
Abstract
Objectives:
This case report aims to describe an extremely rare instance of isolated distal iliotibial band (ITB) rupture due to tuberculosis (TB), a condition that is seldom seen in clinical practice. The goal is to highlight the diagnostic challenges, ultrasound findings and the successful treatment of this condition in a non-athlete patient with non-resolving lateral knee pain.
Methodology:
A 33-year-old female with no history of trauma or pulmonary TB presented with chronic lateral knee pain. Initial ultrasound (USG) suggested ITB friction syndrome, but the symptoms worsened despite treatment. A second USG revealed increased ITB thickness, partial rupture and fluid collection. Histopathological examination of the tissue sample identified granulomatous inflammation and caseous necrosis, while reverse transcription polymerase chain reaction (RT-PCR) confirmed the presence of mycobacterium tuberculosis.
Results:
The diagnosis of musculoskeletal tuberculosis involving the iliotibial band was confirmed, and the patient was successfully treated with anti-tuberculous therapy (ATT). The treatment resulted in the resolution of symptoms and recovery from the rupture.
Introduction
Musculoskeletal tuberculosis (TB) accounts for approximately 10% of all extrapulmonary TB cases. Vertebral involvement is the most common type of skeletal TB, accounting for about half of all cases of musculoskeletal TB.[1] The involvement of TB in peripheral joints, tendons, ligaments and bursa is rare.[2]
The presentation of musculoskeletal TB may be insidious over a long period, and the diagnosis may be elusive and delayed as TB may not be the initial consideration in the differential diagnosis. Concomitant pulmonary involvement may not be present, thus confusing the diagnosis even further.[1]
The iliotibial band (ITB) is a portion of the fascia lata. It terminates distally on the lateral tibial condyle, having the main ribbon-shaped insertion into Gerdy’s tubercle on the anterior aspect of the lateral tibial condyle.[3] The ITB transmits forces from the hip to the knee, acts as a lateral stabiliser of the knee and also serves an important postural function.[4,5]
Iliotibial band friction syndrome of knee is common in athletes, especially in runners and cyclists because of overuse injury. It occurs when ITB moves repetitively over lateral femoral condyle.[6-8]
Isolated distal ITB rupture caused by TB is a very rare entity, never yet reported in literature. There has been a single case report of ITB TB presenting as soft tissue mass.[9] We present a rare case of isolated distal ITB rupture caused by TB as a cause of lateral knee pain with focus on ultrasound findings.
Case Discussion
A 33-year-old female patient, gynaecologist by profession, presented with left lateral knee pain since two years. The patient was not an athlete and had a relatively sedentary life style. There was no history of trauma. The patient was afebrile. She had no history of pulmonary TB. Her chest X-ray was normal, and there was no other joint pain. On clinical examination, some swelling and tenderness over proximal lateral tibia in the region of Gerdy’s tubercle were found for which she was advised ultrasound sonography (USG).
First USG of Knee
Mild thickening with mild increased signal on Doppler was noted in ITB adjacent to the lateral femoral condyle with mild soft tissue thickening/synovial thickening between ITB and the underlying lateral femoral condyle. Small knee joint effusion was noted.
Thus, imaging diagnosis of ITB friction syndrome was suggested, for which the patient was advised physiotherapy by an orthopaedist, and blind steroid injection was administered elsewhere. The patient’s symptoms worsened after that; hence, further USG was performed to check the status of ITB.
Second USG of Knee
The thickness of ITB was increased as compared to that found in the previous USG. Also, there was moderate oedema with fluid and collection between ITB and the lateral femoral condyle. There was partial tear of ITB near the lateral femoral condyle with evidence of small collection superficial to ITB [Figures 1 and 2].
(A) Panoramic USG image of a case showing tear of the iliotibial band (ITB) the above femoral condyle (arrows). (B) Longitudinal USG image at the lateral aspect of the knee showing collection (arrows) below and superficial to ITB at the site of tear
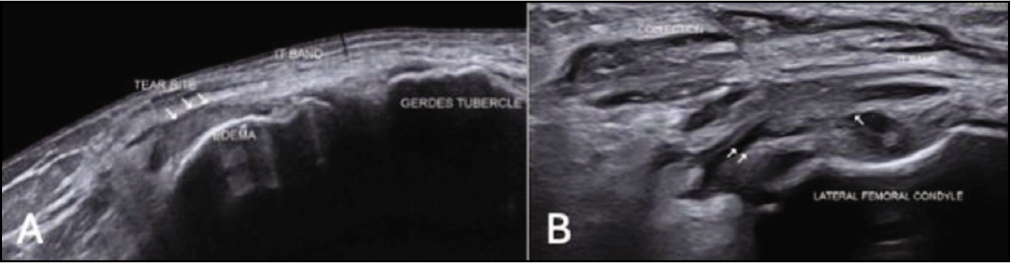
(A) Longitudinal USG image of the lateral aspect of the knee showing the distance of the longitudinal split of ITB from the insertion site at Gerdy’s tubercle. (B) Longitudinal USG image demonstrating the site of the longitudinal split in ITB (proximal site of split marked by the arrow)

