
Abstract
Introduction:
Cavernous hemangioma of rectum is a slow-flow vascular malformation characterized by multiple dilated intramural blood vessels which shows T2 hyperintense signal, mainly on fat-suppressed sequences and may cause bleeding.
Case Details:
The report describes a case of a 16 Years boy who presented with recurrent episodes of rectal bleeding with hyperpigmentation in peri-anal region. MRI study suggested the diagnosis of rectal cavernous hemangioma.
Conclusion:
The illustrated case images highlight the role of clinical examination and MRI in diagnosis of rectal cavernous hemangioma. Peri-anal hyperpigmentation in a young patient with rectal bleeding should raise suspicion of rectal hemangioma.
Introduction
Rectal-perirectal haemangiomas are an important cause of episodic painless rectal bleeding. Peri-anal hyperpigmentation in a young patient with intermittent rectal bleeding should raise suspicion of rectal cavernous haemangioma. MRI plays an important role in the non-invasive diagnosis of this entity.
Case Details
A sixteen-year-old boy presented with a history of recurrent episodes of rectal bleeding. There were two to three episodes of fresh red-coloured stools in the last 12–18 months, which were not accompanied by abdominal pain or gastrointestinal symptoms. During his previous visits to other hospitals, he had undergone colonoscopy and imaging studies, but no specific diagnosis was mentioned in the available records. The blood parameters including the total leukocyte count and erythrocyte segmentation rates were within normal limits. The haemoglobin was 14 gms/dl.
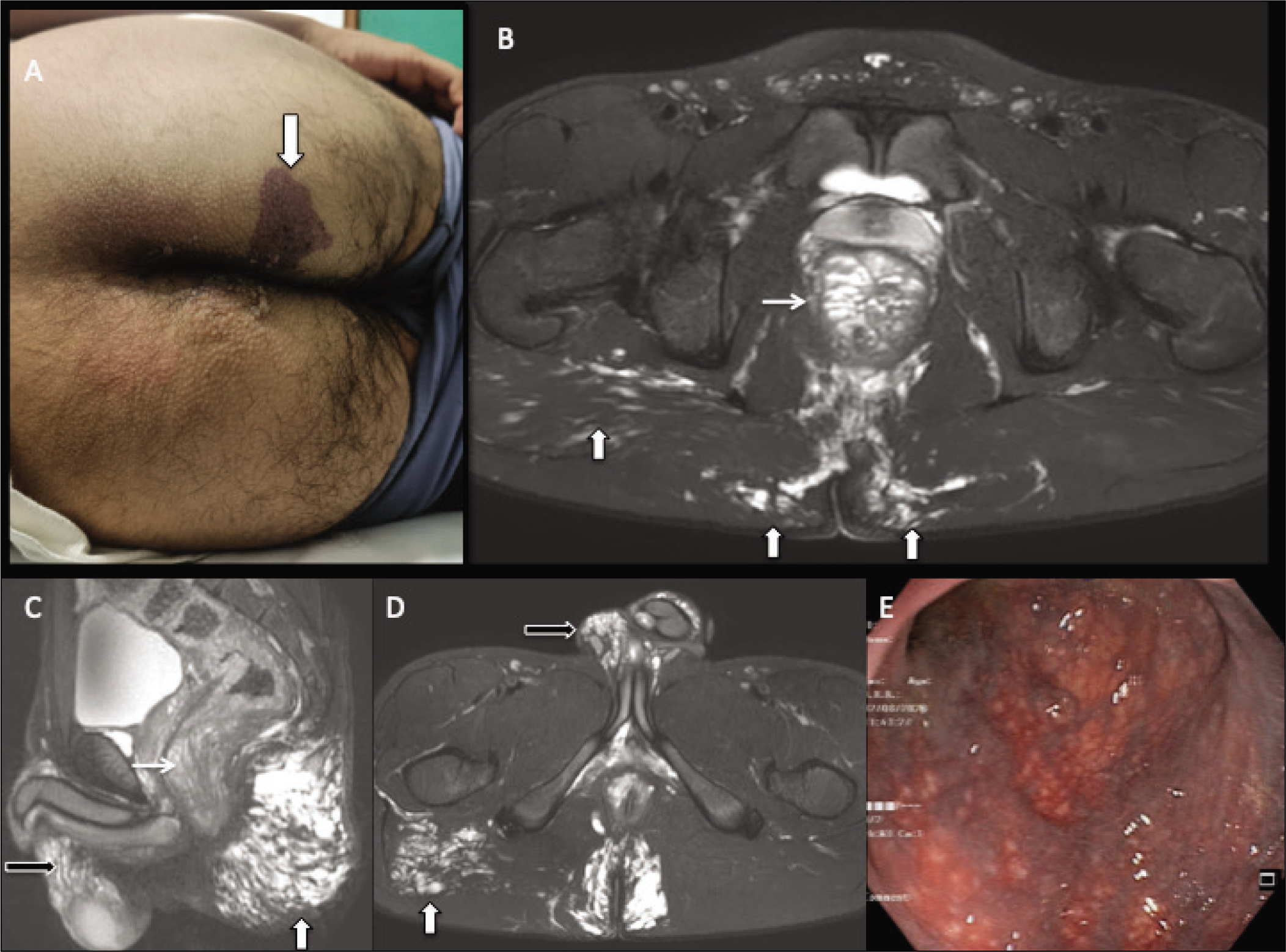
Clinical inspection revealed focal hyperpigmentation in peri-anal skin [downward arrow] with areas of ill-defined redness over the skin surface in peri-anal and bilateral gluteal regions [Figure 1, panel A]. A digital rectal examination did not reveal any palpable lesion or focal tenderness. The anal sphincter tone was within normal limits. MRI study shows long-segment mural thickening in the recto-sigmoid colon with T2 hyperintense signal intensity [arrow], without any obstructive changes [Figure 1, panels B & C]. There were multiple rounded and serpiginous T2 hyperintense foci, in the rectum few of which showed fluid-fluid levels. Similar foci were identified in the right scrotum [black arrow in panels C & D] and in gluteal regions [Figure 1, panel B, C & D]. Diffusion MRI showed a hyperintense signal without restricted diffusion [not shown]. Contrast MRI was not performed. MRI findings raised suspicion of rectal haemangioma with the involvement of the sigmoid colon. Lower GI colonoscopy showed extensive changes of mucosal surface lobulations with prominent compressible sub-mucosal vascular channels in the recto-sigmoid colon which were consistent with cavernous haemangioma. The patient refused any active surgical intervention and is presently under follow-up.
Clinical picture showing focal hyperpigmentation in peri-anal skin [downward arrow, panel A]. MRI study showing long-segment mural thickening in the recto-sigmoid colon with T2 hyperintense signal intensity [arrow], without any obstructive changes [panel B & C]. There were multiple rounded and serpiginous T2 hyperintense foci, in the rectum few of which showed fluid-fluid levels. Similar foci were identified in the right scrotum [black arrow in panel C & D] and in gluteal regions [ panel B, C & D]. Lower GI colonoscopy showing extensive changes of mucosal surface lobulations with prominent compressible sub-mucosal vascular channels in the recto-sigmoid colon which is consistent with cavernous hemangioma [panel E].
