
Abstract
Background and Aims:
Escherichia coli (E. coli), a gram-negative bacillus, causes a variety of infectious diseases, such as urinary tract infections, abdominal infections and sepsis. It is a frequent cause of meningitis in neonates, although rarely a causative agent in adult meningitis. E. coli meningitis in adults is associated with head trauma, neurosurgical procedures and immunocompromised conditions. Endogenous endophthalmitis is an eye condition which may result in visual loss due to the involvement of intraocular structures by the hematogenous spread of infection to the eye from another site in the body.
Case Report:
Here, we report a case of spontaneous E. coli meningitis in an elderly immunocompetent adult complicated by septic arthritis and bilateral endophthalmitis.
Conclusion:
E. coli meningitis in immunocompetent adults is rare and the complications are unpredictable, so these patients should be managed promptly and examined regularly to look for complications including endophthalmitis and septic arthritis, as early management leads to better outcomes.
Introduction
Escherichia coli (E. coli), a gram-negative bacillus, causes a variety of infectious diseases, such as urinary tract infections, abdominal infections and sepsis. E. coli meningitis is commonly observed in neonates, but it is rarely identified as the cause of meningitis in adults. In adults, this type of meningitis is commonly linked to head trauma, neurosurgical procedures, or immunocompromised states.[1] Endogenous endophthalmitis is a condition affecting the eye that can lead to vision impairment as a result of the infiltration of intraocular structures by the hematogenous spread of infection from a different site in the body. Here, we report a case of spontaneous E. coli meningitis in an immunocompetent adult complicated by bilateral endophthalmitis.
Case Presentation
A 77-year-old male hypertensive presented to the Emergency Department with complaints of fever of four days duration and altered sensorium of one day. On examination, he was found to have a high-grade fever with signs of meningeal irritation. His level of consciousness was diminished with a Glasgow Coma Scale (GCS) score of 10/15 (E3M5V2). He was started empirically on ceftriaxone, vancomycin, acyclovir, paracetamol and intravenous fluid. Initial laboratory findings were showing raised blood leucocyte count (13,960 with 90% neutrophil). Non-contrast computed tomography (NCCT) of the brain showed hypodensity in the left frontal gyrus involving the cortex and underlying subcortical white matter. Lumbar puncture was done and cerebrospinal fluid (CSF) was sent for analysis which showed raised CSF protein (204), low glucose (23) and raised TLC (400 cells, neutrophil predominant N75%, L25%). The CSF rapid meningitis PCR (film array) panel revealed E. coli K1. Intravenous antibiotics were modified. He developed subconjunctival haemorrhage along with chemosis and oedema of bilateral eyes (Left>Right) during the hospital stay (Day 6 of admission) [Figure 1]. Ultrasound (USG) orbit bedside was done, and imaging was suggestive of bilateral panopthalamitis (left > right). Contrast-enhanced magnetic resonance imaging (CEMRI) of the brain with orbit showed patchy areas of thick leptomeningeal as well as pachymeningeal enhancement in bilateral frontal, temporal, occipital and right parietal region, along with diffuse enhancing uveal/scleral thickening in both eye globes, oedematous swelling of periorbital soft tissue and thickening of extraocular muscle (Left>Right) [Figures 2 and 3]. Intravitreal antibiotics were given by the ophthalmologist in the eye. There was also development of pain and swelling of the right knee joint. USG knee joint was done, and imaging was suggestive of infective aetiology, involving right knee joint. Aspiration from right knee was done under aseptic precautions and fluid was aspirated and sent for Gram staining and culture and sensitivity. Repeat CSF was done on day 15 of admission, which showed improved cyto-biochemical analysis (Protein - 109, TLC-10). Patient’s sensorium and general condition improved during the course of the stay in hospital. At the time of discharge, patient was conscious, alert and obeying commands with visual loss bilateral eye (left>right).
