
Abstract
Background and Aims:
India is one of the advancing ageing societies of the world; with this, the country’s demographic structure also changes. The incidence of lower limb fractures is high in this population, and it threatens their health both physically and mentally. Therefore, an effective anaesthesia and analgesia regimen is crucial for smooth and stable surgery and perioperative care.
Methods:
In this retrospective study, we aimed to describe the use of lumbar plexus block with an indwelling catheter as a sole anaesthetic technique intra-operatively and for providing peri-operative pain relief for 54 patients with intertrochanteric fracture posted for proximal femoral nailing or dynamic hip screw fixation from October 2020 to October 2023.
Results:
It was found that pain scores remained less than 1 for the majority of the study duration. Most patients underwent surgery within the first day of admission in our hospital and surgery lasted for one to two hours. All patients were discharged within five days of hospitalisation. There were no failures of the blocks before and during the surgical procedures. There were no records of any complications related to the technique. No supplement opioid was used during the procedure.
Conclusion:
With adequate monitoring, expertise, knowledge and familiarity with the procedure, lumbar plexus block with continuous infusion via a perineural catheter supplemented with periprocedural sedation can be used as a safe and effective anaesthetic technique for hip and proximal femur fracture reduction surgeries.
Keywords
Introduction
India is one of the advancing ageing societies in the world; with this, the country’s demographic structure also changes. According to the United Nations Population Fund, at the end of 2023, 68% of the total population of the nation are aged between 15 and 64 years, and 7% are aged 65 years and above. The incidence of lower limb fractures is high in this population, and it threatens their health both physically and mentally, including their ability to carry out daily activities. Elderly patients pose a challenge to the anaesthesiologist concerning advanced age and associated comorbidities.
Accordingly, such lower limb fractures are often treated surgically as early as possible as it restores early ambulation, thus preventing the dreaded risk of deep venous thrombosis, orthostatic pneumonia and bed sores in the elderly population. Early surgery also promotes healing and can improve limb function. Therefore, an effective anaesthesia and analgesia regimen is crucial for smooth and stable surgery and perioperative care.[1]
Lumbar plexus block (LPB) is a safe and effective option commonly used for postoperative pain relief in patients undergoing hip and proximal femoral surgeries and intraoperatively as an adjunct to general anaesthesia, which has been studied for many years.[2] In this case series, we aim to describe the use of a continuous LPB infusion as the sole anaesthetic as well as an analgesic option intraoperatively as well as for perioperative pain relief.
Anaesthesia and pain management for surgeries such as dynamic hip screw fixation and proximal femoral nailing can be challenging. The main anaesthetic modality for lower limb fracture is either general anaesthesia or central neuraxial anaesthesia in the form of subarachnoid block or epidural anaesthesia. In these elderly patients, general anaesthesia has disadvantages such as haemodynamic instability and unpredictable analgesia, while central neuraxial block could result in haemodynamic fluctuations, high level of motor block and anaesthesia of other limb.[3]
LPB, a targeted somatic nerve block, could be a safe and efficient alternative in cases where neuraxial blockade is contraindicated. It prevents sympathetic block even in cardiovascular-compromised patients, which might be a critical factor in reducing postoperative morbidity.[4]
Studies have shown the efficacy of LPB for hip fracture surgeries, but LPB with perineural catheter perioperative sedation as an effective alternative to general anaesthesia or neuraxial anaesthesia has not been studied widely and in this study, we aim to do the same.
Materials and Methods
In this retrospective observational study, after obtaining approval from the ethical committee, 54 patients who underwent hip or proximal femoral surgeries under LPB during the period of three years from October 2020 to October 2023 were analysed. Given the retrospective nature of data collection, a waiver of consent was given by the ethical committee. This study will have no direct impact on the patient’s rights, welfare or clinical care. All measures to minimise breach of confidentiality during record review and data collection were followed. Data analysis and reporting were done in a de-identified, aggregated form.
