
Abstract
Introduction:
Whipple’s (pancreatoduodenectomy) surgery carries significant post-operative morbidity even in specialised centres. We share our findings by comparing the inflammatory markers C-reactive protein (CRP) and white blood cell count (WBC) in early detection of post-operative complications.
Material and Methods:
In this prospective study, 56 patients who underwent the Whipple procedure in our institution between January 2021 and December 2022 were evaluated. Demographic characteristics, pre-and post-operative CRP and WBC levels, intraoperative parameters like pancreatic texture and duct diameter, intraoperative blood loss, postoperative complications, length of stay and final histopathology were evaluated. The receiver operator characteristics curve (ROC) was drawn, and the area under the curve was calculated.
Results:
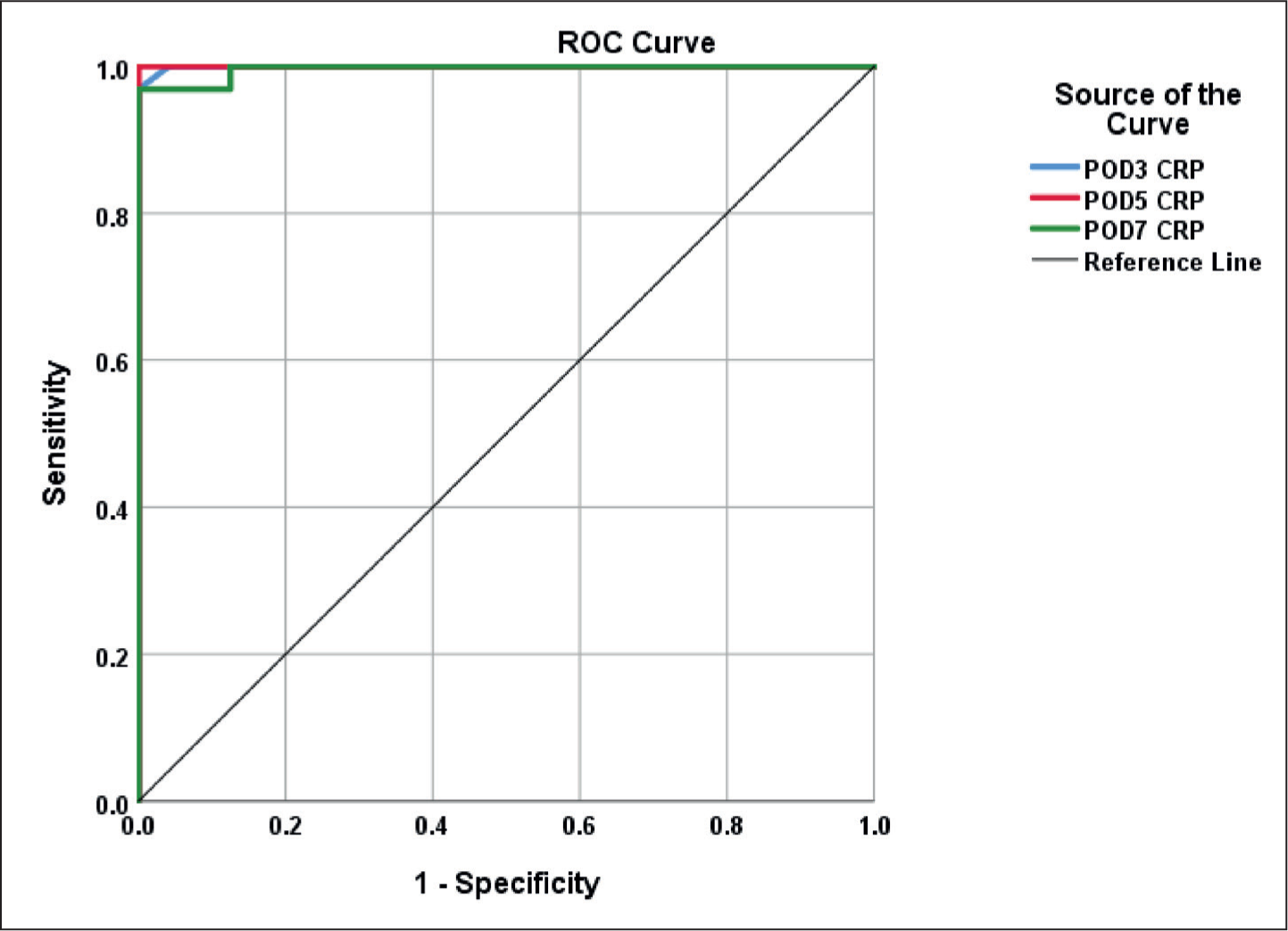
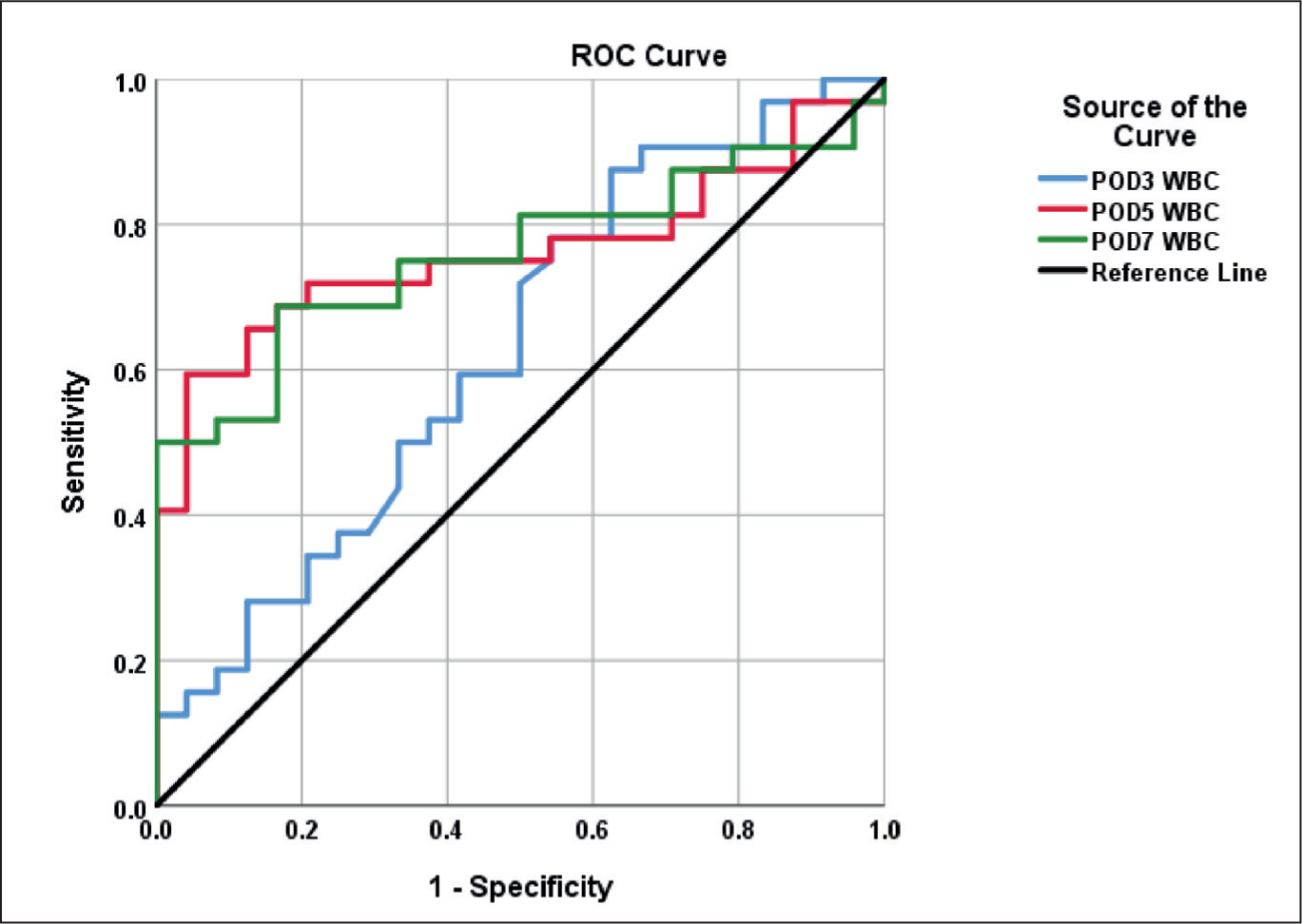
Among the 32 (57.2%) patients who developed complications, 6 (10.7%) had major and 26 (46.4%) had minor complications. ROC curves revealed greatest area under curve value for POD5 CRP (AUC-1.000; P <.01) followed by POD3 (AUC-0.999; P < .01) and then POD7 (AUC-0.995; P < .01). For WBC, the greatest value was found only on POD5 (AUC-0.742; P = .003) followed by POD7 (AUC-0.716; P < .009), but not on POD3 (AUC-0.607; P = .19).
