
Abstract
Objective:
To explore the complex relationship between metabolic syndrome (MetS) and musculoskeletal (MSK) disorders, highlighting the impact of MetS on bone and joint health, and to propose effective management strategies for improving patient outcomes.
Methods:
This comprehensive review involved an extensive literature search conducted on 17 September 2024, utilising scientific databases such as PubMed, Google Scholar, and Scopus. The search, focused on articles published in English and pertaining to humans, employed Boolean operators and MeSH terms ‘MSK’, ‘metabolic diseases’, ‘diabetes’ and ‘osteoporosis’.
Results:
MetS, characterised by obesity, inflammation, insulin resistance (IR), and hypertension, is closely associated with a variety of MSK disorders including osteoarthritis, osteoporosis, and tendinopathy, among others. These conditions exacerbate MetS symptoms, creating a feedback loop that complicates patient management. The review identifies both common and rare metabolic and genetic disorders contributing to MSK issues, emphasising the intricate interplay between metabolic dysfunctions and MSK health. Special attention is given to the MSK manifestations of prevalent metabolic diseases such as diabetes mellitus, gout, and osteoporosis, underscoring their significant impact on quality of life.
Conclusion:
Understanding the relationship between MetS and MSK disorders is crucial for the development of holistic management strategies. The review suggests that addressing the root metabolic issues alongside direct treatment of MSK symptoms can significantly improve patient outcomes. Future research should focus on integrated care approaches that offer hope and optimism for individuals facing these interconnected challenges.
Keywords
Introduction
Metabolic syndrome (MetS) is a cluster of conditions linked to type 2 diabetes (T2D) and cardiovascular disease, which are associated with various musculoskeletal (MSK) issues. Obesity, inflammation, insulin resistance (IR), and hypertension are essential components of MetS, contributing to the development of osteoarthritis (OA), osteoporosis, low back pain, muscle weakness, tendinopathy, fibromyalgia, gout, bone mineral density (BMD) loss, adipose tissue dysfunction, and myofascial pain.[1] These MSK conditions can further exacerbate the symptoms of MetS, creating a vicious cycle. The prevalence of MSK diseases associated with MetS varies based on age, gender, ethnicity, and location. Literature suggests that disability rates in individuals with metabolic diseases are 10%–15% higher than those without it.[2]
In addition to the previously mentioned conditions, MetS has been linked to an increased risk of plantar fasciitis, lateral epicondylitis, and adhesive capsulitis.[3] These conditions are often associated with obesity, IR, dyslipidaemia, and hypertension, which are essential components of MetS. Chronic inflammation, IR, and obesity are key factors contributing to these MSK issues.[4]
Beyond the more common MSK conditions associated with MetS, there are also rare genetic and endocrine disorders that can increase the risk or severity of these issues. Conditions like Achondroplasia-like disorders, Lipodystrophy, McCune-Albright Syndrome, Majeed Syndrome, Cherubism, Fibrodysplasia Ossificans Progressiva, Marfan Syndrome, Ehlers-Danlos Syndrome, Primary Hyperparathyroidism, Hypophosphatasia can all contribute to abnormal bone growth, fat distribution, or metabolic imbalances, leading to MSK problems and exacerbating the symptoms of MetS.[5]
Metabolic diseases are characterised by abnormalities in production, storage, or energy use, which may manifest in the MSK as pathologies. These conditions can lead to various symptoms, including pain, stiffness, and weakness.
While numerous metabolic disorders involve the MSK, this review focuses on the most frequent disorders and overlapping conditions. The objective is to highlight the relationship between MetS and MSK and explore effective management strategies. By understanding the complex interplay between MetS and MSK, we can develop and implement effective management strategies that can significantly improve patient outcomes, offering hope and optimism in the face of these challenging conditions.
Methods
An extended literature review was performed on the 17th of September 2024 on freely accessible available scientific databases (PubMed, Google Scholar, and Scopus). The Boolean operators used were [AND] and [OR]. The MeSH terms used for the search were ‘MSK’, ‘metabolic diseases’, ‘diabetes’, and ‘osteoporosis’. Only fully available free-text articles were considered. The search was refined to include only English articles and studies conducted on humans.