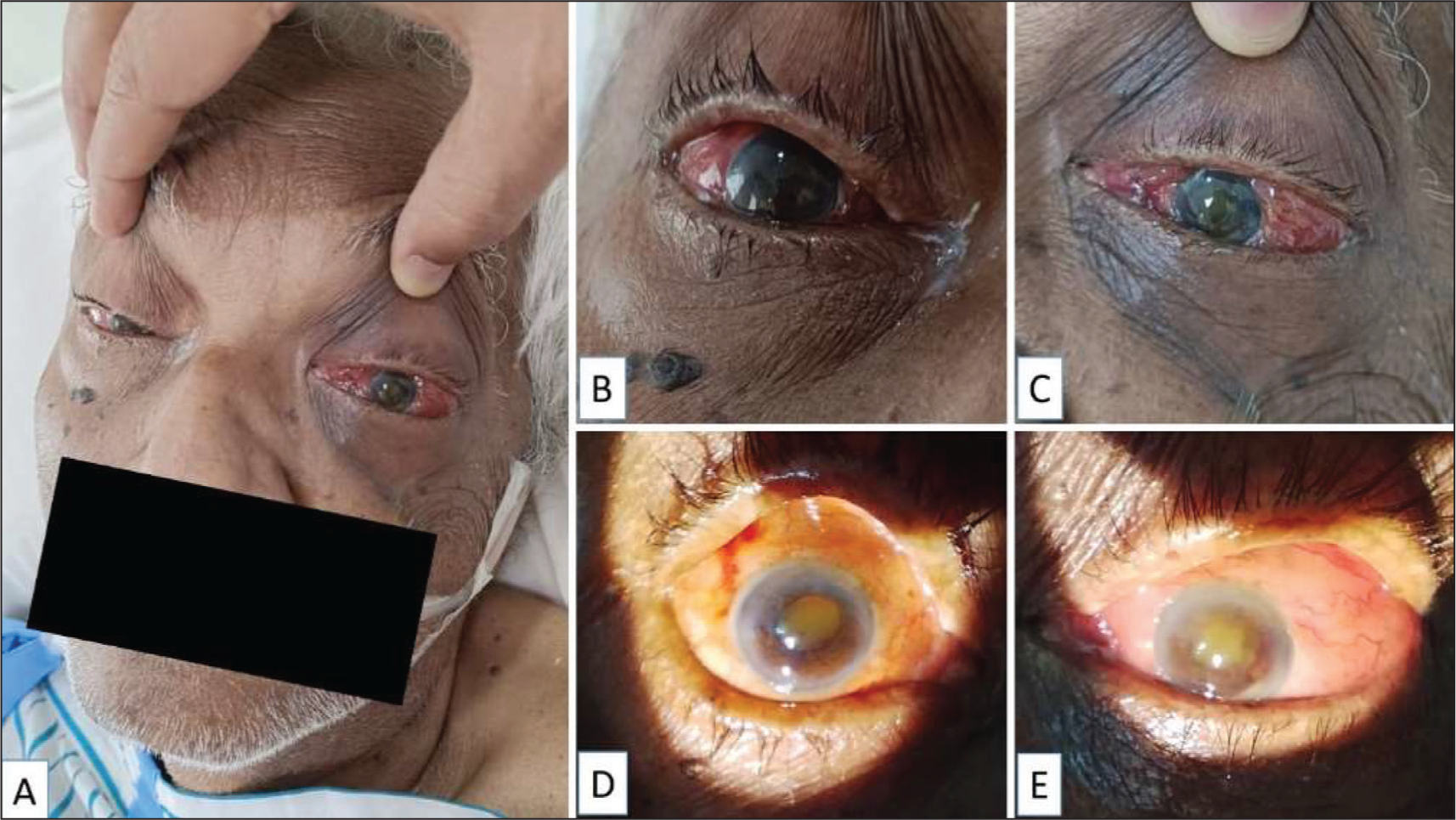
Ophthalmic findings suggestive of bilateral endogenous endophthalmitis in the index case: toxic look and left-sided periocular oedema (A), bilateral lid oedema and conjunctival chemosis (B, C), corneal haze, blood-stained hypopyon, mid-dilated and fixed pupils with yellowish glow and no view of fundi (D, E). All findings were more severe in left eye (C, E) compared to right eye (B, D)
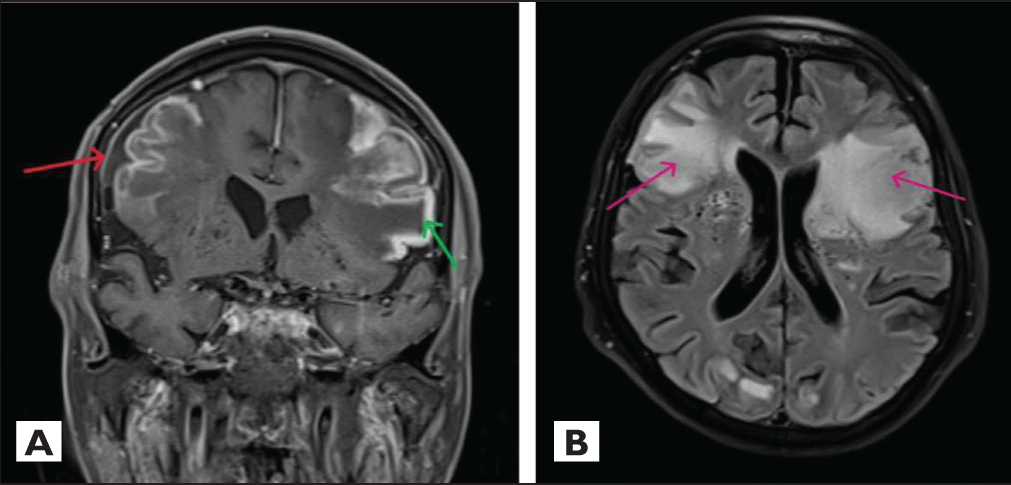
T1W postcontrast coronal image showing pachymeningeal (red arrow) and gyriform enhancement (green arrow) (A) and FLAIR axial image showing hyperintense signal intensity in the bilateral frontoparietal regions (B)
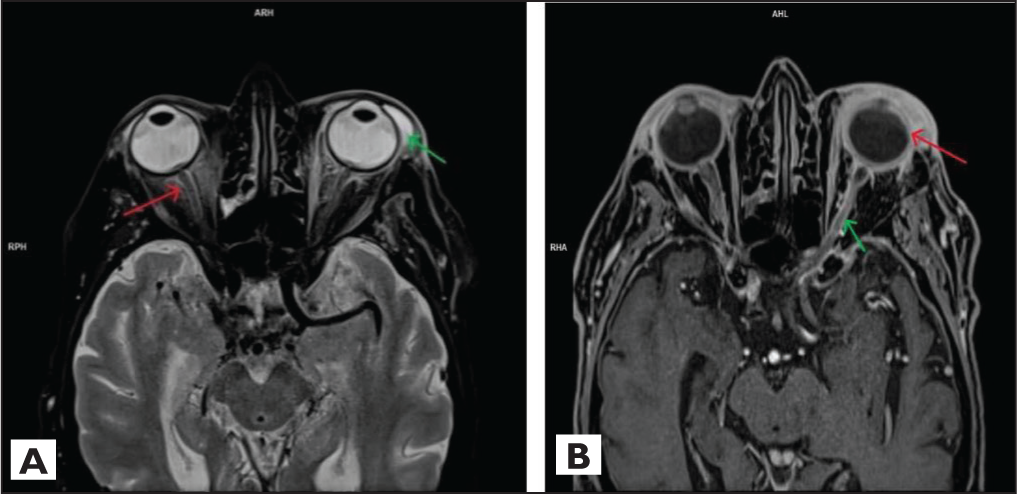
T2W fat sat axial image of orbit showing oedema/inflammatory changes in the retroorbital fat region (red arrow) and soft tissue oedema around the left eyeball (green arrow) (A) and T1W axial postcontrast image showing diffuse scleral enhancement on both sides (left>right) (red arrow) & mild diffuse optic nerve sheath enhancement (green arrow) (B)
Discussion
Meningitis, the inflammation of the meninges and the spinal cord, is a severe disease with a high fatality rate, and survivors often experience lasting complications.[2] It poses a significant public health concern. E. coli is seldom identified as a source of adult meningitis acquired within the community, with only one case reported annually worldwide.[3] The first instance of E. coli meningitis was observed in a 33-year-old woman following an abortion and documented by Theys and Gehrcke in 1923.[4] Our patient did not exhibit any of the risk factors commonly associated with E. coli meningitis, including immunocompromised status, alcoholism, cirrhosis, traumatic head injury or neurosurgical intervention.