Conclusion:
C-reactive protein was better than white blood cell counts in the early detection of postoperative complications.
Introduction
Whipple’s surgery is a complex procedure whose morbidity (40%-50%) remains high even with advancements in technology, improvisation of technical skills of operating surgeons, improved imaging modalities and standardisation.[1-3] Postoperative pancreatic fistula (POPF) is the most common complication encountered, with an incidence of up to 35%, which can lead to post-pancreatectomy haemorrhage and abdominal sepsis.[3] Delays in recognising and managing these complications will prolong the ICU and hospitalisation stay, which substantially increases the use of additional resources for each patient, thereby raising the expenditure even further.[3] The natural post-surgical systemic inflammatory response syndrome (SIRS) can be difficult to discern from early complications. Here is where the part of White blood cell count (WBC) and C-reactive protein (CRP), two inflammatory biomarkers that predominantly reflect a patient’s inflammatory status, may be effective for early diagnosis of problems.[4,5] C-reactive protein has been shown to predict anastomotic complications in colorectal surgery and infectious complications occurring after major surgical procedures in the abdomen.[6,7] But in Whipple’s surgery, different studies showed mixed results, with some favouring and others denying it as a predictor of complications.
CRP is a quick, affordable, and generally accessible biological marker. With its short plasma half-life, CRP levels tend to return to baseline quickly in individuals with a simple postoperative course.[8] However, in patients with complicated postoperative periods, they will remain elevated, thereby alerting the physician to remain vigilant and expect complications. CRP is most widely used in European countries, whereas others were still dependent on WBC as an inflammatory marker.
Previous studies evaluated the role of inflammatory markers in early recognition of post-operative pancreatic fistula only. Only a few studies evaluated the role of C-reactive protein in detecting major complications. In this study, we are comparing CRP and WBC in the early postoperative phase to identify major complications following pancreatoduodenectomy.
Materials and Methods
Study Population
In this prospective study, all the patients who underwent Whipple surgery in our institution between January 2021 and December 2022 were included, with the exclusion of patients who had concurrent additional organ resections or vascular reconstructions and preoperative infections with deranged baseline CRP and WBC levels.
Data Collection
The demographic profile, clinical history, and preoperative investigation (both laboratory and imaging) were collected along with a baseline value of both CRP and WBC, pancreatic duct diameter in millimetres as per the preoperative CECT abdomen (which is uniform and objective), and ASA status.
During surgery, intraoperative details such as the pathology for which being operated, pancreas texture, blood loss in millilitres, type of pancreatic anastomosis and stent placement. Postoperative complications were noted and graded according to Clavien Dindo’s classification, with grades I-II as minor and III-V as major complications, along with CRP, WBC values on POD 3,5,7 and drain amylase values until removal and length of stay in hospital. Patients were followed up for 30 days for any events of readmission and re-operation. Major complications (post-operative pancreatic fistula, post-pancreatectomy haemorrhage and delayed gastric emptying) were defined as per the International Study Group for Pancreatic Surgery criteria. Also, bile leak and intra-abdominal infection and collections were recorded. The length of hospital stay will be defined as the period from the day of the operation to the end of hospitalisation. Our lab reference value for normal CRP is <5mg/L, and for WBC, it is 4000-11,000 cells/mm3.
Statistical Analysis
Data were analysed in SPSS v25. Descriptive statistics were represented with percentages for qualitative data and mean with SD for quantitative data. Shapiro Wilk test was applied to find normality. The chi-square test and Fisher Exact test were applied for the comparison of proportions. ANOVA, Post hoc test – Tuckey test was applied to find significance. ROC curve was drawn. The area under the curve was calculated. Sensitivity, specificity, positive predictive value and negative predictive value were calculated. P < .05 was considered statistically significant.
Results
A total of 56 patients were eligible for the study among the 72 Whipple surgeries during the study period. Among them, six developed major complications and 26 developed minor complications. The demographics and peri-operative characteristics of the study population are displayed in Table 1. Intraoperative blood loss of more than 500 mL was significantly associated with the development of complications. The length of hospital stay was more in the patients who developed complications.