Results and Discussion
Metabolic Diseases and their MSK Manifestations
Various MetS exert a profound impact on bone and joint health, leading to a spectrum of MSK problems [Figure 1].
Metabolic Diseases and their Common Associated Musculoskeletal (MSK) Manifestations
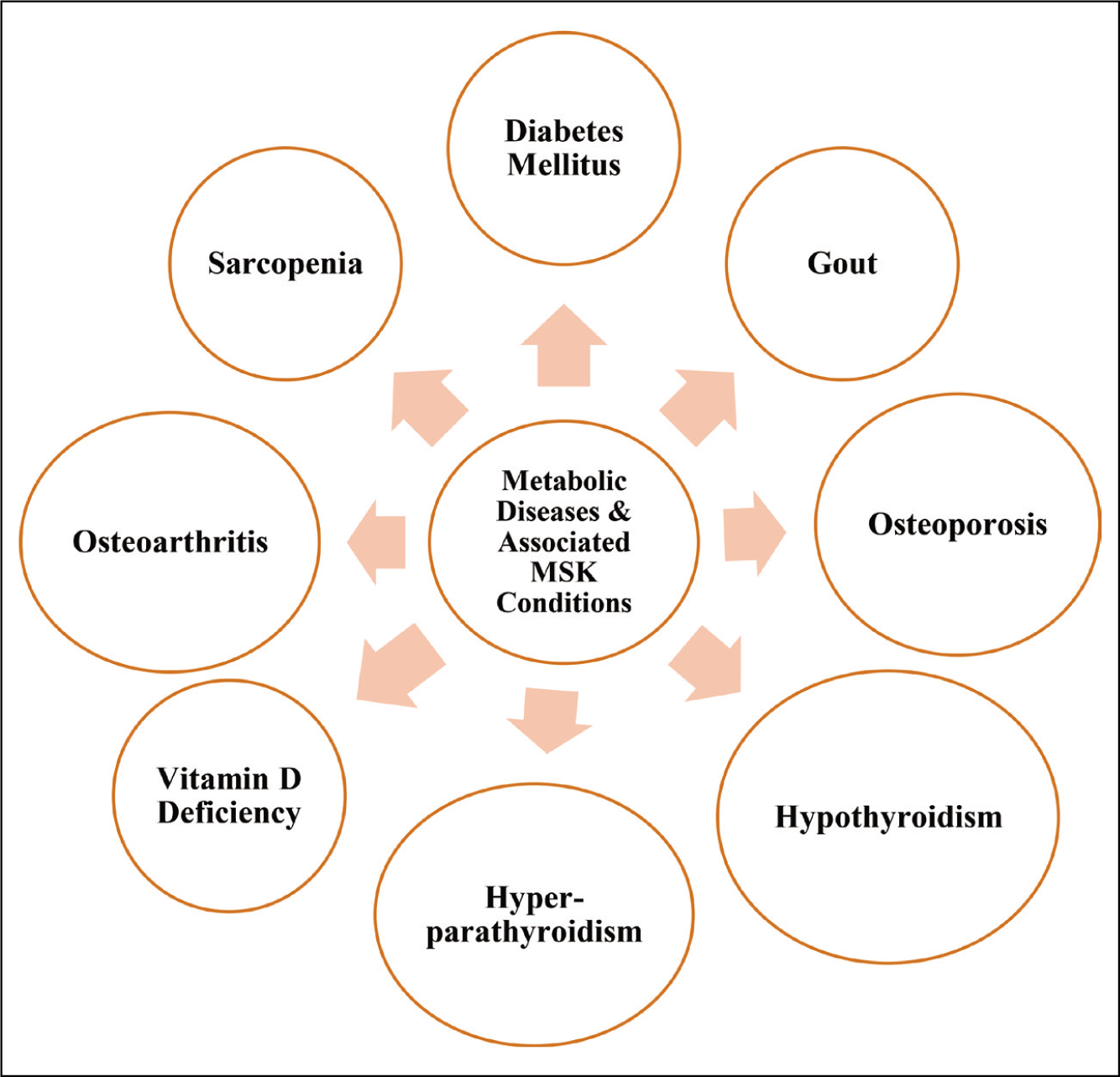
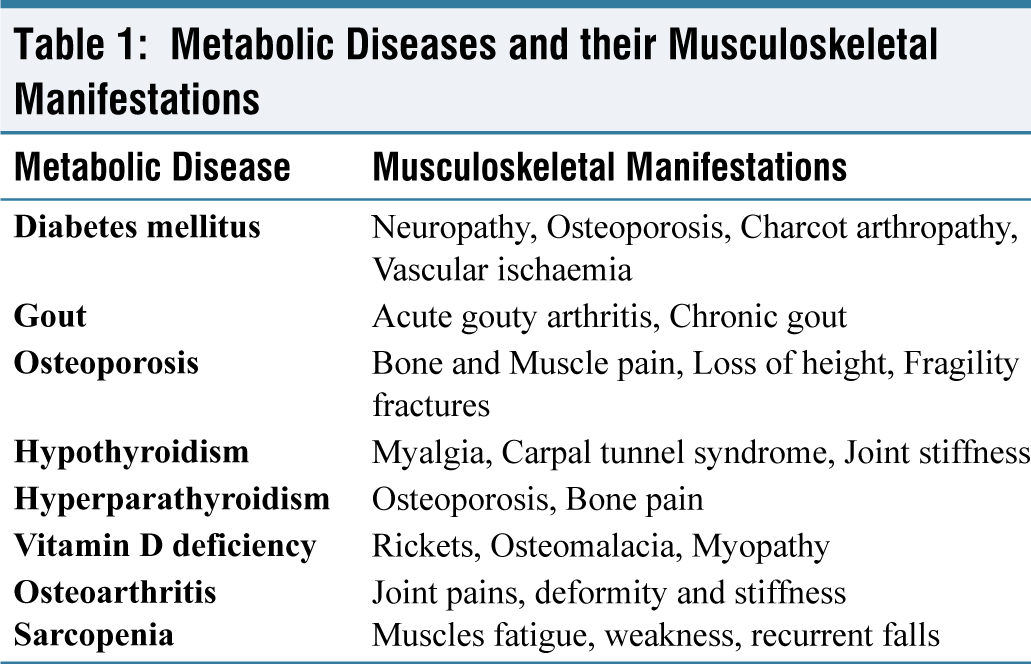
These conditions disrupt normal metabolism and often lead to abnormalities in the structure and function of bones and joints. A brief description of some common MetS that are closely associated with MSK disorders is presented in Table 1.
Metabolic Diseases and their Musculoskeletal Manifestations
Diabetes Mellitus
Diabetes mellitus (DM) is the most common metabolic disorder encountered in the Asian subcontinent. The majority type encountered is T2D-90%, followed by type 1 diabetes (T1D)-10%. Both types affect bone health, as poor glucose control and IR can affect bone metabolism and the MSK system.[6]
Diabetic neuropathy is usually a peripheral type but seldom can also be present in the form of autonomic and proximal neuropathy.[7] The symptoms may include pain, numbness, loss of balance and weakness in the extremities due to neuropathy. DM can also increase the likelihood of osteoporosis, leading to an increased risk of fragility fractures and Charcot’s neuroarthropathy, which is characterised by haphazard joint destruction and without pain.[8] It is most commonly seen in the feet of individuals with diabetes. This is often managed by offloading the affected joint and bracing it.[9] Surgical intervention is required in only severe and deformed cases. Diabetes is also associated with an increased risk of OA, and vascular ischaemic problems, leading to ‘diabetic foot’, non-healing wounds, and gangrene.
