
Abstract
Background:
The temporal lobe is an intricate brain structure with unique features, playing a key role in auditory perception. The connection between abnormalities in the temporal lobe and hearing loss is a significant sensory disruption in the human brain.
Methods:
This review article offers an in-depth analysis of the temporal lobe’s anatomy, physiology and functions, highlighting its involvement in hearing impairment. This analysis draws from a review of various significant research articles on temporal lobe dysfunction, along with a clear and concise overview of the temporal lobe’s structure and functions with respect to hearing.
Results:
The temporal lobe is a crucial component of the human brain. It has an important function for hearing along with several cognitive processes such as information processing. This review article also explores the connection between abnormalities in the temporal lobe and hearing loss, providing compelling evidence that irregularities in the temporal lobe are linked to auditory impairments.
Conclusion:
In routine clinical practices, physicians often face challenges in managing temporal lobe diseases because of limited resources, insufficient comprehensive data, healthcare access disparities and insufficient neuro-auditory assessments. Holistic management needs an understanding of patients’ hearing impairment and temporal lobe lesions. Further research is required for a proper understanding of the temporal lobe functions, healthcare gaps and enhanced healthcare technology.
Introduction
Hearing impairment in the later part of life is a major clinical concern and a leading association of poor cognitive function and is even associated with dementia.[1] The temporal lobe is a vital part of the brain that plays a significant role in hearing.[2] The temporal lobe is the area of the brain where sound is processed and, not surprisingly, it is also an area where auditory language and speech comprehension systems are situated. The auditory cortex is located on the upper edges of the temporal lobe, within the Sylvian fissure.[3] Hearing impairment in an elderly individual is related to a lower volume of grey matter in the auditory cortex of the temporal lobe.[4] The rapid reduction in grey matter volume in the right temporal lobe is associated with age-related hearing loss.[4] Lesions in the primary auditory cortex of the temporal lobe lead to cortical deafness, which has a poor functional outlook and few treatment options.[4] Speech therapy and rehabilitation are recommended to help improve communication skills in patients with cortical deafness.
Methods of Literature Search
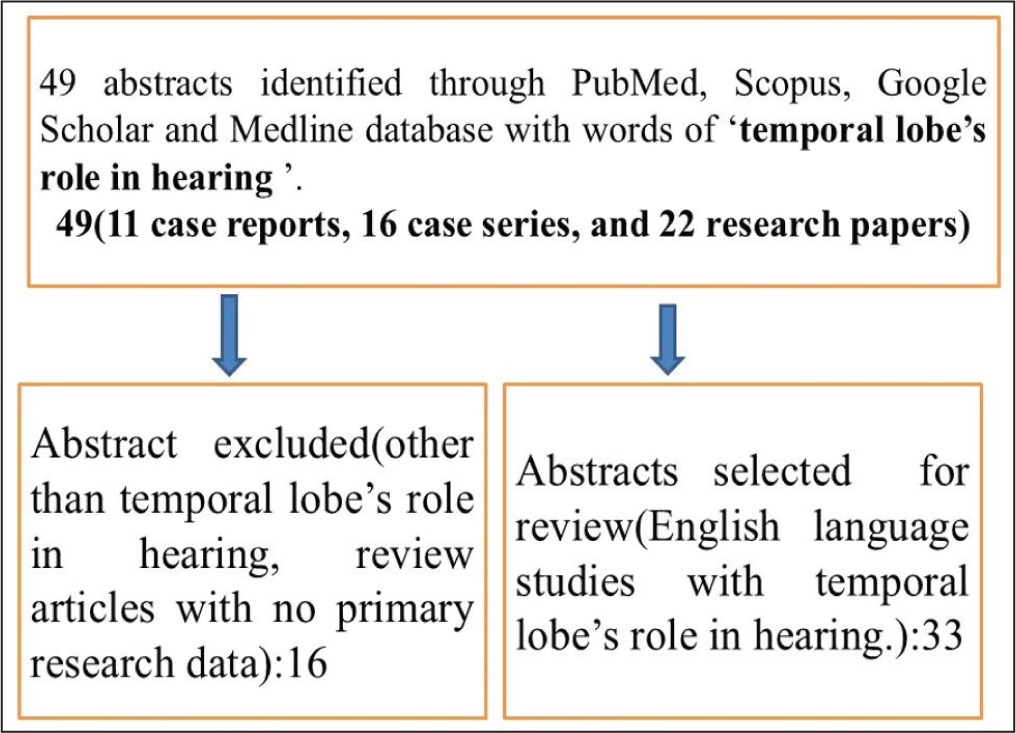
The search was done for recent research articles on the temporal lobe’s role in hearing. First, we conducted a search of the PubMed, Scopus, Medline and Google Scholar databases online. We developed our search strategy based on the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The published works’ abstracts were identified by our search method, although more research publications had to be manually located from the citations. A variety of study designs were looked at, such as case reports, case series, comparative studies, observational studies and randomised controlled trials. There were 11 case reports, 16 case series and 22 research articles in all [Figure 1]. This review article focuses only on the temporal lobe’s role in hearing. A better understanding of the temporal lobe’s role in hearing is provided by this review analysis. It will also catalyse further study and better understanding of the temporal lobe’s role in hearing which is helpful for early detection and treatment of cortical deafness.
