
Abstract
An 8-year-old girl presented with left leukocoria, prompting an evaluation that revealed bilateral intraocular masses, including a right upper nasal choroidal lesion and a large left heterogeneous mass with exudative detachment. Imaging and systemic assessment uncovered multiple intracranial lesions, miliary lung lesion, a facial lesion, and a right tibial lesion. A strongly positive tuberculin test and a history of close contact with a tuberculosis (TB) patient led to the diagnosis of disseminated TB. Treatment with anti-tuberculosis therapy and systemic steroids initially resulted in improvement, including regression of the ocular tuberculomas and enhanced visual acuity. However, the patient developed severe headache due to non-communicating obstructive hydrocephalus, necessitating surgical intervention. Despite intensive care, the patient ultimately succumbed to the condition. This case highlights that ocular TB lesions can mimic intraocular tumors and underscores the importance of comprehensive evaluation, including multimodal imaging and systemic work-up, for early diagnosis and management of disseminated TB.
Plain language summary
This case report describes an eight-year-old girl who developed unusual eye problems that appeared to be tumour but were caused by tuberculosis (TB), a bacterial infection. The child came to the clinic with a cloudy white spot in her left eye (leukocoria) and decreased vision. After thorough testing, doctors found masses in both eyes, lesions in her brain, face, and leg, and confirmed a TB infection. Treatment started with anti-TB medications and steroids, leading to an improvement in her eye condition and vision. Unfortunately, she later developed a life-threatening complication called hydrocephalus, which required emergency surgery. Despite efforts, she passed away. This case highlights the importance of considering TB as a possible cause of unusual eye problems, especially in children from areas where TB is common or with a known TB contact. Early testing, imaging, and treatment are crucial to managing this serious but treatable condition.
Introduction
Tuberculosis (TB) is a global health problem that is broadly classified as pulmonary or extrapulmonary. In 2022, approximately 1.25 million children and adolescents under the age of 15 were diagnosed with TB. 1
Recent studies have reported a rise in the incidence of extrapulmonary TB cases. The eye is one of the potential sites of extrapulmonary TB, being affected either in isolation or along with other organs in 1%–2% of TB patients. 2 TB could affect different ocular structures. 3 Patients with ocular TB may present with ocular manifestations that mimic intraocular malignancy or other inflammatory conditions.4,5 Failure to identify tuberculosis-related lesions and diagnose the underlying systemic disease can result in vision loss and, more critically, life-threatening complications. 5
Previous studies reported different unusual presentations of ocular TB in different age groups. As an unusual presentation, ocular TB may mimic retinoblastoma in the pediatric age group. 6 In this study, we a report a case of a child presented with bilateral intraocular masses as a presenting manifestation of disseminated TB. The study protocol was approved by the research ethics committee of the Faculty of Medicine, Ain Shams University, and a written informed consent was obtained from the mother of the child. The study followed CARE guidelines (Supplemental File 1).
Case report
An 8-year-old female presented to the ocular oncology clinic at Ain Shams University with left leukocoria. Two months before, the girl experienced pain, redness, and worsening vision in her left eye. Despite topical treatment with a combination of antibiotic and steroid eye drops prescribed at a primary care unit, her condition failed to improve, and her mother subsequently noticed a white pupil in the affected eye. Her past medical history revealed that she had been admitted for pneumonia 3 months prior. The family history revealed that the girl’s father was diagnosed with pulmonary tuberculosis and has been undergoing treatment for the past 6 months. Ophthalmological assessment of the patient showed 6/6 unaided vision in the right eye and light perception with good projection in the left eye. Pupil and anterior segment examination in the right eye were unremarkable while the left eye showed relative afferent pupillary defect, no red reflex, and detached infiltrated retina was seen retrolental during slit lamp examination (Figure 1). Dilated fundus examination showed blurred disc margin, hyperemic disc, and an upper nasal whitish deep lesion almost 2-disc diameter with surrounding cuff of subretinal fluid in the right eye (Figure 1). B scan ultrasound was done for both eyes (Figure 1) which showed dome shaped subretinal upper nasal lesion in the right eye and closed funnel retinal detachment in the left eye with a temporal exophytic lesion exhibiting heterogeneously high internal echogenicity. Ocular coherence tomography (OCT) line scans were taken over the right eye lesion and revealed an elevated dome shaped choroidal lesion with overlying subretinal fluid (Figure 1).
