
Abstract
Introduction:
To enhance recovery, we can use short acting agents and monitor depth of anaesthesia. Desflurane is less soluble in blood and has good emergence characteristics. Traditionally, MAC was used to assess the depth of anaesthesia and to aid in recovery from anaesthesia. Recently, Bispectral index (BIS) monitor has gained popularity for monitoring the depth of anaesthesia. The present study aims to compare the efficacy of BIS and corrected MAC as monitors for the depth of anaesthesia and the recovery profile of patients undergoing surgery under general anaesthesia
Patients and Methods
A prospective randomised comparative double blinded study was conducted. Sixty patients in the age group of 18–65 years were scheduled for mastectomy surgery under general anaesthesia with ASA grade 1 and 2 were included in the study and were randomly divided into two groups.
Group B:
Desflurane concentration was adjusted to maintain a BIS value of 45–55.
Group M:
Desflurane concentration was adjusted to maintain a target age-corrected MAC of 0.8–1.3
Results:
Patients monitored with BIS had faster awakening and less consumption of desflurane.
Conclusion:
With the use of BIS monitor, there is less anaesthetic gas consumption and early recovery from anaesthesia, which makes it a superior choice for monitoring the depth of anaesthesia.
Introduction
Recovery is a state of consciousness of a person when he is awake and aware of himself and things around him.[1,2] Patients usually respond to verbal stimuli when alveolar anaesthetic concentration is decreased to about 30% of minimum alveolar concentration (MAC), if unimpeded by other factors.[2]
For early emergence, we can monitor the depth of anaesthesia and use short acting agents.[3] As desflurane is less soluble in blood, it is associated with early emergence.[4]
Achieving adequate depth of anaesthesia during surgical procedures is desirable. While a deep level of anaesthesia results in cardiovascular depression, a lighter plane of anaesthesia can be frightening from the patient’s point of view.
Awareness may have psychological sequelae for the patient, which may include: insomnia, depression, anxiety and post-traumatic stress disorder (PTSD) with distressing flashbacks.[5] The majority of patients who have suffered intraoperative awareness fear future surgery.[6]
There are various methods to monitor the depth of anaesthesia. Traditionally, MAC was used to assess the depth of anaesthesia and to aid in recovery from anaesthesia. Volatile anaesthetic agents are titrated to maintain an adequate depth of anaesthesia according to their MAC value and hemodynamic response.
Nowadays, Bispectral index (BIS) monitor is commonly used to monitor the depth of anaesthesia. There are studies which have demonstrated earlier recovery from general anaesthesia with the use of BIS monitoring.[7-9]
The present study aims to compare the efficacy of BIS and corrected MAC as the monitors for the depth of anaesthesia and the recovery profile of patients undergoing surgery under general anaesthesia.
Material and Methods
Sample Size
R Sudhakaran et al.[3] conducted a study in 90 patients randomised in 3 groups and found that emergence time and time to extubation in BIS guided anaesthesia and ETAC guided anaesthesia was less than the standard clinical protocol group. It was found that emergence time (mean ±SD) in ETAC was 5.1± 1.53 min and in BIS was 5.0 ± 2.12 min. Taking these values as reference, the minimum required sample size with 80% power of study and 5% level of significance is 5,359 patients in each group. For a finite sample size, taking the population as 60, the total sample size calculated is 60. So the total sample size taken was 60 and the patients were randomised in two groups.
A prospective, randomised, comparative and double blinded study was conducted in the Department of Anesthesiology, Fortis Hospital, Mohali. Sixty patients in the age group of 18–65 years scheduled for mastectomy surgery under general anaesthesia with ASA grade 1 and 2 were included in the study and were randomly divided into two groups. Patients were randomised to Group B (BIS-control) and Group M (MAC-control) prior to surgery.
On arrival in the operating room, standard ASA monitors and BIS sensor (COVIDIEN BIS LoC 2 Channel) were applied.
Anaesthesia was induced with injection Fentanyl 2 mcg/kg, injection Propofol 1.5–2.5 mg/kg and injection Rocuronium 0.6 mg/kg, intravenously. After intubation and confirming bilateral air entry, lungs were ventilated with Desflurane in oxygen: air mixture of 50:50 at the rate of 10–12 breaths per minute with tidal volume of 4–6 ml/kg and PEEP of around 5 cms of water was added to maintain EtCO2 30–35 mmHg.
Low flow anaesthesia was used with a total fresh gas flow of 500ml/min. End tidal control mode was used in all the patients, which guarantees the set values of end tidal anaesthetic and oxygen concentration.
Neuromuscular blockade was maintained with intermittent doses of injection Rocuronium 0.15 mg/kg to keep train-of-four count of 2.
The bispectral index values, end tidal anaesthetic agent concentration, MAC and haemodynamics were recorded in both the groups at every 5 minutes after the zero time (10 minutes after induction) by another independent person.
