformation, soft-tissue sarcoma, lipoma and fibroma. However, the MRI findings, particularly the presence of flow voids and phleboliths, along with the ultrasound evidence of significant blood flow, were most consistent with an AVM. The Mulliken and Glowacki classification helps differentiate these conditions based on their growth patterns, cell activity and tissue structure.[9] Vascular tumours like haemangiomas grow through cell multiplication, while vascular malformations like AVMs result from abnormal vascular development and are categorised as either slow-flow or fast-flow lesions.[10,11] Misdiagnosis can lead to incorrect treatment, such as unnecessary watchful waiting or overly aggressive surgery.[9-11]
Difference between Hemangioma and vascular malformation
In our case, the delayed diagnosis and the complex nature of the AVM, especially its proximity to the elbow joint, posed particular challenges. The successful outcome, marked by the patient’s pain relief, full functional recovery and excellent Mayo and DASH scores, supports the effectiveness of complete surgical removal for similar intramuscular AVMs. Punit et al.[4] reported a comparable case of a vascular malformation in the triceps of a 33-year-old woman, initially misdiagnosed as a lipoma. Their successful surgical removal without recurrence after a year aligns with our findings. The decision for open surgery in our case was based on the lesion’s defined nature and its location within the triceps. Careful dissection, including identifying and tying off feeding vessels, allowed for complete removal and reduced the risk of recurrence, which is a concern with AVMs due to their potential for continued growth.[2,4,7]
This case contributes to the limited body of knowledge on intramuscular AVMs in the triceps. It emphasises the need to consider AVMs when diagnosing soft-tissue masses in the upper extremities. Careful planning before surgery, including detailed MRI imaging, is crucial for safe and effective treatment. When feasible, complete surgical removal remains the best approach for a cure and to minimise recurrence in these complex cases.
Conclusion
This case underscores the importance of considering AVMs in the differential diagnosis of soft-tissue masses, especially in unusual locations like the triceps muscle. Accurate diagnosis, facilitated by MRI, enables appropriate treatment planning. As shown in this rare instance of a triceps AVM, complete surgical excision provides the best chance for a cure and excellent long-term functional outcomes, reinforcing its role as the preferred treatment when possible.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Ethical approval was obtained from the OHRC Ethical Committee Board, reference number 40/2024, dated 2nd December 2024.
Informed consent
The patient’s family provided informed consent for the publication of the data and images.
Credit author statement
J Terrence Jose Jerome: Roles/writing – original draft, Data curation, Conceptualization, Writing – drawing, review & editing.
Data availability
The data supporting this study are available upon request from the corresponding author.
Use of artificial intelligence
The use of artificial intelligence is not relevant to this article, as it does not involve AI technologies or methodologies in its analysis or conclusions.