[5] The transmission of E. coli from the blood, urinary tract or gastrointestinal tract has been recorded in previous literature. In approximately half of the instances, the aetiology or origin of transmission remained elusive as we were unable to identify the primary source for E. coli. The classical triad of meningitis, which includes fever, neck stiffness and altered mental status, was observed in our patient. This combination is found only in 25% of individuals with E-coli meningitis.[6]
Bacterial endophthalmitis results from bacterial multiplication within the eye. A majority of endophthalmitis cases in the Asian population are attributed to Gram-negative bacilli.[7] Risk factors for endophthalmitis closely resemble those of E. coli meningitis and are present in almost all patients with endogenous bacterial endophthalmitis.[8]
The CSF analysis conducted on our patient revealed the presence of neutrophilic pleocytosis and elevated protein levels, along with a low concentration of CSF sugar. These findings are consistent with the characteristic profile observed in cases of bacterial meningitis. The CSF Gram stain was negative. The conclusive identification of bacterial meningitis is determined through CSF culture, with a positivity rate ranging from 50% to 90% in patients, but yielded a negative result in our particular case. The sensitivity of the CSF culture outcomes is reduced when antibiotics are given prior to conducting a lumbar puncture for obtaining the CSF sample.[9] Patients who have undergone antibiotic treatment before lumbar puncture may benefit from polymerase chain reaction (PCR) testing on the CSF. This is important because both CSF and blood cultures could potentially yield false negative results. In our case, the CSF biofire meningoencephalitis panel revealed a positive result for E. coli K1.
The management of E. coli meningitis requires the utilisation of a third-generation cephalosporin like ceftriaxone or cefotaxime, recognised for its effectiveness against gram-negative bacteria. A three-week regimen of intravenous antibiotic treatment is advised.