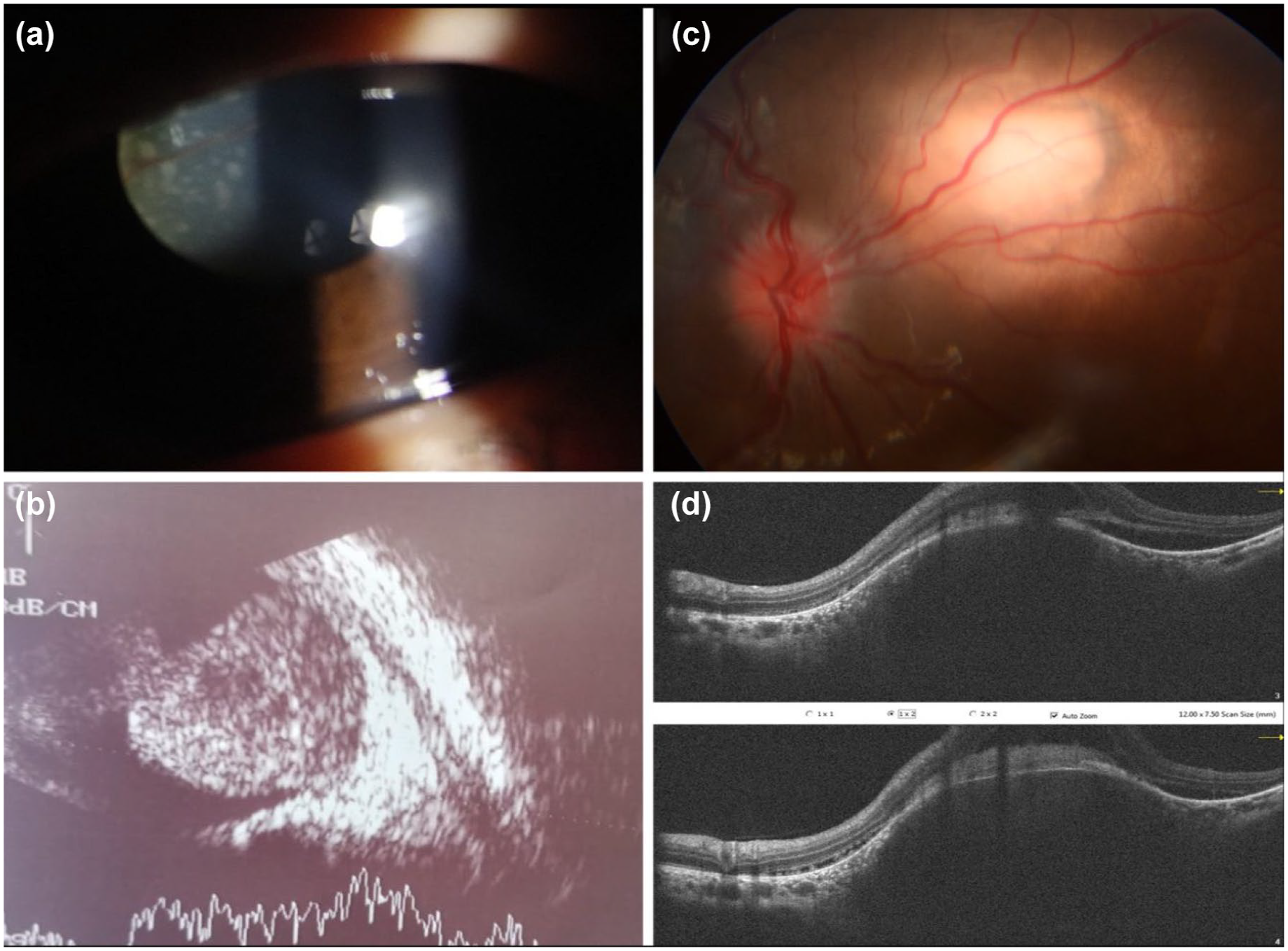
Ocular examination and investigations at the initial presentation. (a) Slit lamp photo of the left eye showing extensively detached retina seen behind the lens, (b) B scan ultrasound of the left eye showing total exudative retinal detachment, exophytic mass (13 mm basal diameter × 11.5 mm height) with heterogenous high internal echogenicity and choroidal excavation, (c) colored fundus photo of the right eye showing upper nasal whitish mass around two disc diameter with surrounding cuff of subretinal fluid and evident hyperemic disc with blurred margins and obliterated cup, (d) OCT line scans over the lesion of the right eye showing dome shaped choroidal elevation with loss of the normal choroidal pattern and overlying subretinal fluid at the edge with loss of the normal structure of the outer retinal layers.