Gout
Gout is a form of inflammatory arthritis arising from the metabolism of purines, substances found in many foods and human cells. The prevalence of gout ranges from 1% to 10% globally, with more predilection towards some ethnicities.[10] When the body breaks down purines, it produces uric acid. Hyperuricemia is commonly seen in clinical practice, and the sudden fluctuation in serum uric acid level may precipitate an attack of gout. Excessive production or inadequate excretion of uric acid leads to its accumulation, forming sharp, needle-like urate crystals in a joint or surrounding tissue, causing pain, inflammation, and swelling.[11] The gout may present as:
Acute gouty arthritis is characterised by sudden, severe pain, redness, and swelling in a joint, often the big toe. Recurrent attacks, joint damage and deformity might complicate it. Kidney stones due to uric acid crystals (urate) deposition are also not uncommon. Management involves nonsteroidal anti-inflammatory drugs (NSAIDs), colchicine, and corticosteroids.[12] Chronic Gout may present due to recurrent acute gout attacks, joint damage, and uric acid deposits (tophi). Management involves lifestyle modifications (avoiding triggers like alcohol, red meat, and certain medications) and medications to lower uric acid levels (Allopurinol, Febuxostat).[13]
Osteoporosis
Osteoporosis is a silent disease with mild telltale signs such as bone pains, decreased height and fragility fractures after trivial falls.[14] This condition, characterised by weakened bones more prone to fracture, is linked to metabolic disturbances in calcium and vitamin D metabolism. Osteoporosis results from an imbalance between bone resorption and bone formation, decreasing bone mass and density. Factors like hormonal changes, especially in postmenopausal women, and inadequate dietary intake of calcium and vitamin D can exacerbate this condition.[15] The risk factors include poor blood sugar control, IR, and certain medications like corticosteroids, and thyroid hormones. The management includes quantification by DEXA scans and treatment in the form of physical activities to load the joints and medical treatment in the form of calcium, vitamin D3 supplementation and anti-osteoporotic therapy (e.g., bisphosphonates, denosumab, etc.) based on the severity of osteoporosis.[16]
Hypothyroidism
Metabolic diseases related to the thyroid are often encountered, with hypothyroidism being four times more prevalent than hyperthyroidism.[17] The most frequently encountered clinical presentations associated with hypothyroidism are myalgia, carpal tunnel syndrome, hair loss and joint stiffness, especially in the morning. Treatment relies on thyroid replacement therapy. Carpal tunnel syndrome is a multifactorial disease and is only associated seldom with hypothyroidism. Management includes splinting, physical therapy, and, in severe cases, surgery.[18]
Hyperparathyroidism
This condition involves the parathyroid hormone (PTH) overproduction by the parathyroid glands, which is often triggered by a benign tumour or secondary stimulation due to chronic vitamin D deficiency (VDD). PTH is responsible for regulating calcium levels in the blood.[19] Overproduction leads to excessive calcium extraction from the bone, weakening it and increasing the risk of osteoporosis and fractures. It can also lead to the formation of calcium stones in the kidneys and calcium deposits in other tissues.
Vitamin D deficiency
Osteomalacia and Rickets are related to VDD, leading to softening of the bones due to impaired bone metabolism. In children, the condition is called Rickets and can cause bone deformities.[20] In adults, it is known as Osteomalacia, resulting in weak bones, bone pain, and muscle weakness. Pseudo fractures or insufficiency fractures can happen in Osteomalacia, especially in the pelvis and hip.[21]
Osteoarthritis
People with MetS are associated with OA more than those who do not have it. The VDD is common and associated with knee OA in an adult population. Moderate evidence of a positive association between VDD and the progression of OA was reported.[22,23]
Plain radiographs are usually used to diagnose OA, but they are unable to detect early changes in OA. Simultaneous use of 18F sodium fluoride (18F-NaF) positron emission tomography/magnetic resonance imaging (PET/MRI) is a new radiological technique to detect knee abnormalities unseen on MRI. It was found to be a promising tool for detecting early metabolic changes in OA and classifying osseous metabolic abnormalities in knee OA.[24]