Aim and Objectives
The aim of this study was to describe the use of LPB as the sole analgesic and anaesthetic option for perioperative management of patients with hip and proximal femur fractures undergoing surgical management.
The primary objective is to describe the use of LPB with indwelling catheter as the sole anaesthesia technique for the surgery and for providing peri-operative pain relief for patients with intertrochanteric fracture posted for proximal femoral nailing or dynamic hip screw fixation.
The analgesic action will be measured by noting the pain score using the visual analogue score (VAS) prior to and after the block placement. Other parameters noted will be vitals before and after placement of block, duration of the procedure and use of rescue analgesics.
On arrival, all patients were given injection midazolam 0.15 mg/kg, a maximum of 2 mg, and injection fentanyl (2 μg/kg). Oxygen was supplemented via Hudson’s facemask at 6 L/m. The patient was positioned to lateral decubitus with the affected side up. Parts were prepared with aseptic solution and sterile drapes placed. LPB was secured using peripheral nerve stimulator following Winnie’s posterior approach[5] [Figure 1]. Once the lumbar plexus was reached, a bolus of 30 mL of 0.25% bupivacaine was given, followed by the placement of a nerve block catheter, which was then tunnelled and secured. An infusion of 0.18% ropivacaine was started at 8–10 mL per hour and continued until surgery.
Placement of LPB catheter

During surgery, all patients were sedated using an infusion of propofol at a dose of 25–50 μg.kg-1 min-1. For surgical anaesthesia, a bolus of 30 mL 0.25% bupivacaine was given on arrival to the operating room. Along with standard monitors, respiratory rate was monitored using a side-stream sensor of end-tidal carbon dioxide (EtCo2), and oxygen was supplemented using a Hudson’s facemask. Fluid infusion and blood–blood products were transfused as required. The surgical duration was noted.
Postoperatively, an infusion of 0.18% ropivacaine was administered through the nerve block catheter at 10 mL per hour, and a bolus of 10 mL was given in case of breakthrough pain. Pain score and vitals were measured, and the need for rescue analgesics, time to mobilisation and duration of hospital stay were noted.
Data will be collected only from those patients who had the procedure done under block alone. Those patients on whom general or spinal anaesthesia was electively added along with the block will not be included in this report.
Statistical Analysis
Summary statistics were presented with mean ± SD and frequency (%) for the continuous and categorical factors respectively. The median (IQR) was presented while the data skewed. Normality of the data was checked by using Shapiro–Wilk test. Paired sample test/Wilcoxon signed rank test was used to determine the significant changes between paired observations. Friedman test was used to determine the changes in the VAS over the time period for the both post-block and postoperative examinations. P value < .05 was considered as statistical significance. All the statistical analysis was computed by using SPSS (IBM, 28.0).