A 20% increase from baseline blood pressure or heart rate, patient movement, grimacing, lacrimation or sweating during the maintenance period was defined as inadequate anaesthesia. Any sign of inadequate anaesthesia, despite the lowest target value of BIS or highest target value of MAC, was treated with injection Fentanyl 0.5 μg/kg intravenously.
Any episode of decrease in blood pressure (MAP less than 20% of baseline) or decrease in heart rate (heart rate <50/min or lower than 20% of baseline) despite achieving highest target value of BIS or lowest target value of MAC was treated with injection Mephenteramine 6mg intravenously or injection Atropine 0.6 mg intravenously, respectively.
When closure was initiated, concentration of Desflurane was adjusted to lowest target MAC, that is, 0.8 MAC in group M and to highest BIS target value, that is, 55 in group B.
Injection Paracetamol 15mg/kg was given intravenously to all the patients.
At the end of procedure, Desflurane was discontinued and fresh gas flow was increased to 6 l/min.
Neuromuscular blockade was reversed with injection Neostigmine 0.05 mg/kg and injection Glycopyrrolate 0.01 mg/kg.
Patient was extubated when adequate reversal of neuromuscular blockade was achieved and when the patient was able to open eyes spontaneously or on verbal commands.
During emergence, hemodynamic parameters, ETAA, MAC and BIS were noted every 1 minute.
During emergence, time to spontaneous respiration, time to eye opening spontaneously or on verbal commands and extubation time were assessed every 1 minute.
Time from discontinuation of anaesthetic agent to eye opening, spontaneously or on verbal commands, was the emergence time.
Time from discontinuation of anaesthetic agent till extubation was the extubation time.
Total anaesthetic gas consumption in the surgery was noted.
Patients were assessed for their level of sedation (using Brussels Sedation Scale) and severity of pain (using VAS), once in the operation theatre before being shifted to PACU, and then after 1 hour after PACU admission.
Post-operative, VAS score >3 was treated with injection Tramadol 1–2 mg/kg intravenously.
Post-operatively after 24 hours, patients were questioned for any incidence of intraoperative awareness using Modified Brice Interview.
The following measures were assessed and recorded:
Blood pressure, heart rate and SpO2 were measured in preop (baseline) before induction and 10 minutes after intubation. EtCO2, MAC, BIS and EtAA were measured every 5 minutes till the start of skin closure and at every 1 minute after the discontinuation of the volatile anaesthetic gas till emergence and at extubation. Emergence time. Extubation time. Requirement of intra-operative analgesics. Sedation score after extubation and one hour post-operatively. Pain score after extubation and one hour post-operatively. The occurrence of any adverse events, including hypotension or bradycardia Analgesic requirement post-operatively. Total anaesthetic gas consumption. Incidence of intraoperative awareness.
Results and Observations
In our study, the demographic characteristics such as age, sex, height, weight and BMI of the patients in both the groups were comparable. There was no statistically significant difference in the ASA grade of the patients and duration of the surgery between the two groups.
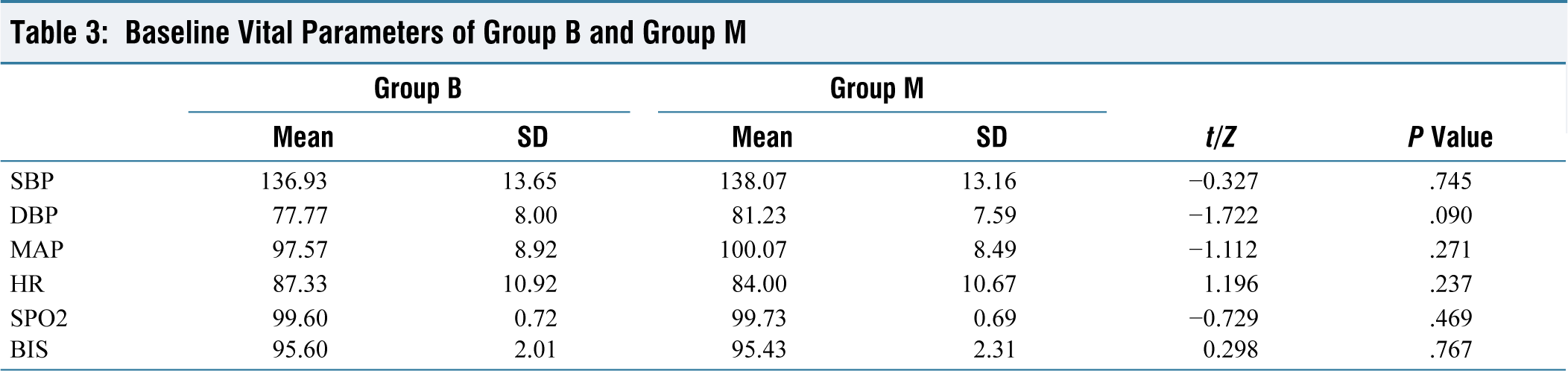
Baseline hemodynamic parameters (SBP, DBP, MAP, HR, SpO2) were comparable in both the groups (Tables 1–3).