Sarcopenia
Sarcopenia is an MSK disorder characterised by progressive loss of muscle mass and strength, particularly in the elderly population. It is associated with a greater incidence of falls, leading to an increased risk of fractures, and often leads to loss of independence in older individuals. Sarcopenia can be diagnosed by checking the muscle strength, quantity or quality, and physical performance. Factors contributing to its development include decreased type II muscle fibre size and number, inactivity, obesity, IR, reduced androgen and growth factor serum concentrations, and inadequate protein intake.[25] Testing the handgrip strength (HGS) is reliable and cost-effective.[26] Sarcopenia has become an increasingly studied condition, in the recent past.[27]
Association of MetS and MSK Diseases
The association between MetS and MSK disorders represents a fascinating and complex interplay that significantly impacts public health and individual well-being. This syndrome does not only elevate the risk for cardiovascular diseases and DM but also has a profound linkage with various MSK disorders. The MSK disorders, encompassing a wide array of conditions affecting muscles, bones, and joints, have been shown to associate with MetS strongly. The underlying mechanisms of this association are multifaceted and include shared risk factors, inflammatory pathways, and IR, among others.[28]
One of the most notable associations is observed with OA, as its prevalence is significantly higher in individuals with MetS. This can be attributed to the increased mechanical stress on joints due to obesity—a usual component of MetS—and systemic inflammation induced by metabolic abnormalities.[22]
Another critical area of concern is the relationship between MetS and osteoporosis. IR is a hallmark of MetS and has been implicated in the development of osteoporosis, as it disrupts the bone remodelling process, leading to decreased bone formation and increased bone resorption, thereby weakening the bone architecture.[14]
Furthermore, the association between MetS and rheumatoid arthritis (RA), an autoimmune inflammatory joint disorder, has been increasingly recognised. Patients with RA are more likely to exhibit features of MetS, which not only exacerbates joint damage but also heightens the risk of cardiovascular diseases in these patients.[28]
Inflammation plays a central role in linking MetS with MSK disorders. Adipose tissue in individuals with MetS secretes pro-inflammatory cytokines, such as tumour necrosis factor-alpha and interleukin-6, which can contribute to the pathogenesis of MSK disorders by promoting inflammation and joint degradation. The interconnection between MetS and MSK disorders emphasises the importance of adopting a holistic approach to managing patients with these conditions. Lifestyle interventions, including diet, exercise, and weight management, are pivotal in controlling MetS and, by extension, may mitigate the severity of MSK diseases. Moreover, early detection and management of metabolic abnormalities in patients with MSK disorders could help in alleviating the overall disease burden and improving outcomes.[29]
Disparities in Metabolic MSK Disorders Between Developing and Developed Countries
Though metabolic diseases have a predictable progression, various factors may lead to disparities amongst various countries. A complex interplay of socioeconomic factors, lifestyle choices, healthcare access, infrastructure challenges, misdiagnosis, social stigma, environmental factors, and genetic predisposition influences the disparities in metabolic diseases between countries.
Key Factors
A general overview of the key factors contributing to differences in metabolic and MSK diseases between developing and developed countries is presented in Table 2.
Disparities in Metabolic Musculoskeletal Diseases Between Developing and Developed Countries
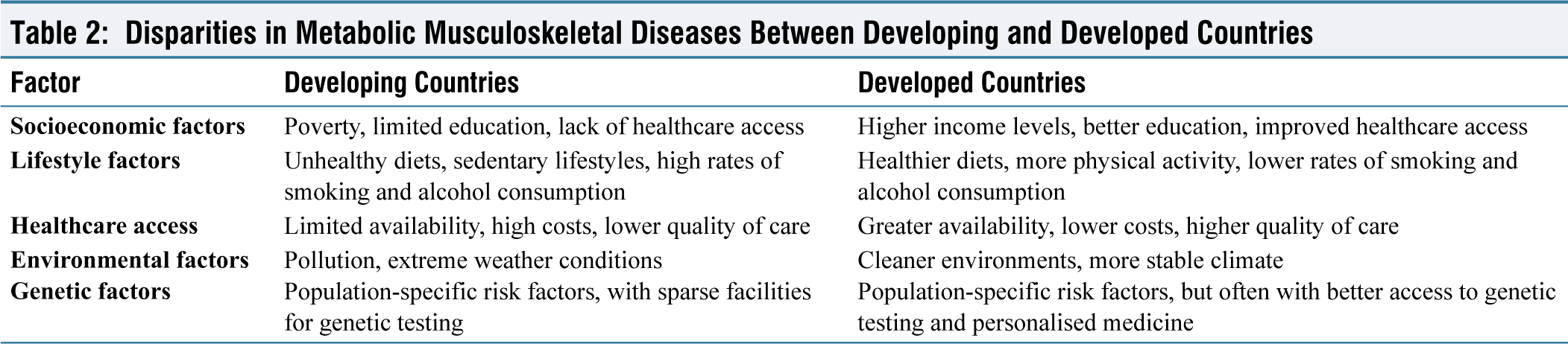
Metabolic diseases often follow a predictable course and exhibit significant disparities between countries. Many factors, ranging from socioeconomic conditions to environmental influences, contribute to these disparities.