Following an evaluation by ocular oncology and uveitis consultants, the child was urgently referred to the pediatric department. Initial assessment showed stable vital signs; however, her growth parameters fell below average, with a weight of 21 kg (10th–15th percentile) and height of 123 cm (10th–15th percentile) for her age. No abnormalities were detected in her chest auscultation, and abdominal exam, but localized swelling and tenderness were noted above the ankle. She had a lesion on her face in the right zygomatic area. A chest CT scan obtained during her prior admission for pneumonia demonstrated right upper lobar pneumonic consolidation, along with multiple atelectatic bands and subpleural thickening. Brain and orbit imaging (Figure 2) was done on the same day. Multiple scattered supra and infratentorial intraparenchymal hyperdense lesions were seen in the MRI brain with a few ring-shaped lesions. A new chest X ray showed tiny multiple miliary lesions (Figure 2). The child was admitted in the pediatric department, initial laboratory investigations revealed normal CBC with normal liver, kidney functions and electrolytes as shown in Table 1. A lumbar puncture was performed for CSF analysis, and GeneXpert test. The results of the GeneXpert test returned negative after a few hours. Based on the clinical findings, history of TB exposure, and initial imaging results, the child was diagnosed with disseminated tuberculosis. Treatment was initiated the same day with antitubercular therapy (ATT) and intravenous dexamethasone due to associated intracranial lesions.
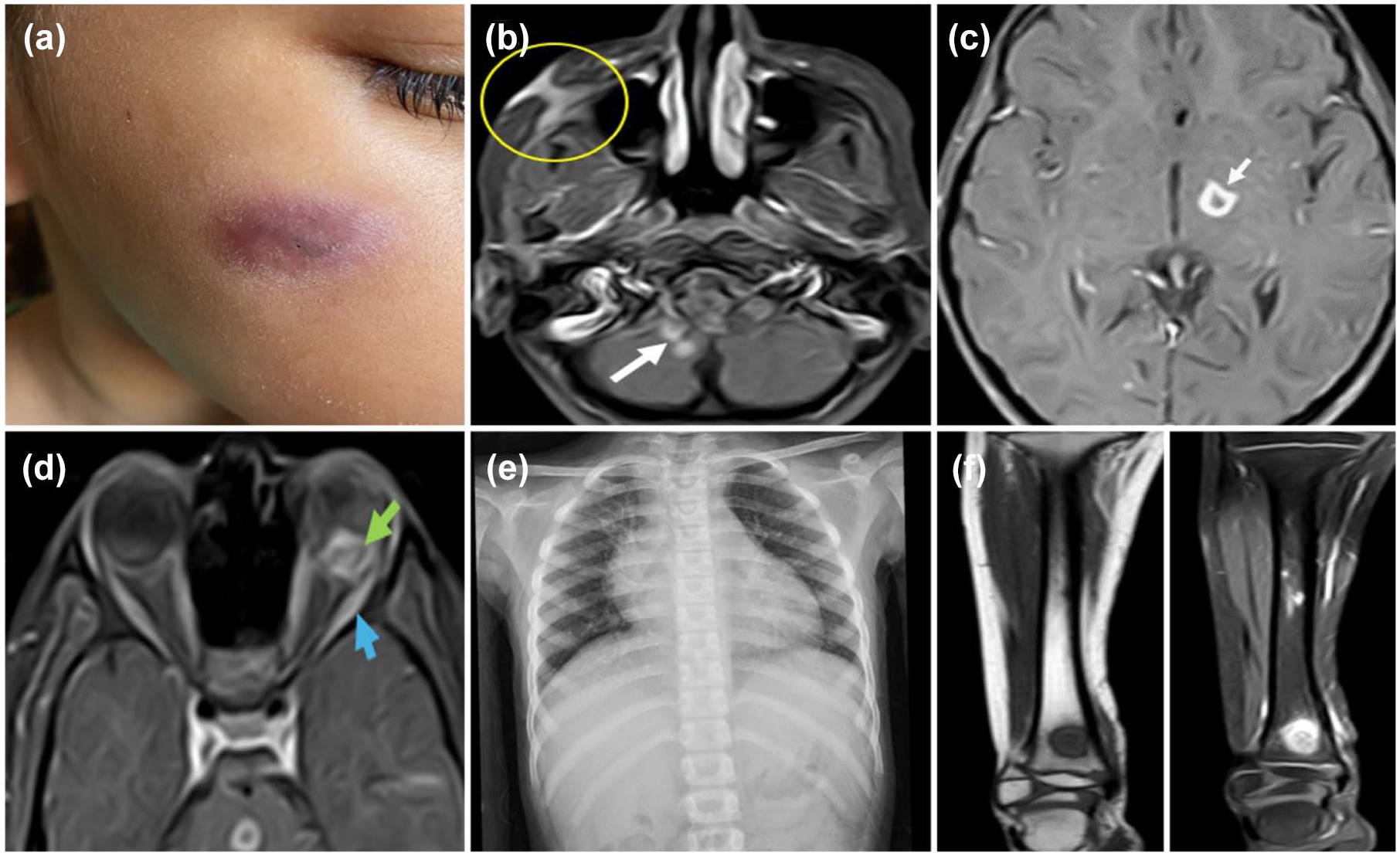
Systemic examination and imaging at the initial presentation. (a) A photo of a chronic wound over the right cheek surrounded by area of bluish discoloration, (b, c) MRI brain T1 weighted images of the brain showing few supra and infratentorial small ring enhancing lesions (white arrows) and right cheek enhancing fistulous tract is noted extending to the right maxillary sinus (yellow circle), (d) MRI orbit T1 weighted images shows intra-ocular peripheral enhancing lesion (green arrows) based on the lower aspect of the left eye globe in addition to swollen and accentuated enhanced extra-ocular muscles (blue arrow), (e) plain chest X ray showing tiny miliary nodules within both lungs, (f) MRI of the right tibia with and without IV contrast, showing the tibial chronic inflammatory lesion.