Method of literature search
Epidemiology
Hearing loss is a significant public health issue that results in communication challenges and is linked to a lower quality of life.[5] According to the Global Burden of Disease Study, hearing loss ranks as the fourth leading cause of disability worldwide.[6] The prevalence of hearing loss increases with age, impacting approximately 42% of individuals over 50 years old, and rising to 71% among those over 70 years.[7] Age-related hearing impairment impacts almost all individuals over 70, progressing more quickly and primarily affecting higher frequencies.[8] Chronic and progressive hearing loss typically affects communication with the involvement of speech recognition.[9] The decline of central auditory system or temporal lobe auditory cortex occurs due to peripheral auditory system dysfunction that contribute very limited success for intervention. Age-related hearing impairment usually affects older people with reduced hearing thresholds and speech discrimination affecting communication and quality of social life.[10]
Neuroanatomy of Temporal Lobe
Only primates have temporal lobe in the brain, that is the largest in human, accommodating 17% of the cerebral cortex.[11] The temporal lobes include auditory, olfactory, vestibular, visual and linguistic functions.[11] The temporal lobe of the brain can be categorised into its classic Brodmann areas, which include the superior, middle and inferior temporal gyri, as well as the parahippocampal and entorhinal gyri, and the fusiform gyrus.[11] Eight cognitive domains can be observed through functional imaging, along with their corresponding areas in the temporal lobe: speech perception, production and hearing (all in the posterior superior temporal gyrus); episodic memory (in medial structures); semantic processing (in the ventral temporal lobe); social cognition (in two regions of the temporal lobe); and visual processing (at the temporal-occipital junction).[12] The temporal lobe is connected by several important association fibre tracts, such as the uncinate fasciculus, inferior longitudinal fasciculus, inferior frontal-occipital fasciculus, middle longitudinal fasciculus, arcuate fasciculus and cingulum. It also contains two main commissural fibres: the corpus callosum and the anterior commissure.[13] The amygdala, situated in the medial temporal lobe, is made up of nuclei that can be divided into three categories: the basolateral amygdala group (which includes the lateral, basal and basomedial nuclei), the cortical group (consisting of the cortical nuclei and the nucleus of the lateral olfactory tract) and the centromedial group (which encompasses the medial and central nuclei).[14] The amygdala is essential for processing fear and also contributes to a range of emotional functions, such as anxiety, reward processing, reward learning and motivation, as well as drug addiction. Furthermore, it is also associated with aggression, maternal behaviours, sexual behaviours and ingestive behaviours like eating and drinking. The hippocampus, located deep within the medial temporal lobe, is essential for forming declarative memories. Declarative memory encompasses both episodic and semantic types. Episodic memory refers to ability to recall specific events from the past, including their particular time and place. The human primary auditory cortex is located on the superior surface of the temporal lobe in an area known as Heschl’s gyrus. This gyrus is typically longer and wider in the left hemisphere compared to the right.[15] Wernicke’s area is a component of the temporal lobe that helps to understand and form meaningful sentences.