Socioeconomic factors play a pivotal role. Poverty, characterised by limited access to healthcare, nutritious food, and safe housing, increases the risk of metabolic diseases. Inadequate health education and awareness can lead to delayed diagnosis and inadequate management. Lifestyle factors also contribute significantly. Consuming highly processed foods, sugary drinks, and unhealthy fats can lead to obesity and metabolic diseases. Inadequate physical activity and sedentary lifestyles, common in developing countries, increase the risk of obesity and associated health problems. Smoking and alcohol consumption can exacerbate these conditions.[30]
Limited healthcare access is another significant factor. In developing countries, the cost and quality of care may be lower due to a lack of trained professionals and outdated equipment. Lack of awareness itself is a significant drawback. Infrastructure challenges can hinder access to healthcare services. Poor transportation and electricity can limit accessibility. Misdiagnosis can occur due to limited resources and training, leading to incorrect identification of metabolic MSK diseases. Social stigma associated with these diseases can prevent individuals from seeking treatment.
Environmental factors, such as pollution and extreme climates, can affect access to food and water, leading to malnutrition and other health problems. Genetic factors in specific populations may predispose individuals to metabolic diseases.[31]
Addressing Disparities
Addressing disparities in metabolic MSK disorders between developed and developing countries requires a comprehensive approach [Table 2]. Expanding healthcare coverage, increasing the availability of specialised services, and reducing healthcare costs are essential for improving access to care. Public health interventions, such as promoting healthy lifestyles, improving nutrition, and increasing physical activity, can significantly reduce the risk of these diseases. Disease prevention and early detection through screening programmes and community-based interventions are also critical.
Addressing social determinants of health, including poverty, education, and environmental factors, is crucial for reducing health disparities. Collaborating with private sector organisations through public-private partnerships can enhance healthcare access and quality. Developing and implementing cost-effective treatment strategies is essential for ensuring sustainable and equitable healthcare delivery. Investing in research and development to better understand the causes and prevention of metabolic MSK disorders in developing countries is also vital.[32]
Specific Challenges and Solutions
DM, a prevalent metabolic disease in developing countries, often faces the challenge of underdiagnosis [Table 3]. Implementing mass screening programmes, promoting healthy lifestyles, and improving access to affordable insulin can address this issue. Gout, another metabolic disease, frequently leads to joint damage and kidney stones due to delayed diagnosis and treatment. Raising awareness about gout, providing early diagnosis and treatment, and improving access to medications are crucial solutions.