Results
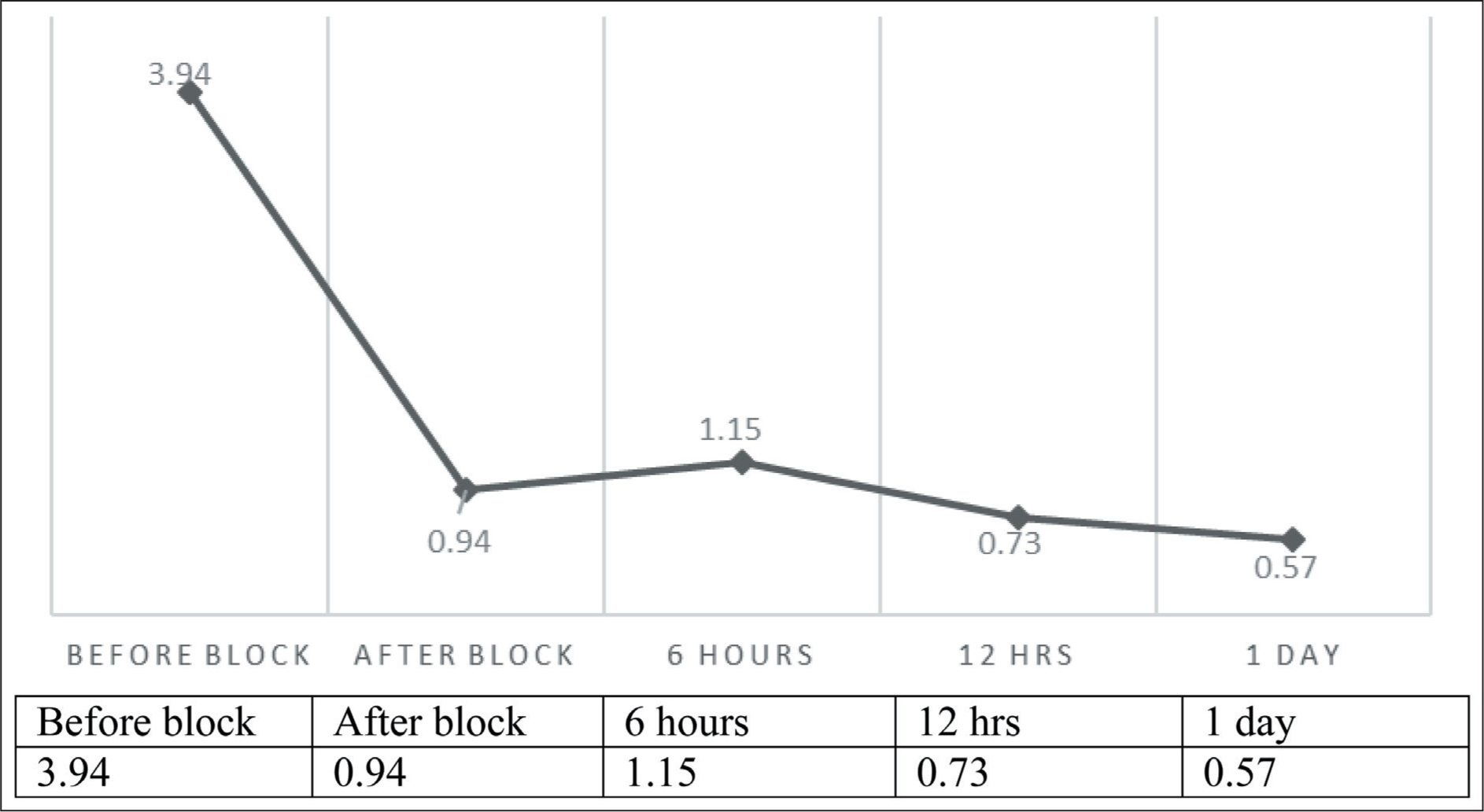
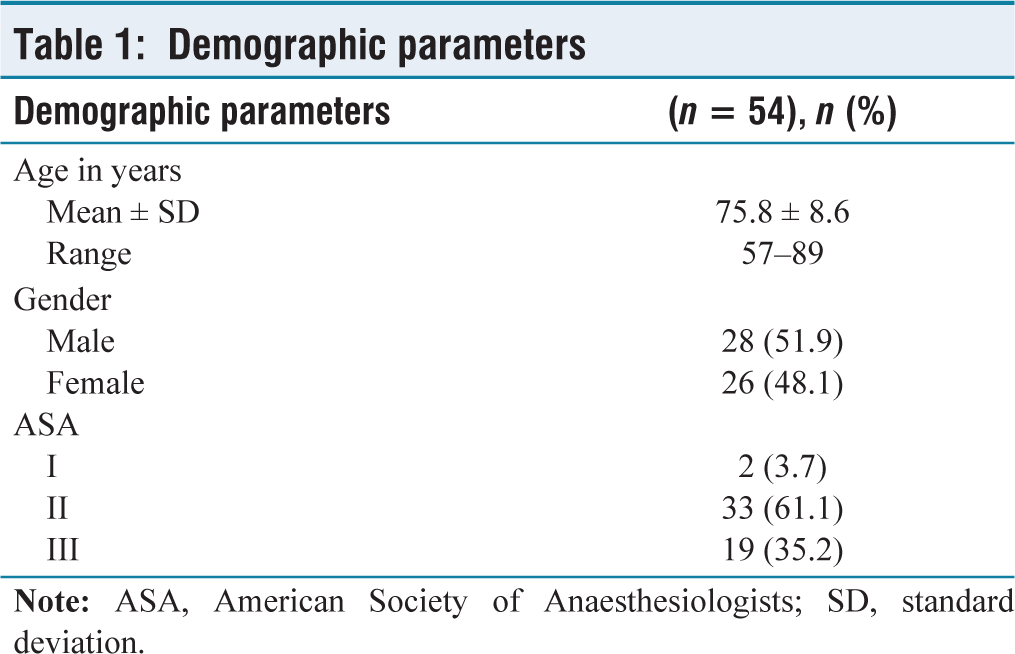
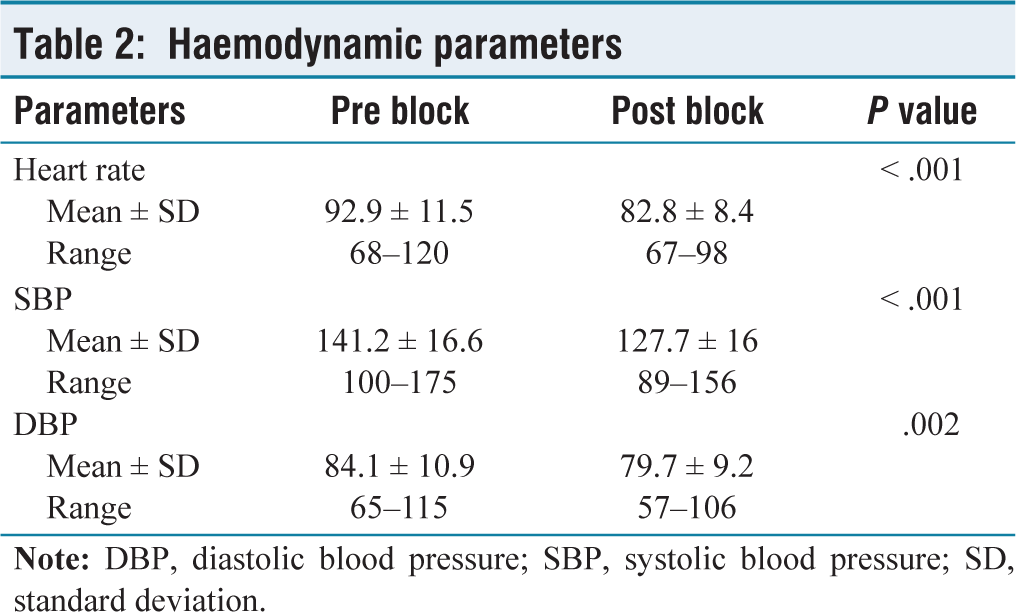
The patients included in this study belonged to the age group of 57 to 89 years, with an average of around 76 years. There was no significant difference between both genders, and the majority of the patients were either ASA class 2 or 3 [Table 1]. Figure 2 shows the mean pain score, and a significant decrease in pain score is seen immediately after the placement of the block. Pain scores remain less than 1 for majority of the study duration. Haemodynamic parameters show significant change after block placement as shown in Table 2. Most patients underwent surgery within the first day of admission in our hospital, and surgery lasted for one to two hours. All patients were discharged within five days of hospitalisation. There were no failures of the blocks before and during the surgical procedures. There were no records of any complications related to the technique. No supplement opioid was used during the procedure.
Perioperative pain score trend
Demographic parameters
Haemodynamic parameters
Discussion
As the incidence of lower extremity fractures is increasing and surgery remains the mainstay treatment, having an optimal anaesthesia protocol for such surgeries that can cater to an elderly population is important.
