
Abstract
Background and Aims:
This study examines whether the level of the conus medullaris affects the incidence of cerebrospinal fluid (CSF) leaks in spinal surgery.
Material and Methods:
Retrospective analysis was performed on 55 patients who had suffered from CSF leaks post-operatively. The data was stratified by spinal pathology, age, and sex using patient records and MRI scans/reports.
Results:
The results show that more patients with a CSF leak had surgery for disc pathologies as opposed to spinal stenosis. Additionally, patients with spinal stenosis were generally older, and there were more women in the CSF leak cohort. Notably, patients with disc pathologies had a higher conus level than those with spinal stenosis, with no CSF leaks occurring in patients with low-lying conus levels at or below L3.
Conclusion:
We did not find any correlation between level of conus and CSF leaks.
Introduction
As with any major procedure, spinal surgery carries risks from common and relatively minor to rare and potentially very serious. These can include thromboembolisms, excessive bleeding, the disruption of nervous structures and subsequent wound infection.[1] When working in close proximity to the spinal cord, many complications stem from damage to the dural layer or other non-ligamentous/non-bony structures. Naturally, a dural tear could result in a leak of cerebrospinal fluid (CSF) which can complicate care on the table as well as post-operatively. These have an estimated incidence of 0.5%–18% intraoperatively,[2] with subsequent leaks occurring without obvious durotomy in a minority of cases. Both can disrupt wound healing but also increase the risk of life-threatening infections including meningitis.[3] A large enough leak can cause reduced intracranial pressure, further worsening prognosis and adding another dimension to the post-procedural care.
When discussing CSF leaks in the context of spinal surgery, it is important to consider the anatomy of not only the spine itself but also the nervous structures within. The cord, terminating in the conus medullaris, is not usually implicated in the causes of CSF leakage with incidental durotomy being a more likely culprit.[4] However, with a certain amount of anatomical variation present within the population, it is important to rule out whether the cord may play a role in increasing the risk of CSF leaks. The conus, as previously stated, comprises the terminal segment of the spinal cord. Subsequent continuations of the pia mater and spinal nerves lie within the canal following this juncture, with the latter forming the cauda equina.[5] In the general population, the level at which this termination occurs is accepted to be around the L-1 vertebrae, with a termination at or below the L-3 vertebrae considered low-lying.[6]
There is currently an absence of research examining the relationship between a low-lying conus and CSF leak incidence; therefore, this article has been developed to identify patterns in the data and shine a light on any potential correlative affects.
Material and Methods
This retrospective study aimed to determine whether the presence of a low-lying conus-medullaris predisposed patients undergoing spinal surgery to dural tears. 88 cases where a potential intra-operative dural tear had been reported at the xxxx tertiary orthopaedic hospital between August 2008 and May 2024 were selected. Inclusion criteria were dural tears confirmed by whole spine MRI. Duplicate cases from the same patient were excluded from the study. Inclusion and exclusion criteria left 55 individual patients with confirmed dural tears for data collection. Participant characteristics of age and sex were collected as well as the date of event. The entire MRI of the lumbar spine (sagittal and axial T2 MRI images in particular) was reviewed to find the level of the conus medullaris. Participants were divided into two cohorts, those who had surgery for spinal canal stenosis and those who had surgery for disc pathology. Data from each patient was compared to radiology reports for each MRI to ensure the validity of the results. Data was recorded in Microsoft Excel, which was then used to create a summary table of the results.
Results
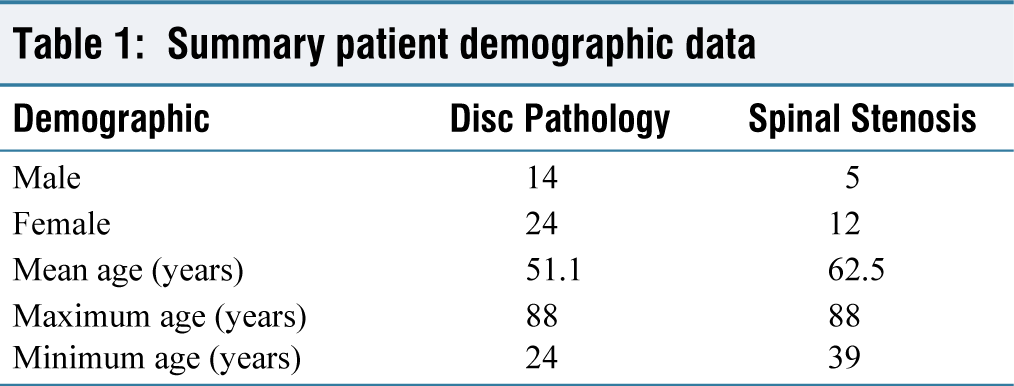
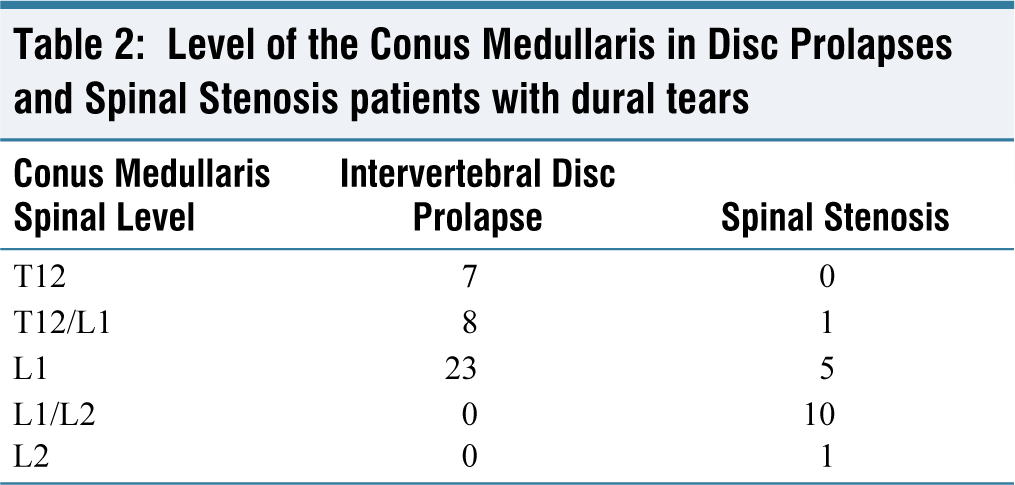
Table 1 shows the age and sex of patients with both intervertebral disc pathologies or spinal stenosis who had confirmed dural tears during surgery. 38 patients with dural tears had disc prolapses compared to 17 that had spinal stenosis. The mean ages in these categories were 51.1 and 62.5 years, respectively. Table 2 shows the level of the conus medullaris in patients with disc pathology and spinal stenosis. The mode conus medullaris level in all patients was L1 (n = 28). When separating the disc pathology cohort and spinal stenosis groups, mode conus levels were L1 (n = 23) and the L1/L2 disc (n = 10), respectively. No patients with dural tears had a low-lying conus below L3. The highest spinal level of the conus was T12 (n = 7) and occurred exclusively in patients with disc pathology; the lowest conus level was L2 (n = 1) and occurred in a patient with spinal stenosis.