Distribution of Age (Years) Between Group B and Group

Distribution of Height (cms), Weight (kgs), Body Mass Index (kgs/m2) Between Group B and Group M

Baseline Vital Parameters of Group B and Group
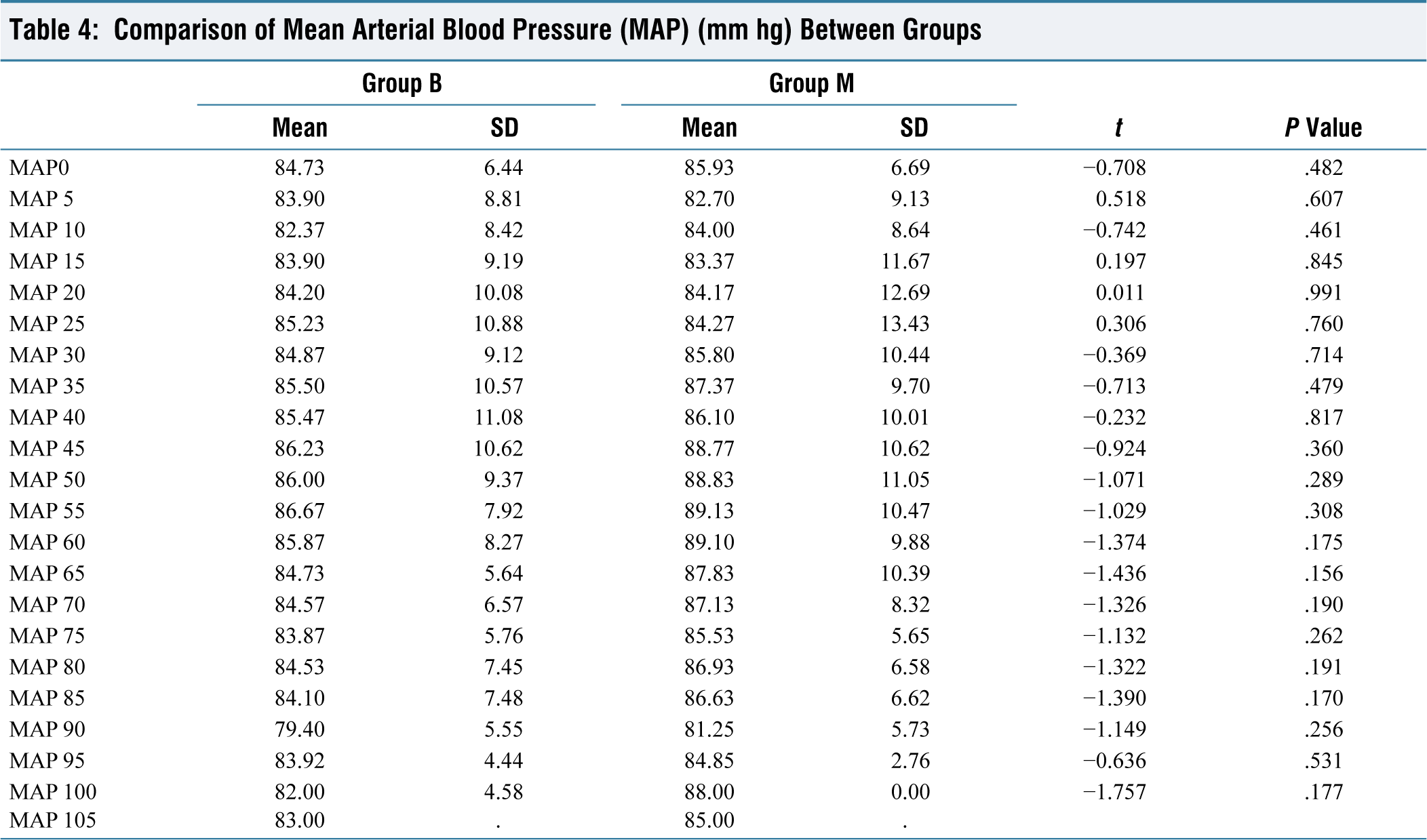
Intraoperatively, hemodynamic parameters (SBP, DBP, MAP, HR, SpO2, EtCO2) were comparable in both the groups (Table 4).
Comparison of Mean Arterial Blood Pressure (MAP) (mm hg) Between Groups
There was no significant difference in intraoperative and post-operative analgesic requirement between both the groups. Also, there was no significant difference in post-operative sedation and post-operative incidence of nausea or vomiting between both the groups (Tables 5–7).