Auditory Cortex
The auditory cortex is situated deep within the Sylvian fissure, in the upper part of the temporal lobe. It includes both primary and secondary auditory regions, along with four separate auditory fields.[16] The primary auditory cortex, known as area AI, corresponds to Brodmann area 41, while the secondary auditory cortex, AII, is identified as Brodmann area 42, located at the back of the superior temporal gyrus. Nearby, Wernicke’s area, also known as Brodmann area 22, is responsible for language comprehension.[16] The arcuate fasciculus connects the auditory association areas in the inferior parietal lobe to the pars triangularis of the frontal operculum, where Broca’s area, which includes Brodmann areas 44 and 45, is involved in expressive language and music perception.[16]
Anatomical Relations of the Temporal Lobe with Hearing
The temporal lobe is situated in the middle cranial fossa, which is bounded in the front by the greater wing of the sphenoid bone, below by the upper surface of the petrous portion of the temporal bone, and on the sides by the squamous part of the temporal bone and the adjacent parietal bone. The tentorium cerebelli is located beneath the posterior and medial parts of the temporal lobe, with its free edge positioned beneath the anterior end of the parahippocampal gyrus. It lies laterally to the uncus and the posterior entorhinal sulcus, forming a subtle indentation referred to as the intrahinal sulcus.[17]
Importance of Studying Temporal Lobe Disorders
The temporal lobe is commonly called the neocortex of brain.[18] It forms part of the cerebral cortex, which also includes the occipital, parietal and frontal lobes.[18] The temporal lobe is seen in the middle cranial fossa, positioned beneath the lateral fissure, also known as the Sylvian fissure or lateral sulcus.[18] It is divided into three sections: the superior temporal lobe, the middle temporal lobe and the inferior temporal lobe.[18] Temporal lobe of the brain consists of many key brain structures, such as the auditory cortex, hippocampus and amygdala. The auditory cortex (Area 41) is located in the upper temporal gyrus, while the rest of the temporal lobe consists of association areas.[19] The auditory cortex features a tonotopic map that represents the audible frequency spectrum, with high frequencies positioned medially and low frequencies laterally. Neural pathways from the medial geniculate nucleus of the thalamus connect to the auditory cortex through the auditory radiations.[19] The primary auditory cortex receives neural inputs from both ears. Its role is generally well recognised in sound perception and sensory memory, with more advanced cognitive processes occurring at higher levels of brain organisation. So, a lesion in the temporal lobe does not lead to contralateral deafness in the same pattern as an occipital lesion results in contralateral vision loss.[18] The temporal lobe is regarded as “polysensory” because it integrates auditory, sensory, visual and limbic functions.[19] The auditory pathway culminates in the temporal lobe (both the primary and secondary auditory cortex) after traversing various peripheral and central components of the auditory system. To analyse information processes for auditory pathways, it is essential to maintain the anatomical and functional integrity of all these structures.[19] Neuronal loss in temporal lobe can lead to challenges in mentally processing auditory information, which may impair patients’ hearing and communication abilities.[19] Cortical deafness is an uncommon condition that primarily occurs due to bilateral damage to the primary auditory cortex in the temporal lobe. In this condition, auditory signal cannot be perceived by the auditory cortex, even though the peripheral hearing organs are functioning normally.[20] Cortical deafness is caused by lesions in the temporal lobe that affect Heschl’s gyrus, which houses the primary auditory cortex.[20] Additionally, lesions in other central auditory pathways, such as the inferior colliculi, medial geniculate nucleus or basal ganglia, can also lead to this condition.[21] Patients with cortical deafness typically present with a sudden bilateral loss of hearing. The diagnosis may be similar to other language and communication disorders, including Wernicke’s aphasia, auditory agnosia or verbal deafness.[20]
Temporal Lobe Volume Loss
Hearing impairment during the period of 45-65 years may be linked to neurodegeneration in the temporal lobe, which is a biomarker for the early stages of Alzheimer’s disease.[22] Hearing impairment in midlife is a significant risk factor for the loss of temporal lobe volume. Specifically, poorer hearing in the right ear during midlife is usually linked to a decline in the hippocampus and entorhinal cortex.[22] Primary age-related hearing loss is characterised as a clinical condition caused by damage to the peripheral auditory system, especially impacting the outer hair cells, stria vascularis or cochlear neurons.[23] Various risk factors contribute to age-related hearing loss, such as exposure to loud noises, cognitive function and genetic factors.[24] Recent study on age-related hearing loss has focused on studying changes in the central auditory and cerebral systems. One study found a link between hearing loss and reduced volume of grey matter in the temporal lobe.[25] Another study found that hearing loss is linked with reduced white matter volume.[26] Additionally, a longitudinal study reported a connection between hearing impairment and a decrease in grey matter volume in the right temporal lobe.[27] Peripheral hearing impairment can result in atrophy of temporal lobe due to neural deprivation from the absence of sensory input.[28] Reduced hearing is linked to decreased white matter volume in the left temporal lobe, which houses the auditory cortex and is crucial for high-frequency sound processing. Additionally, there is a reduction in white matter in the right insula, which has a significant role in auditory processing, as well as in right pre- and postcentral gyri, areas associated with speech.[29] This indicates that variations in volume are observed in certain brain areas associated with hearing impairment, rather than in other regions.