Summary of the laboratory results on initial presentation.

ALT, alanine aminotransferase; AST, aspartate aminotransferase; BUN, blood urea nitrogen; CSF, cerebrospinal fluid; D, Direct; FBC, full blood count; HB, hemoglobin; INR, international normalized ratio; MCV, mean corpuscular volume; T, Total; TLC, total leucocytic count.
The child was scheduled for further investigations in the next few days. Her investigations showed highly positive tuberculin test (22 mm), positive QuantiFERON, while her viral markers including HIV test were negative. Imaging results are shown in Figure 2 and laboratory results are shown in Table 1. Genetic testing for mycobacterial susceptibility was conducted.
The child was initially admitted for 2 weeks and received standard quadruple ATT. This included a fixed-dose combination tablet containing Isoniazid (10 mg/kg/day; 50 mg per tablet), Rifampicin (15 mg/kg/day; 75 mg per tablet), and Pyrazinamide (30 mg/kg/day; 150 mg per tablet), administered as four tablets daily (total daily dose: Isoniazid 200 mg, Rifampicin 300 mg, Pyrazinamide 600 mg). Additionally, ethambutol (15 mg/kg/day) was prescribed as a water-dispersible tablet formulation dissolved in water. Concurrently, she received intravenous dexamethasone at a dose of 0.4 mg/kg/day, divided every 12 h. After 1 week of intravenous steroid therapy, she was transitioned to oral prednisolone at an equivalent dose (0.4 mg/kg/day). To prevent isoniazid-induced peripheral neuropathy, vitamin B6 supplementation was prescribed. She was enrolled in the Directly Observed Therapy, Short-course program in accordance with guidelines of the Egyptian National TB Program. Regular follow-up visits were scheduled to monitor her systemic and ocular conditions and evaluate for potential medication-related adverse effects, particularly visual acuity changes and color vision abnormalities.