Summary patient demographic data
Level of the Conus Medullaris in Disc Prolapses and Spinal Stenosis patients with dural tears
Discussion
Our data showed that no patients with confirmed CSF leaks have a low-lying conus medullaris of L3 or below. Other patterns identifiable in these results are mentioned below. There were more patients with CSF leaks in the disc pathology cohort than spinal stenosis. The mean age of patients with spinal stenosis was higher than patients with disc pathology cohort. There are more women than men within the CSF leak cohort. Patients with disc pathology had a higher mode conus than those with spinal stenosis. None of the patients with disc pathology has a conus lower than L-1.
It is well known that patients who have surgery for both disc pathology and spinal stenosis are at an increased risk of CSF leak due to the nature of the surgical interventions required to treat the pathology.[7] However, the existing literature suggests that stenotic patients suffer a higher chance of CSF leaks.[8] In fact, Strömqvist et al. describe the risk of CSF leak as ‘unquestionably lower in disc surgery than in spinal stenosis surgery’ citing ‘the less extensive procedure and the usually more voluminous spinal canal volume in disc patients’.[9] This runs contrary to our findings suggesting more disc pathology cohort patients suffering durotomy than the stenotic cohort. Bound by the retrospective nature of the article, we must be cautious in assigning correlation to this finding, however, it does represent an interesting divergence from the accepted risk ratios.
Contrary to this, our next finding is very much in keeping with the existing literature: that patients suffering from spinal stenosis possess a higher mean age than those who have surgery for disc pathology. Mostofi et al. propose that although disc prolapse is common in the elderly population, those who are symptomatic are more likely to suffer from stenosis with age. Conversely, their symptoms are increasingly less likely to be due to prolapse alone.[10] This would explain the picture we see in Table 1 that younger patients are more likely to undergo surgery for disc pathology and older for stenosis. This would naturally reflect in the incidence of CSF leaks.
We find that there are substantially more women n = 36 than men n = 19 suffering from CSF leaks following spinal surgery. This concurs with Ishikura et al., who identified female sex as being an independent risk factor for incidental durotomy during surgery.[11] Whilst it is still a matter of debate as to precisely why this is the case, many have put forward theories. Studies have investigated the thickness of the dural sac and found that there is some evidence that women have thinner dural linings, therefore increasing the risk of tears.[12] Our results seem to fit with this notion; however, we cannot completely rule out confounders. In any case, more research is required to rule out other potential causes.
With regard to conus level, we noted some interesting findings. Mode conus level appears higher in patients with disc pathology cohort (mode L1, n = 23) than spinal stenosis (mode L1/2 disc, n = 10). In addition, the conus level was not lower than L1 in the disc pathology cohort and the mode conus level for the spinal stenosis cohort was L1/L2 disc.
Given the retrospective nature of the study, we cannot with certainty prove a correlation between conus level and the risk of incidental durotomy during spinal surgery.
Limitations
We acknowledge that there are some limitations to our article. This cohort is taken from a tertiary orthopaedic centre, so is representative of different areas of the country. However, the number of patients included is limited, at 55. We would like to increase the cohort size in order to improve the reliability of our findings. Furthermore, as our study is retrospective, we may only include individuals who have had a CSF leak. In order to show true correlations in our data, a prospective study is required with an age and pathology-matched control group.
Conclusion
Incidental durotomies and CSF leaks are substantial risks in spinal surgery, having a significant impact on a patient’s outcome both on and off the operating table. It is important in the surgical field to identify what may affect these risks so that we may take steps to minimise them. Our results show that none of the patients with CSF leaks had low-lying conus.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Local ethical committee approval was obtained.
Informed consent
Informed consent was not applicable to this article, as it is a review article drafted from various research articles and does not involve direct patient data.
Credit author statement
Conception and design, or acquisition of data, or analysis and interpretation of data - Kennedy R, Botchu R.
Design, or acquisition of data, or analysis and interpretation of data - Kennedy R, Ali A, Botchu R.
Drafting the article or revising it critically for important intellectual content - Kennedy R, Ali A, Hughes S, Hassan F, Botchu R.
Final approval of the version to be published - Kennedy R, Ali A, Hughes S, Hassan F, Botchu R.
Data availability
No data is available to share.
Use of artificial intelligence
No AI was used.