Challenges and Solutions in the Diagnosis and Management of Metabolic Musculoskeletal Diseases in Developing Countries
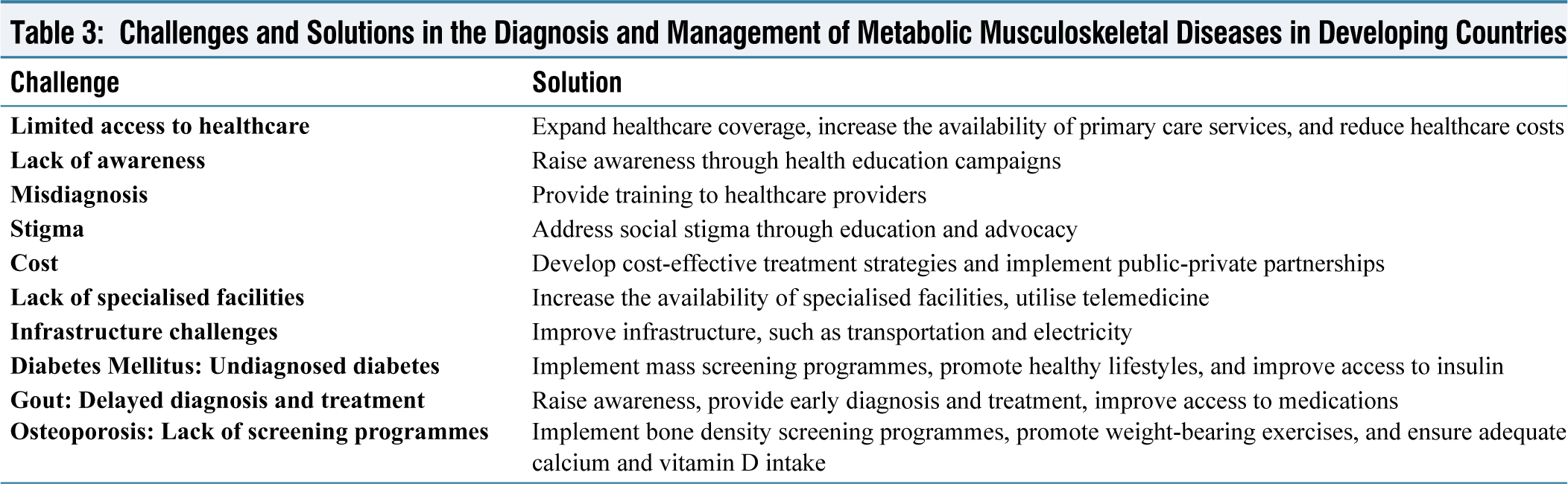
Osteoporosis, a silent disease that often goes undiagnosed due to a lack of screening programmes and limited access to bone density tests, poses significant challenges. Implementing bone density screening programmes, promoting weight-bearing exercises, and ensuring adequate calcium and vitamin D intake are essential to address these challenges.
By effectively addressing these specific challenges and implementing appropriate solutions, substantial improvements can be made in developing countries’ diagnosing and managing metabolic MSK disorders.
Research Gaps and Future Directions in Metabolic MSK Diseases
Despite significant advancements in understanding and treating metabolic MSK disorders, several research gaps must be addressed. Addressing these gaps is crucial for improving patient outcomes and developing more effective therapies [Table 4].
Research Gaps and Future Research Directions
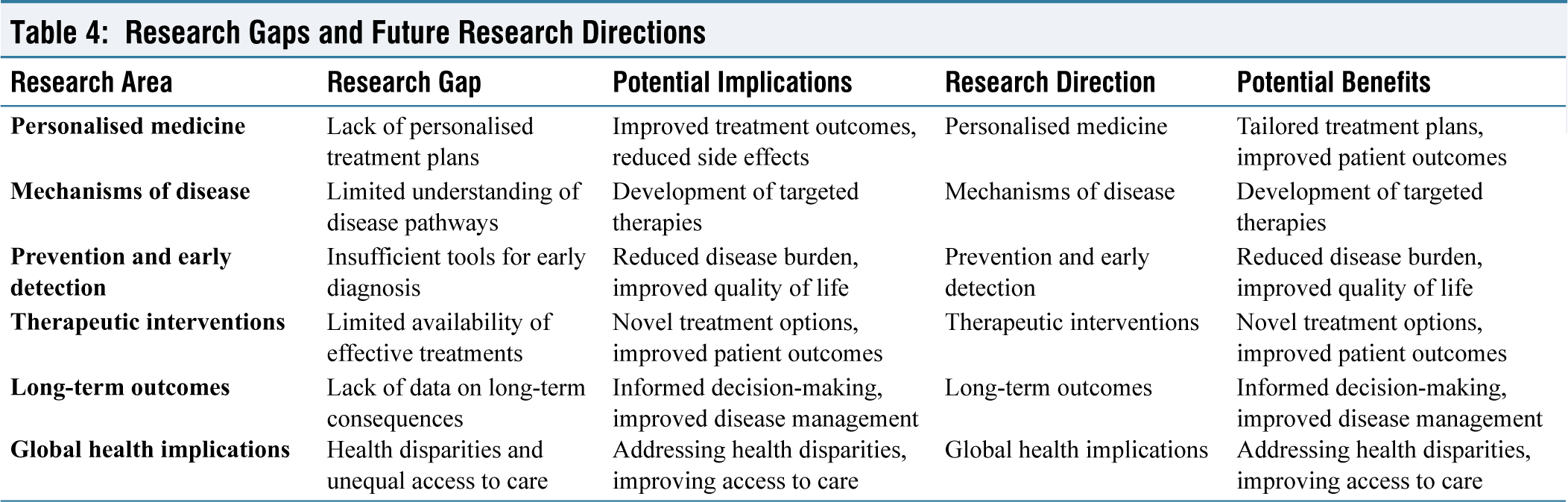
Personalised medicine, tailored to individual genetic profiles, is an emerging area that requires further research. The role of genetic variations in disease susceptibility and progression remains poorly understood. Understanding the intricate interplay between metabolic disorders and MSK tissues and the specific cellular and molecular mechanisms involved in disease development is essential for targeted therapies.
Identifying early-stage markers and risk factors for metabolic and MSK diseases is crucial for preventive interventions. Developing practical screening tools and guidelines is essential for early detection and timely management. Exploring new therapeutic approaches, including drug repurposing, gene therapy, and regenerative medicine, is necessary to address unmet clinical needs. Investigating the efficacy of combining different therapeutic modalities to improve outcomes is also essential.
Understanding the long-term consequences of metabolic MSK disorders and their impact on quality of life is essential for effective management. Developing strategies to prevent or delay the onset of complications, such as fractures, joint damage, and disability, is crucial. Conducting global epidemiological studies to assess the burden of metabolic MSK disorders in different populations is essential. Examining the influence of cultural and socioeconomic factors on disease prevalence and outcomes is also crucial.[33]
By addressing these research gaps, significant advances can be made in the understanding and treatment of metabolic MSK diseases, leading to improved patient outcomes and a better quality of life.