Discussion
Diffuse cavernous haemangioma of the rectum is a slow-flow vascular malformation characterised by multiple dilated blood vessels in the rectal wall.[1] MR imaging allows excellent soft tissue resolution and offers detailed delineation of the size and extent of the haemangioma in the rectal-perirectal region. Diffuse mural thickening with a hyperintense signal on T2WI, which is more evident on fat-suppressed sequences, is an important indicator of vascular cause.[2] Diffusion-weighted MRI and dynamic contrast-enhanced MRI may further support the diagnosis. The inferior mesenteric vein is often dilated and shows inferior extension up to the mesorectum. Mesenteric angiography can be a useful tool in patients with acute bleeding, which allows precise tumour localisation and guided endovascular ablation of the arterial component of the inflow. Although, not seen in our patient, Radiography and CT imaging may show the presence of phleboliths in the lesion, which is an important imaging sign of rectal haemangioma and is seen in 26%–50% of patients.[3] These are calcific foci due to intra-sinus thrombosis along with perivascular inflammation and blood flow stasis.
Despite the imaging signs, the diagnosis of rectal haemangioma is often delayed due to vague clinical presentations.[4] Because of the high risk of haemorrhage, a biopsy of clinically suspected haemangiomas is often not recommended for the diagnosis. Clinical examination findings of peri-anal hyperpigmentation offer vital clues to suspect an underlying vascular malformation as illustrated in our case.
Surgical resection is the optimal treatment of rectal haemangiomas. Conservative treatment options predominently include sclerotherapy[5] which may be performed using the direct injection of sclerosing agents like alcohol, sodium tetradecyl sulphate or polydocanol. MR imaging plays an important role in diagnosis, clinical decision-making regarding the appropriate treatment and surveillance of these patients.
Summary
The illustrated clinical photograph, MR imaging and colonoscopy findings in this case highlight the role of clinical examination and MR imaging in the diagnosis of diffuse rectal cavernous haemangioma in young boys with intermittent rectal bleeding. Peri-anal hyperpigmentation in a young patient with intermittent rectal bleeding should raise suspicion of rectal cavernous haemangioma.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical statement
Ethical approval was obtained for this article from the relevant institutional ethics committee, ensuring compliance with ethical standards for research involving human participants.
Human ethics
Human ethics approval was granted by the institutional ethics committee, confirming adherence to ethical guidelines for the inclusion of human participants in this study.
Patient consent
Patient consent was obtained from all participants included in this study, ensuring they were informed about the purpose, procedures, and potential risks involved in the research.
Credit author statement
NPG– Manuscript text and MRI Images/legends. Overall responsibility for the manuscript.
KK– Patient Clinical Details, Endoscopy Images/Legends.
Use of artificial intelligence
No AI tool is used for the writing of this manuscript.