Comparison of Intraoperative Analgesia Requirement Between Group B and Group

Comparison of Need for Any Rescue Analgesia Between Group B and Group

Comparison of Nausea or Vomiting (N or V) Between Group B and Group

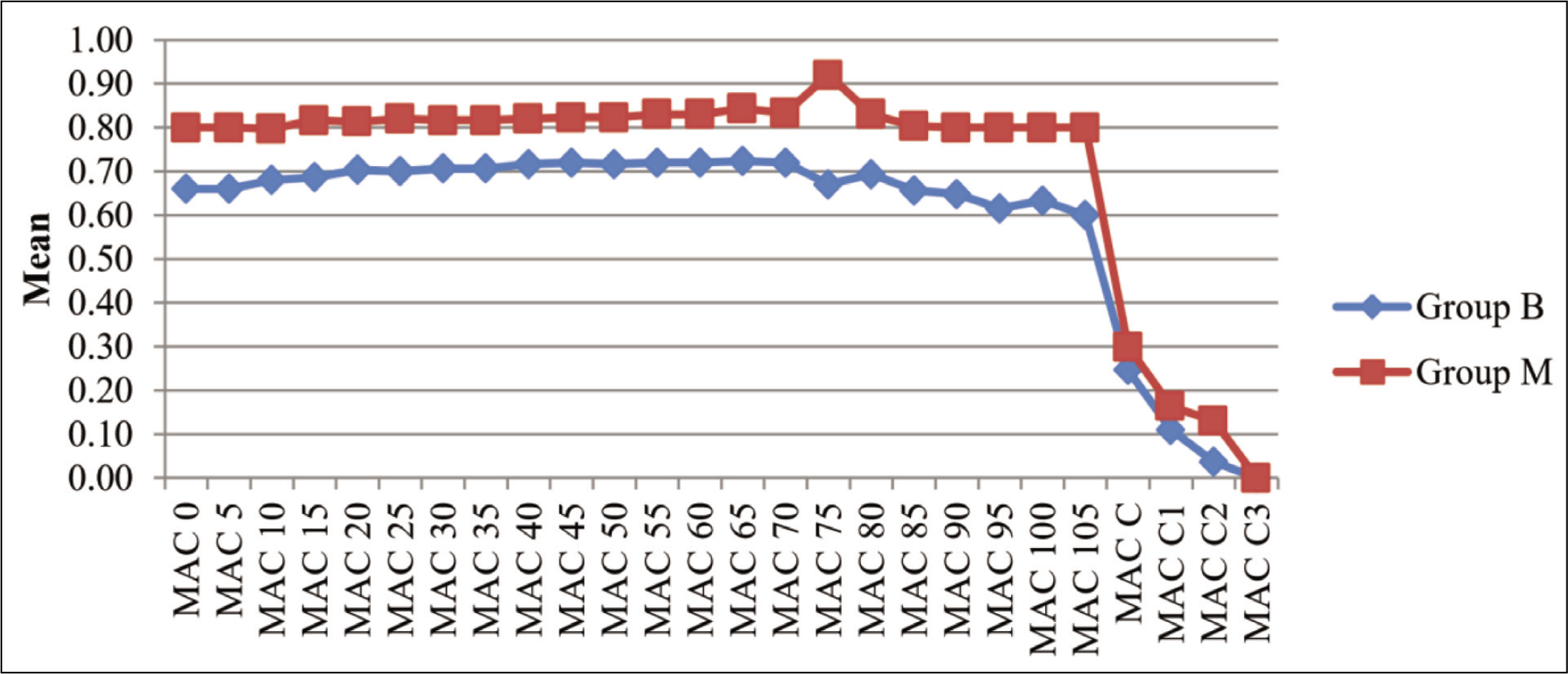
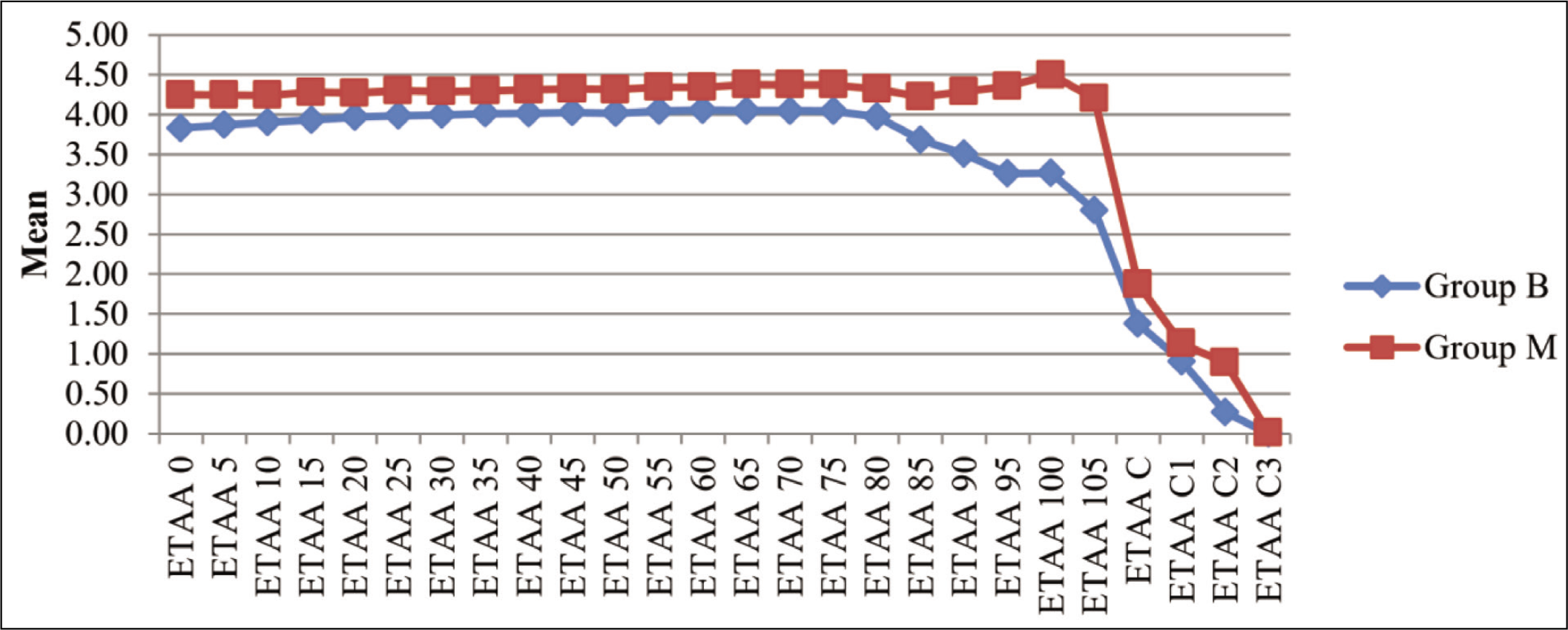
The intraoperative MAC and ETAA values monitored at 5 minutes interval during the surgery were less in group B as compared to group M, and the difference was statistically significant (Figures 1 and 2).