Three weeks later, her ocular condition improved, with a reduction in subretinal fluid around the choroidal mass in the right eye. In the left eye, vision improved from PL to 2/60, along with improvement in the exudative retinal detachment. Five weeks after starting her treatment, fundus fluorescein angiography (FFA) was done (Figure 3). Her facial lesion started to heal with scarring and her tibial lesion markedly improved. The steroid dosage was adjusted for gradual withdrawal, while continuing the anti-tuberculosis therapy.

Colored fundus photo and fundus fluorescein angiography 1 month after starting treatment. (a) Colored fundus photo of the right eye showing upper nasal choroidal tuberculoma and blurred disc margin, (b) FFA showing early hyper fluorescence of the tuberculoma, (c) Montage of the FFA images of the right eye showing pooling around the lesion with hot disc, (d) colored fundus photo of the left eye showing subtotal exudative retinal detachment sparing the area superior to the disc, (e) FFA photo of the superior part showing diffuse pinpoint perivascular leakage, and (f) montage of the FFA images of the left eye showing diffuse perivascular pinpoint leakage with pooling of the dye in the detached retina and diffuse disc leakage.
Two months after her initial presentation and being on treatment, she presented to the ER with severe headache and vomiting. Fundus examination showed extensive disc edema compared to the last fundus imaging. Urgent brain CT scan was done, which showed hydrocephalus. Meanwhile, she started to have fits and deteriorated conscious level. She received intravenous dexamethasone, along with intravenous mannitol to manage raised intracranial pressure while being prepared for surgery. Neurosurgical intervention was urgently done, and a ventriculo-peritoneal shunt was inserted followed by ICU admission. After initial improvement, she complained again of severe headache with deterioration of conscious level. After imaging, she was diagnosed with obstructive non communicating hydrocephalus and another shunt was inserted. She didn’t regain consciousness after the second surgery and her laboratory workup showed electrolyte disturbance and signs of sepsis. A few days later, she died. Genetic test results came back later, no definite molecular cause has been identified.
Discussion
Tuberculosis is a major health issue that can affect nearly all body organs as part of extrapulmonary TB. Cases of infected children below the age of 14 represent 12% of the estimated TB cases worldwide. 7
We report a case of an 8-year-old child who presented to our ocular oncology service with leukocoria. Tumors, especially retinoblastoma, are among the leading suspected causes in cases presenting with leukocoria. Congenital malformations, vascular diseases, phakomatoses, inflammatory lesions, retinal detachment, and congenital cataract may all present with leukocoria. 8 The primary differential diagnosis for our patient included acquired inflammatory lesions (tuberculosis), late retinoblastoma, and choroidal tumor.
As previously reported by Shields et al., late retinoblastoma after the age of 5 years represents 8.5% of patients diagnosed with retinoblastoma. 9 In their case series, all children with late retinoblastoma presented with unilateral disease. In our patient, using OCT, the right sided lesion was shown to be choroidal with overlying subretinal fluid. Thus, eliminated the possibility of being retinoblastoma, however, theoretically it could be metastatic choroidal lesion from retinoblastoma in the left eye. Choroidal invasion has been previously documented in cases of retinoblastoma, with or without optic nerve involvement; however, such occurrences have been limited to the affected eyes diagnosed with retinoblastoma. 10
Another possibility was a choroidal tumor, either as a primary choroidal melanoma or an intraocular metastasis. However, choroidal melanoma is rare in this age group and is more likely to be melanotic. Masoomian et al. in their multicenter study reported the characteristics of 66 pediatric patients with choroidal melanoma. In their study, 82% of the cases were melanotic lesions. 11 Our patient has no known risk factor for ocular melanoma like ocular and oculodermal melanocytosis, familial melanoma, and neurofibromatosis type 1. 12 Also, the lesions were bilateral and amelanotic.