Clinical and peri-operative characteristics
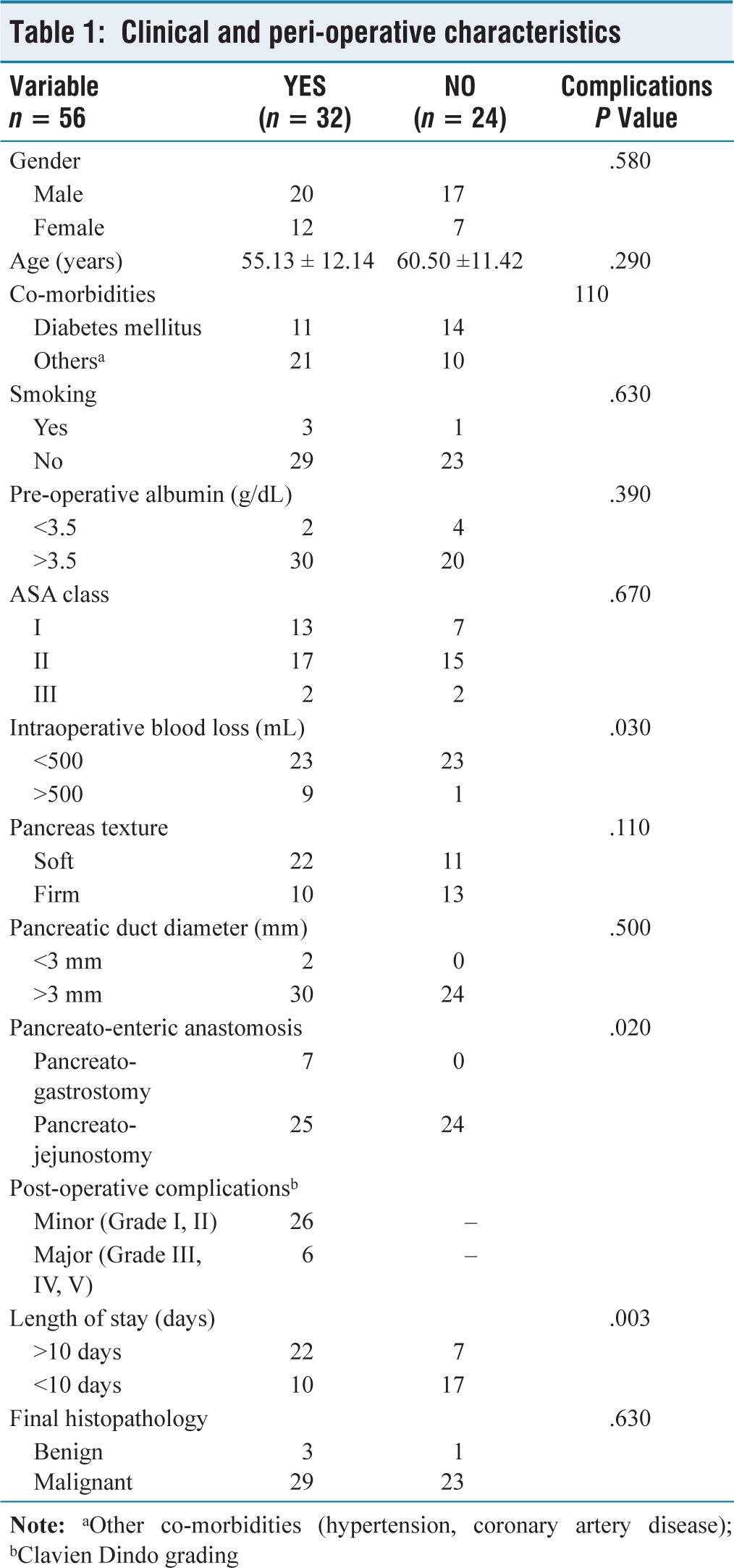
Among the major complications, three had post-operative pancreatic fistula – B requiring percutaneous image-guided drainage of the collection; one had post-pancreatectomy haemorrhage – C, which required relaparotomy for control following failed endoscopic therapy; one had delayed gastric emptying – B with pancreatic fistula related collection, which was managed with pigtail drainage and one had deep surgical site infection presenting with fever due to infected collection managed with antibiotics and pigtail drainage. All of them recovered well following the intervention. There is a significantly high mean CRP value in these patients on POD3 (202.6 ± 14.4 mg/L), POD5 (239.6 ± 33.9 mg/L) and POD7 (242.9 ± 34 mg/L), respectively, with a P value of < .001 in raising trend suggestive of the development of significant complications [Tables 2–3, Figure 1].