In this study, we aimed to demonstrate the efficacy of continuous LPB with perioperative sedation as an effective alternative to general or regional anaesthesia for hip fracture surgeries. It was observed that this technique provided profound analgesia, adequate muscle relaxation and excellent postoperative pain control. Multiple studies showed the benefits of using single-shot posterior LPB as an anaesthetic technique for hip fractures, but continuous infusion via a perineural catheter was not studied widely.[6]
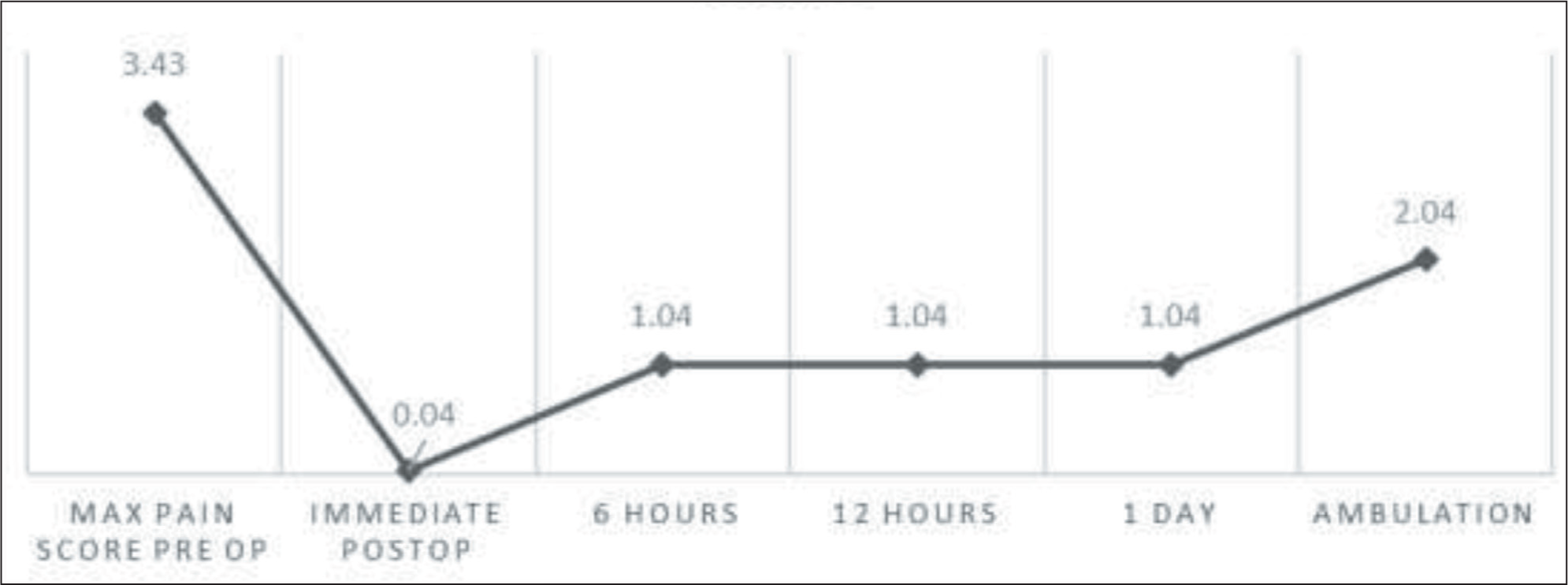
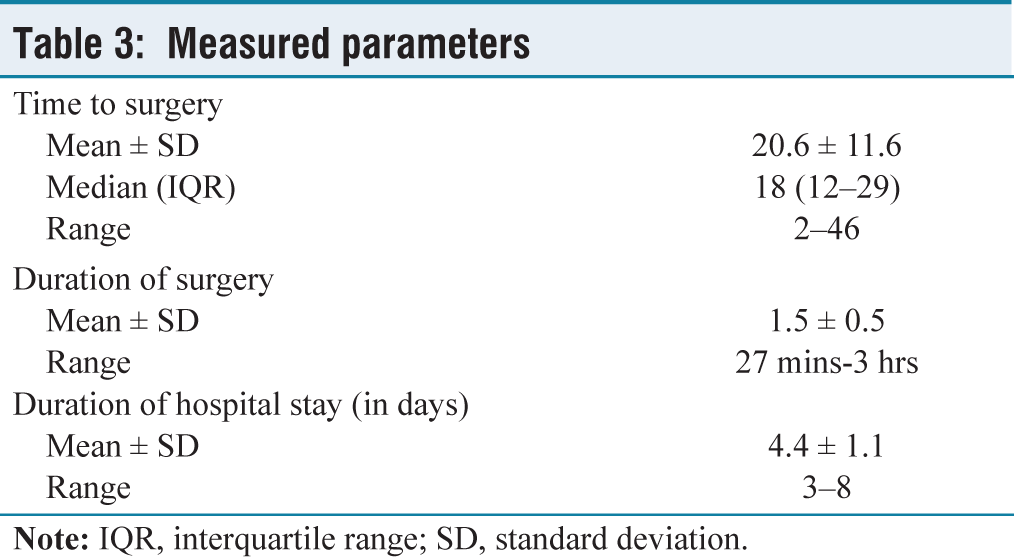
We observed that the pain scores were majorly below or near 1 for a considerable amount of time; this was demonstrated in the perioperative pain score trend in Figure 3. The maximum pain score prior to block placement was more than 3, which drastically reduced after LPB and continued to be the same throughout. The block also provided stable haemodynamic conditions throughout the surgery, as demonstrated by other studies.[7] The mean time to surgery, duration of surgery and duration of hospital stay were also noted in Table 3. Though not compared with existing studies nor officially analysed, the block was found to have aided in early ambulation and early discharge. There were no adverse events noted in this study, rendering this as a safe option in the elderly group, similar to the study done by Xu et al.[8] Surgeon satisfaction as observed in an unofficial manner in terms of muscle relaxation, surgical conditions and blood loss was acceptable, and this alternative anaesthesia option seemed appropriate. This was similar to the observations made by Amiri et al.[9]
Maximum perioperative pain score trend
Measured parameters