Comparison of Minimum Alveolar Concentration (MAC) Between Group B and Group M (P < .05)
Comparison of End Tidal Anaesthetic Agent Concentration (EtAA) Between Group B and Group M (P <.05)
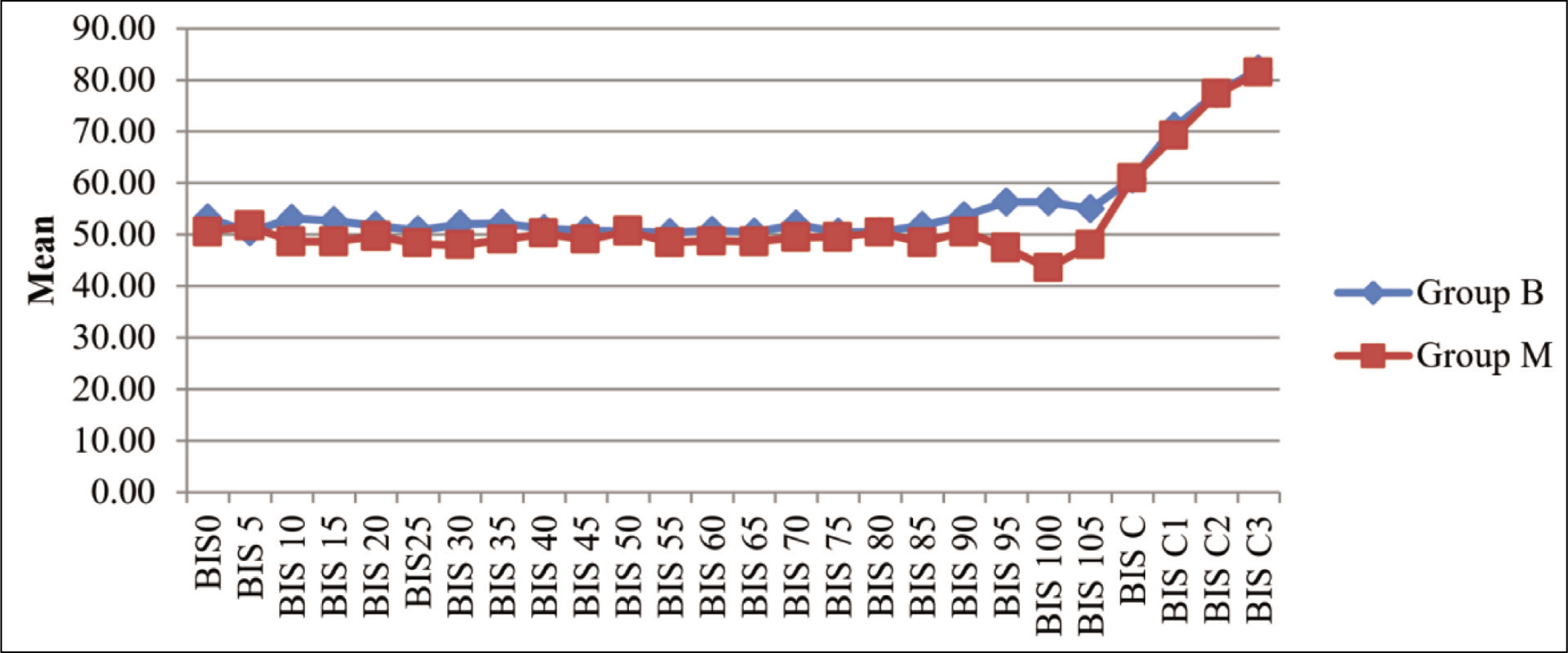
The intraoperative BIS values during the surgery in group M were at times less as compared to group B, and the difference was statistically significant. However, the BIS values remained within the target range of 45 to 55 at all times (Figure 3).