Accuracy of inflammatory markers in detecting post-operative major complications

Sensitivity, specificity, positive predictive and negative predictive value for CRP on POD3,5,7 respectively

Receiver operating characteristic curve for CRP on POD3,5,7 respectively
The mean value of WBC measured on POD3 (13,006.7 ± 915.5 cells/mm3; P −.11) was not significant in detecting major complications, but was significant for values on POD5 (14,120 ± 4,051.1 cells/mm3; P < .001) and POD7 (15,045 ± 5,234.7 cells/mm3; P < .001) [Table 4, Figure 2].
Sensitivity, specificity, positive predictive and negative predictive value for WBC on POD3,5,7, respectively

Receiver operating characteristic curve for WBC on POD3,5,7, respectively
Discussion
The mean C-reactive protein values in the patients who developed major complications in this study were significantly raised on POD3,5 and 7 with P value of < .001. Likewise, the mean white blood cell counts on POD5 and POD7 were significantly associated with major complications, except for POD3, which is similar to the study by Dongen et al.[9] Since the number of patients who developed major complications in this study were less (n = 6; 10.7%), deducting cut-off value is not possible. This smaller number of major complications can be due to a multitude of reasons such as normal BMI, ASA2 with adequately controlled co-morbidities, fewer number of smokers, following enhanced recovery after surgery protocol (ERAS) and also none underwent pre-operative biliary drainage for obstructive jaundice, which is an exclusion criterion, unlike most other studies. Although the cut-off value was not ascertained, the minimum CRP value was found to be more than 180 mg/dL on all measured days (POD3,5,7) in patients with major complications. Also, in patients without complications, none of the CRP values measured were above 112 mg/dL.
Welsh et al showed that for POD4 cut-off value of >140 mg/L is significantly associated with post-operative inflammatory complications. The mean CRP on POD3 peaked at 173 mg/L in patients with complications, which persisted thereafter, which is similar to our study in which the mean CRP value on POD3 (202.6 ± 14.4 mg/L) in patients with complications. Also, in the same study for patients without complications, the CRP value peaked on POD3, followed by a decline thereafter, which is similar to our study.[10] Hiyoshi et al. predicted that pancreatic fistula occurred in patients with POD3 CRP cut-off value >200 mg/L with significant elevations from POD2 to POD5, which is similar to our study.[11] Jamieson et al. also demonstrated that POD2 CRP of 180 mg/L or higher (P < .05) was significantly associated with pancreas-specific complications with prolonged ICU stay, similar to our study.[12] Dongen et al. showed that CRP values on POD3 and POD5 were superior in detecting major complications, unlike on the POD7 level. Also, CRP was significantly better than WBC levels on POD3 and POD5. This is almost similar to our study, where all the CRP values measured on POD3,5,7 were significantly elevated, whereas the POD3 WBC was not significantly raised, unlike on POD5 and POD7.[9]
In our study, blood loss >500 mL and the type of pancreatic anastomosis were significantly associated with complications, unlike Dongen et al., whose study showed that body mass index, pancreatic duct diameter and the texture of the pancreas were associated with complications.[9] Also, Jamieson et al., in their study, reported that a soft pancreas and small duct diameter of the pancreas were significantly associated with complications.[12]
There are limitations in our study such as a moderate sample size, a smaller number of patients developing major complications and a limited duration of post-operative follow-up.
Conclusion
In our study, CRP was found to be a more sensitive and specific inflammatory marker than WBC in patients who developed complications post-Whipple surgery. Also, a gradual rising trend in CRP levels was observed as early as POD3 onwards in patients who developed complications, unlike WBC levels, which started increasing from POD5 only. Serial monitoring of CRP levels can be utilised to forecast early postoperative complications and treat them at their earliest stages, thereby decreasing associated morbidity. Also, patients with persistently low CRP levels can be planned for early discharge, thereby avoiding prolonged hospitalisation. Large-scale, multicentre trials are required to validate the study findings.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Institutional ethics committee approval has been obtained (Application number AMH-DNB-072/07-21).
Informed consent
Informed consent has been obtained from all patients who met the eligibility criteria.
Credit author statement
All authors contributed to the study conception and design. Literature search and data acquisition were done by Jayapal L., while the manuscript, data processing and final editing were done by all three authors. All authors read and approved the final manuscript.
Data availability
Data supporting the findings of this study is available with the corresponding author.
Use of artificial intelligence
Nil.