Bacteraemia and other concurrent infections are commonly associated with E. coli meningitis, particularly urinary tract infection, pneumonia and septic arthritis.[6] Our patient exhibited septic arthritis alongside bacterial endophthalmitis, a rare occurrence in conjunction with E. coli meningitis. Only a single was case reported in literature showing an association of endophthalmitis with E. coli meningitis.[10]
Patients with gram-negative bacillary meningitis experience a significantly higher mortality rate in comparison with cases of pneumococcal and meningococcal meningitis, as over 50% of these patients succumb to sepsis or multi-organ failure as the primary cause of death.
Conclusion
E. coli meningitis in immunocompetent adults is rare and the complications are unpredictable, so these patients should be managed promptly and examined regularly to look for complications including endophthalmitis and septic arthritis, as early management leads to better outcomes.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest concerning the research, authorship and publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethics committee approval number
The Institutional Ethics Committee Approval Number is not applicable as ethics approval was not required for this study.
Informed consent
Informed consent was obtained.
Credit author statement
Concept and design: Ankit Panjwani and Sanaullah Mudassir.
Data collection: Vidya Bhushan Kumar and Keshaw Kumar.
Data analysis and interpretation: Sanaullah Mudassir.
Manuscript drafting: Ankit Panjwani and Sanaullah Mudassir.
Critical revision: Ankit Panjwani and Sanaullah Mudassir.
Data availability
All data are included in the manuscript.
Use of artificial intelligence
The use of artificial intelligence is not relevant to this article, as it does not involve AI technologies or methodologies in its analysis or conclusions.