Comparison of Bispectral Index (BIS) Between Group B and Group M (P < .05)
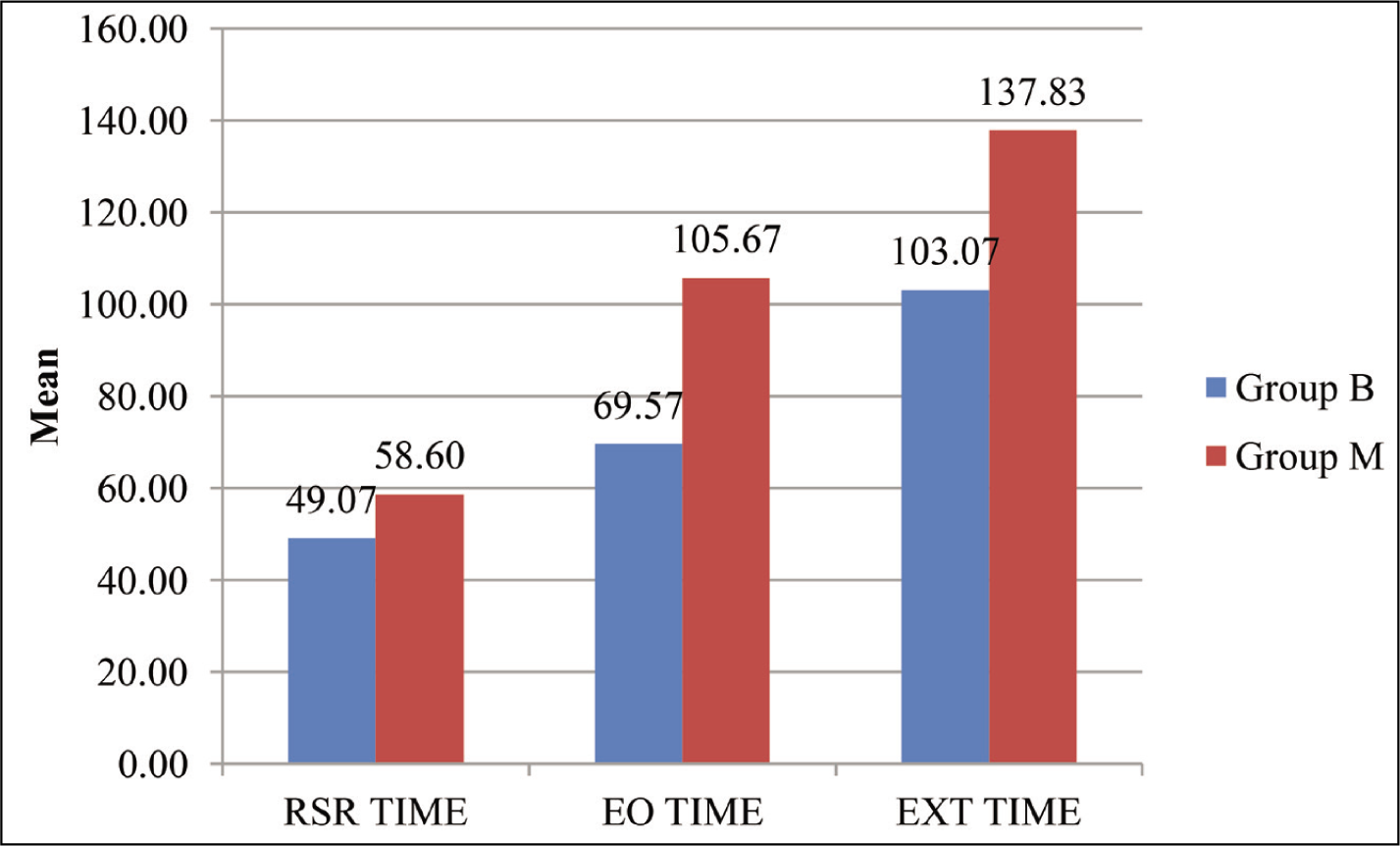
Comparison of time to eye opening and time to return to spontaneous respiration was significantly less in group B as compared to group M (Figure 4).