Stroke-Associated Lesion
Stroke-associated cortical deafness is a rare but severe type of hearing impairment.[30] It arises from the combination of cortical and subcortical damage along the central auditory pathway.[30] Bilateral injury to the primary auditory cortex and/or auditory radiation due to cerebrovascular ischemic events may result in a complete hearing loss called auditory deafness.[31] Neuroimaging is helpful to find out the ischemic changes in primary auditory cortex. The hypodense lesion of the auditory cortex is seen in computed tomography (CT) scan that suggests ischemic changes of auditory cortex. At the beginning of the stroke in the temporal lobe, the ischemia core is surrounded by oedema that appears similar in the CT scan. The auditory electrophysiological testing can be done that contributes to understand functional and neural alterations of cortical deafness due to stroke. Magnetic resonance imaging (MRI) and functional MRI are helpful to fully understand the nature of changes in auditory cortex following ischemic manifestations.
Nose-Induced Hearing Loss
The exposure to noise can lead to cochlear damage, which is linked to structural changes in the cochlear nuclei.[32] The deterioration of the peripheral auditory system significantly impacts the structure and function of the central auditory system.[32] Peripheral hearing impairment seems to affect the morphology of the auditory cortex, resulting in reduced grey and white matter volume within that region.[33]
Hearing Impairment and Cortical Deafness
Sensorineural hearing loss can happen at various stages, from the inner ear to the auditory cortex in the temporal lobe of the brain.[19] Afferent signals are sent from the cochlea to the auditory cortices on both the same side (ipsilateral) and the opposite side (contralateral) of the temporal lobe via brainstem nuclei and tracts.[19] Stroke is a primary cause of cortical deafness, which is the most severe form of central hearing impairment. Cortical deafness is usually poorly characterised and often misdiagnosed. An insult due to embolic stroke or intraparenchymal haemorrhage causing infarction at the auditory cortex leads to persistent symptomatic hearing loss. High-frequency hearing impairment is linked to a reduction in grey matter volume in the auditory cortex, along with an increase in cerebrospinal fluid (CSF) in that area, indicating potential atrophy of the auditory cortex due to hearing impairment. The relationship between hearing thresholds and the grey matter of the temporal lobe’s auditory cortex has been disrupted, suggesting that hearing impairment may causally affect the cortex.[33] Patients with cortical hearing loss typically exhibit normal otoacoustic emissions (OAEs), indicating that the outer hair cells are functioning properly. These individuals also show normal early latency response waveforms, suggesting that the cochlear nerve and brainstem are working as expected. Cortical deafness individuals manifest with central hearing impairment that is characterised by the inability to process auditory signals in the cortex, despite normal peripheral hearing.[34] Patients with cortical deafness maintain the ability to read, speak, write and respond to loud sounds.[35]
Conclusion
The temporal lobe is a vital part of the brain that plays an important role for getting the perception and understanding of hearing. It receives sensory input from peripheral auditory pathways and facilitates hearing to brain. Damage to the temporal lobe can lead to auditory perception. Understanding the lesions of the temporal lobe is crucial for formulating an effective treatment. The study of temporal lobe disorders is important for better understanding central auditory dysfunction. More focused studies are required to better understand the specific challenges and opportunities related to disorders of the temporal lobe.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Ethical approval was not applicable for this article, as this is a review article drafted from various research articles and not from patients directly.
Informed consent
The author has obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that her name and initials will not be published and due efforts will be made to conceal his/her identity, but anonymity cannot be guaranteed.
Credit author statement
Santosh Kumar Swain contributed to conceptualisation, literature search, data acquisition, manuscript preparation, manuscript editing and approval of the version to be published.
Data availability
Data are available in a public, open access repository.
Use of Artificial Intelligence
Nil.