Limitations of the study
This review, while comprehensive, is not without limitations that must be acknowledged. First, the reliance on articles published in English and freely available may introduce a selection bias, potentially overlooking relevant studies published in other languages or behind paywalls. Second, the focus on human studies, while necessary for applicability, limits the inclusion of animal model studies that might offer valuable mechanistic insights into the relationship between MetS and MSK disorders. Lastly, the dynamic nature of MetS and its components, alongside the heterogeneity of MSK conditions, complicates the ability to draw firm conclusions, suggesting a need for more targeted and longitudinal studies to fully comprehend these complex interactions.
Conclusion
The intricate relationship between MetS and MSK disorders emphasises the importance of an integrated approach to diagnosis and management. As this review highlights, conditions such as DM, gout, osteoporosis, and others significantly impact MSK health, leading to a range of debilitating symptoms. Early identification and comprehensive management of MetS components can mitigate these effects, improve quality of life, and decrease the risk of further complications. It is imperative for healthcare professionals to consider the metabolic underpinnings of MSK disorders in their clinical assessments and treatment plans. Through interdisciplinary collaboration and patient education, better management of these complex conditions can be offered to improve outcomes and enhance well-being of those affected.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional Ethical Committee Approval Number
Ethical permission was not applicable for this article, as this is a review article drafted from various research articles and not from patients directly.
Patient consent
Consent was not applicable, as this is a review article compiled from various research articles and guidelines and not from patients directly.
Credit author statement
AV, RV- Conceptualization, data collection and analysis, literature search, manuscript writing, editing and final approval.
AV, RV, KPI- Literature search, data collection and analysis, manuscript writing, references, editing, supervision, and final approval.
Data availability statement
The data availability statement is not applicable as no datasets were generated or analyzed during the current study.
Use of artificial intelligence
We used Grammarly to enhance the English grammar and readability of the article, but all the text, figures are original and have been rechecked and approved by the authors.