Comparison of Time to Return of Spontaneous Respiration (Seconds), Time to Eye Opening (Seconds) and Time to Extubation (Seconds) Between Group B and Group M (P < .05)
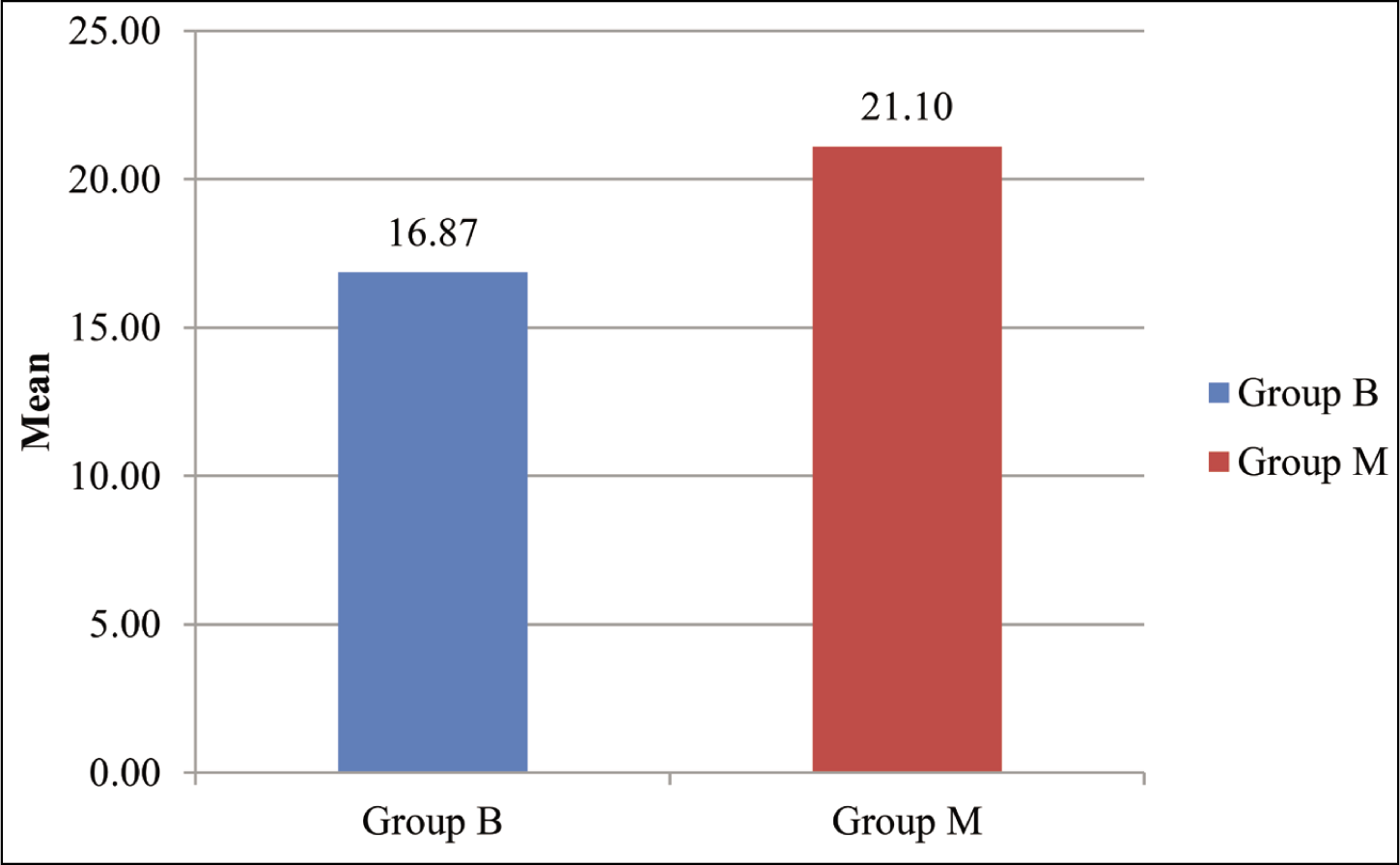
Comparison of total gas consumption between group B and group M revealed that consumption in group B was significantly less than in group M (Figure 5).
Comparison of Total Gas Consumption (TGC) (ml) Between Group B and Group M (P < .05)
Discussion
Various studies have been done, which have shown that MAC and ETAA monitoring and BIS monitoring are better in maintaining adequate depth of anaesthesia and in achieving early recovery from anaesthesia as compared to anaesthesia guided by clinical parameters only.[3]
A few studies have compared MAC and BIS as monitors for the depth of anaesthesia and early recovery from anaesthesia with conflicting results.[10-12]
The present study was aimed to compare the efficacy of BIS monitoring and age corrected MAC monitoring on the recovery time from general anaesthesia using Desflurane.