Choroidal metastases are another rare clinical manifestation, particularly in pediatric patients. To date, all reported cases in the literature have been unilateral and associated with neuroblastoma or carcinoid tumors.13,14
In the present case, initial imaging studies did not reveal lesions indicative of malignancy; rather, they suggested a chronic inflammatory etiology. A comprehensive evaluation incorporating the patient’s family history of TB and prior pneumonia strongly indicated disseminated TB (encompassing pulmonary and extrapulmonary involvement) as the most probable diagnosis. Accordingly, her ocular presentation was diagnosed as bilateral TB choroiditis with tuberculomas, aligning with the standardized nomenclature for ocular TB phenotypes. 15
Despite multiple CNS tuberculomas, our patient had a normal CSF analysis—a finding previously reported in the literature. Thomas et al. reported typical CSF abnormalities in only 66% of 111 TB meningitis cases. 16 CNS TB may present as diffuse meningitis, localized tuberculomas, abscesses, or spinal involvement. Our patient’s silent tuberculomas likely reflect early-stage disease, similar to two cases described by Deif et al., 17 who initially had normal CSF and were later diagnosed with CNS TB.
A multicenter study by Chu et al. in China evaluated 4654 pediatric TB patients (<18 years), comprising 54.23% pulmonary TB, 17.76% extrapulmonary TB, and 28% combined pulmonary/extrapulmonary TB. Among extrapulmonary TB cases, tuberculous meningitis (34.18%) was the most prevalent subtype, while disseminated TB was documented in 11.13% of the cases; ocular TB was not specifically assessed. 18
Kaur et al. conducted a retrospective study in North India evaluating the clinical features and outcomes of 32 pediatric patients (<16 years) with TB-associated uveitis. Posterior uveitis and panuveitis were the most common presentations (43.75% each), followed by intermediate and anterior uveitis (6.25% each). Despite ATT and corticosteroids, nearly 30% of patients exhibited inadequate treatment response or disease progression, necessitating adjunctive immunosuppressive therapy. 19
The patient was managed with anti-tuberculosis therapy and systemic corticosteroids, adhering to established treatment protocols for central nervous system TB. 20 After initiating treatment, our patient exhibited early clinical improvement with a management plan involving a 1-year ATT regimen. However, her condition worsened due to hydrocephalus, with further deterioration after her second neurosurgical intervention. She later developed sepsis and ultimately succumbed to sepsis-related complications. Reported mortality rates from disseminated TB is still high, ranging from 25% to 30%. 21 In 2022, an estimated 214,000 children and young adolescents (under 15 years) died from TB, equating to nearly 600 young lives lost every day to this preventable disease. 1
This case study highlights the potential for ocular TB lesions to serve as the initial indication of disseminated TB. We present a rare manifestation involving bilateral choroidal tuberculomas that clinically mimicked intraocular tumors. Through the integration of multimodal ocular imaging alongside systemic laboratory and radiological assessments, an accurate diagnosis was established. Notably, this case occurred despite the well-structured Egyptian National TB Program and its commendable efforts in prevention, early diagnosis, and management of TB—underscoring that gaps in awareness and delayed recognition can still lead to neglected or advanced presentations. Emphasizing education and proactive screening among the families and close contacts of TB patients remains essential for timely detection and effective management.
Supplemental Material
sj-pdf-1-oed-10.1177_25158414251356373 – Supplemental material for Bilateral intraocular masses in a child as a first presentation of disseminated tuberculosis: case report
Supplemental material, sj-pdf-1-oed-10.1177_25158414251356373 for Bilateral intraocular masses in a child as a first presentation of disseminated tuberculosis: case report by Doaa Maamoun Ashour, Nada Abdel Salam Abdel Aziz, Khadiga Eltonbary, Noha Abdul Khaliq and Yasmeen Abdelaziz Fereig in Therapeutic Advances in Ophthalmology
Footnotes
Acknowledgements
We would like to thank Dr Manar Ashour, Radiology department, Ain Shams University for her effort in interpretation of the imaging results of our patient.
Author’s note
Part of the data presented in this report was presented as oral presentation by Dr Doaa Ashour, in the annual meeting of the Egyptian Vitreoretinal Society (EGVRS), Luxor, Egypt, 2024.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.