Although many studies have focused on the different modes of anaesthesia for lower limb surgeries, there is a paucity of similar data in our country, especially for continuous catheter-based infusion blocks. This could be because of the lack of expertise, the need for monitoring or the poor availability of study-based evidence.
Conclusion
With adequate monitoring, expertise, knowledge and familiarity with the procedure, LPB with continuous infusion via a perineural catheter supplemented with periprocedural sedation can be used as a safe and effective anaesthetic technique for hip and proximal femur fracture reduction surgeries. LPB provides stable perioperative haemodynamics, adequate analgesia, satisfactory anaesthetic and surgical conditions and patient and surgeon satisfaction, all leading to early ambulation, fewer postoperative complications and reduced duration of hospital stay.
Footnotes
Acknowledgements
Thanks to Shivashankari—research assistant and Logesh—biostatistician, Research Department, Apollo Hospital, Chennai, Tamil Nadu, India.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional Ethical Committee Approval Number
Ethical approval was obtained from Institutional Ethics Committee- Bio Medical Research, Apollo Hospitals, Chennai. Application no- AMH-C-S-011/02-24.
Informed consent
Informed consent has been obtained from all the patients who met the eligibility criteria.
Credit author statement
SV participated in data acquisition, literature search, investigations, data analysis and manuscript preparation.
VR participated in conceptualisation, investigation, supervision, data analysis and manuscript editing.
Both the authors reviewed and approved the manuscript.
Data availability
Data presenting the study’s findings is available with the corresponding author.
Use of Artificial Intelligence
Nil.