The inference we get from our study is that adequate depth of anaesthesia as depicted by BIS values between 45 to 55 was maintained with relatively lesser doses of inhalational agent as depicted by lesser values of ETAA and MAC in group B at all times as compared to group M. Administering just the right amount of anaesthetic agent, titrated according to the individual‘s requirement, leads to early recovery from anaesthesia as depicted by the shortened emergence time and time to extubation in group B as compared to group M. This also results in lesser consumption of anaesthetic agent in group B as compared to group M.
Our results were in accordance with the study done by Shukla U et al.[10] in patients undergoing elective surgery under general anaesthesia lasting up to 120 minutes using Sevoflurane. They found that the mean time to extubation was significantly shorter in the BIS guided group as compared to the end tidal gas concentration guided group. Also, the consumption of Sevoflurane was significantly less in the BIS group.
Similarly, a study done by Sadek S et al.[13] supported our present study in which BIS guided anaesthesia was compared with MAC guided anaesthesia. They found that in the BIS guided group there a was shorter time to eye opening, to follow commands and to tracheal extubation, and less anaesthetic gas consumption as compared to MAC guided group.
A study conducted by Nair et al.[11] in patients undergoing breast surgery under general anaesthesia found that the time to extubation is significantly less in BIS guided anaesthesia as compared to MAC guided anaesthesia. Also, the consumption of Sevoflurane was significantly less in BIS guided anaesthesia. The results of this study supported our study.
With the use of a lesser amount of anaesthetic agent, intraoperative awareness remains a concern. However, in our study there was no incidence of intraoperative awareness in both the groups. Similar results were found in a study done by Avidan MS et al.[14] in 2000 patients with no significant difference in intraoperative awareness in BIS guided anaesthesia and ETAG guided anaesthesia.
Contrary to these studies, a study done by Jain N et al.[12] with Halothane found that the time to extubation was significantly more in BIS guided anaesthesia as compared to ETAG guided anaesthesia. As BIS is specific for each inhalational agent, the difference in their outcome could be due to the use of Halothane. The drug specific changes in BIS values were found in a study conducted by Banerjee N et al.[15] They compared BIS values of Halothane, Isoflurane, Sevoflurane and Desflurane at equivalent MAC concentrations and found that at 1 MAC, Halothane has significantly higher BIS values as compared to Isoflurane, Sevoflurane and Desflurane.
It was also noted in a study conducted by Kim JK et al.,[16] who compared the relationship of BIS with equivalent MAC values of Sevoflurane, Isoflurane and Desflurane and noted that Desflurane produces significantly low BIS values as compared to Sevoflurane at equivalent MAC.
Some studies have shown no significant difference between the BIS guided and MAC guided anaesthesia. A study conducted by Villafranca A et al.[17] noted that there was no significant difference in time to extubation in patients undergoing fast track cardiac surgery in both BIS guided group and ETAC guided group. Similar results were noted in a study conducted by Vance JL et al.[18] on patients undergoing elective coronary bypass graft surgery. They found no significant difference in time to extubation and length of stay in ICU in BIS and ETAG groups. In both these studies, patients were not extubated in the immediate post-operative period and were monitored in ICU for a few hours before extubation, where the sedation was not titrated on the basis of BIS and ETAA. This could lead to results being comparable in both the groups.
Conclusion
Both BIS and MAC are useful for monitoring the depth of anaesthesia as there was no incidence of intraoperative awareness in both the groups. However, with the use of BIS monitor, there is less anaesthetic gas consumption and early recovery from anaesthesia, which makes it a superior choice for monitoring the depth of anaesthesia. Maintaining just adequate depth of anaesthesia can lead to more stable hemodynamics in patients with compromised cardio respiratory functions and early recovery in desired patients, such as obese patients, airway surgeries, etc. Also, lower consumption of anaesthetic agent can lead to decreased cost, which can be further evaluated in further studies.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
IEC/2021/TH/16.
Informed consent
Patient consent has been obtained.
Credit author statement
We hereby state that the manuscript has been read and approved by all the authors. This manuscript represents honest work. The contents have not been published elsewhere. As this was an observational study, it was not registered with Clinical Trials Registry.
Guneet Kaur contributed in acquisition and interpretation of data.
Jasmeet Kaur conceptualised and designed the study and supervision of Guneet.
Arvinpreet Kour helped in the proof reading and gave valuable inputs in the article.
Akashdeep Singh helped in drafting of the article, revising it critically and provided final approval for the version to be published with all the modifications.
Preeti Adlakha helped in the proof reading and gave valuable inputs in the article.
Data availability
Not applicable.
Use of artificial intelligence
The use of artificial intelligence is not relevant to this article.