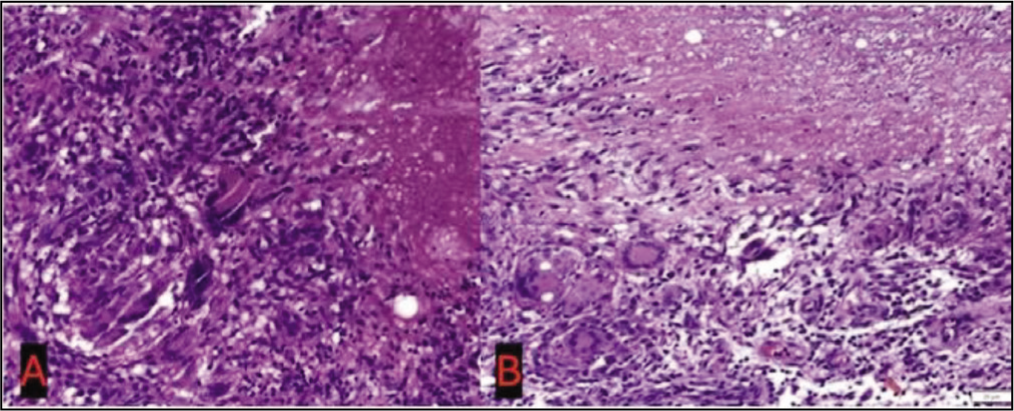
She had surgical debridement of collection with repair of ITB tear, and tissue was sent for histopathological examination that showed chronic inflammation, presence of multiple well-defined and confluent epithelioid granulomas, Langhan-type giant cells and areas of caseous necrosis, suggesting necrotising granulomatous inflammation in keeping with TB [Figure 3]. The reverse transcription polymerase chain reaction of the tissue sample was done that showed the presence of the mycobacterium TB complex, which was sensitive to rifampicin. The patient was successfully treated with anti-tuberculous therapy (ATT).
(A) Haematoxylin and eosin stained slide shows the presence of epithelioid cell granuloma with Langhans giant cells and the presence of caseous necrosis. (B) H&E (haematoxylin and eosin) stained slide shows the presence of prominently caseous necrosis, epithelioid cell granuloma with Langhans giant cells
Discussion
Tuberculosis of synovial sheath of tendon and bursa is a rare clinical and imaging entity. The incidence of tuberculous tenosynovitis and bursitis is 2%. TB tenosynovitis most commonly involves tendon sheath of the hand and the wrist and less commonly the foot and the ankle.[9,10] The IT band lacks a tendon sheath; however, it has paratenon like Achilles tendon that can be inflamed.[11]
ITB syndrome causes lateral knee pain in the area of the lateral femoral epicondyle or slightly below it, which occurs after repetitive flexion and extension of knee, typically in runners, cyclists and athletes. On physical examination, tenderness below epicondyle and superior to the joint line is an important finding [Figures 4–6].
Knee in Complete Extension

Knee in Complete Flexion

Post Operative Visible Scar of IT Band Repair and Biopsy 1 Year After Surgery

Three provocative tests are available for ITB assessment. The Noble test is performed with the patient in supine position. Beginning with the affected knee at 90° flexion, the leg is extended applying direct pressure over the lateral femoral epicondyle, with pain being reproduced near 30° of knee flexion. The Ober test is most commonly used test to assess the tightness of the tensor fascia lata and ITB. It is performed with the patient lying on the unaffected side in lateral decubitus, beginning with the affected knee supported and both hip and knee extended, and then abducting the hip, followed by releasing the knee support. A positive test is the failure of the knee to adduct. The Thomas test is used to check the tightness of iliopsoas muscle, rectus muscle and ITB. It is performed with the patient lying in supine position, asking the patient to flex the unaffected knee as far to chest as possible and hold; a positive test with opposite extended leg abducting indicates tight ITB.[12,13]
Both magnetic resonance imaging and USG may be used to assess ITB. Ultrasound sonography is valuable for the assessment of ITB syndrome as a cost-effective imaging modality that enables the visualisation of the superficial soft-tissue structures with high resolution and dynamic evaluation and helps their comparison with the contralateral healthy side.[14-23]
On USG, ITB is assessed in the longitudinal as well as the short-axis plane on the lateral aspect of the knee. Normal ITB appears as a linear fibrillar structure that crosses over the lateral epicondyle of the femur and inserts distally into Gerdy’s tubercle of the tibia.
USG findings of ITB syndrome include soft-tissue oedematous swelling of ITB and discrete fluid collection between the ITB and the lateral femoral epicondyle.[24-26] Cortical irregularity of the adjacent femoral epicondyle can also be observed.[27]
In the present case of ultrasound, there was thickening of ITB near the lateral femoral condyle that increased in a one-year interval with the development of the longitudinal split of ITB at this site. Also, there was an interval increase in fluid collection between ITB and the lateral femoral condyle with the development of collection superficial to ITB at the site of split.
The case represents a diagnostic challenge owing to its insidious onset and subtle non-specific symptoms. Ultrasound imaging in primary musculoskeletal TB with no pulmonary involvement can help narrow the differential diagnosis. The definitive diagnosis however requires the isolation of TB bacilli through biopsy and culture of the infected tissue. Percutaneous biopsy under USG guidance and microbiologic culture helps in diagnosing with a minimally invasive technique.
Conclusion
In patients with unresolving ITB friction syndrome, an alternative diagnosis of atypical infection like TB should be considered.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Not applicable.
Informed consent
Informed consent obtained from patient.
Credit author statement
All authors contributed to the paper.
Data availability
The data supporting the findings of this case report are available upon request from the corresponding author. The histopathological and microbiological data (including RT-PCR results) have been anonymized to protect patient confidentiality and are not publicly available due to privacy restrictions.
Use of artificial intelligence
AI was not used.