
Abstract
Background and Aims:
Diabetic ketoacidosis (DKA) poses a risk for acute kidney injury (AKI) in children, with incidence varying across different regions and populations. The aim of the study is to assess the proportion and predictors of AKI in children with DKA and to assess the impact of AKI on the duration of hospital stay and recovery from metabolic acidosis.
Methods:
Medical records of children under 14 years admitted with DKA between 2021 and 2023 were analysed retrospectively. Data on clinical characteristics and outcomes were collected and analysed using descriptive and inferential statistics.
Results:
Out of 31 patients, 7 (22.6%) developed AKI. Statistically significant differences were found between the AKI and non-AKI groups in terms of age, body mass index, corrected sodium and blood urea levels. Children with AKI had a longer median duration of hospital stay (10 vs. 6 days, P = .002) and a longer time to recover from metabolic acidosis (96 vs. 39 hours, P = .001) compared with those without AKI.
Conclusion:
A significant proportion of children with DKA are affected with AKI, leading to prolonged hospitalisation and delayed recovery from metabolic acidosis. Identifying predictors of AKI can help in the early recognition and management of this complication, improving patient outcomes.
Keywords
Introduction
Children and adolescents are affected by type 1 diabetes; most of them may present with diabetic ketoacidosis (DKA). About 0.5 million new cases of type 1 diabetes are diagnosed with a median age of onset of 39 years. In 2021, about 8.4 million individuals worldwide had type 1 diabetes.[1]
DKA can be a presenting feature in children with new-onset diabetes, although the incidence varies across countries ranging from 12.8% to 80% with the higher incidence in the United Arab Emirates, Saudi Arabia and Romania, and the lower incidence in Sweden, the Slovak Republic and Canada.[2] Children with established diabetes presenting with recurrent DKA are 5% to 10% per patient-year.[3]
DKA is associated with various complications resulting in mortality and morbidity. Developing countries have a higher mortality ranging from 3% to 13%.[4]
DKA can have varied degrees of volume depletion resulting in prerenal kidney injury and subsequent acute tubular necrosis. Children are more vulnerable to volume depletion than adults, as the compensatory mechanisms are not established, and with kidney injury, renal excretion of acid will not be adequate.[5] As normalisation of metabolic acidosis is important in the resolution of DKA, with acute kidney injury (AKI), the normalisation of acidosis will be hindered.
Children admitted in paediatric intensive care unit (PICU), who develop AKI in the hospital, have a longer duration of stay.[6] Children who developed AKI while admitted in PICU were independently associated with higher mortality.[7] Children after surviving AKI have long-term complications, persistent proteinuria, hypertension and chronic kidney disease.
The prevalence of AKI in children with DKA is variable among different studies, ranging from 7.2% to 65%. This study was carried out with the aim of knowing the proportion and predictors of AKI in children with DKA. We also aimed to study the impact of AKI on the duration of hospital stay and recovery from metabolic acidosis.
Methods
Data Collection
Data were collected from the medical records of children with age younger than 14 years admitted to the Department of Paediatrics with DKA from 2021 to 2023 retrospectively. Children who were initially treated outside with fluids and those whose medical records were missing were excluded. Data collection included age at diagnosis, sex, body weight, episodes of
Children with blood glucose >200 mg/dL, venous pH <7.3 or serum bicarbonate <18 mEq/L and increased urine or blood ketones were considered as DKA.
Kidney Disease Improving Global Outcomes criteria as a creatinine level >1.5 times the baseline creatinine level were used to define. Previous baseline creatinine will not be available, and it was derived as expected baseline creatinine using eGFR of 120 mL/min/1.73 m2 and patient height. Patients were divided into no AKI, mild AKI creatinine more than 1.5 to 2 times the expected baseline creatinine and severe AKI creatinine more than 2 times the expected baseline creatinine. Children with DKA were treated as per international society for pediatric and adolescent diabetes (ISPAD) protocol. Children with AKI were managed according to severity.
Statistical Analysis
The data were analysed using descriptive and inferential statistics. Continuous variables were expressed as median and interquartile range, given the non-normal distribution of the data, as assessed by the Shapiro–Wilk’s test. Categorical variables were summarised as frequencies and percentages. The Mann–Whitney’s U test was employed to compare differences in continuous variables between the AKI and the non-AKI groups due to the data’s skewed distribution. For categorical data, the chi-square test or Fisher’s exact test was used, depending on the expected frequencies in the contingency tables. These tests were applied to evaluate the distribution of categorical variables such as gender and the presence of new-onset diabetes among the study groups. The correlation between clinical variables and outcomes was assessed using Spearman’s rank correlation coefficient, considering the ordinal nature of some of the clinical data and the non-parametric distribution of the variables. A P value of less than .05 was considered statistically significant for all tests. All statistical analyses were conducted using SPSS version 26.0 (IBM Corp., Armonk, New York, United States) or a similar statistical software package capable of handling non-parametric data analysis.
Results
In total, 38 cases were identified as DKA between 2021 and 2023, out of which seven cases were excluded due to initial management being done in another hospital and incomplete records. Twenty-nine per cent of cases were between 6 and 9 years, and 64% were more than 10 years. Sixteen cases (51%) were male, and a new onset of diabetes was present in 20 cases (64.5%). Out of 31 patients admitted with DKA, seven patients (22.6%) developed AKI. The clinical characteristics and laboratory findings were compared between the AKI and non-AKI groups, and the differences in age, body mass index (BMI), corrected sodium and blood urea between the AKI and non-AKI groups were statistically significant [Table 1]. There were no obvious reasons for a child on treatment for diabetes to develop DKA.
Demographic and laboratory findings between AKI and non-AKI groups

aStatistically significant.
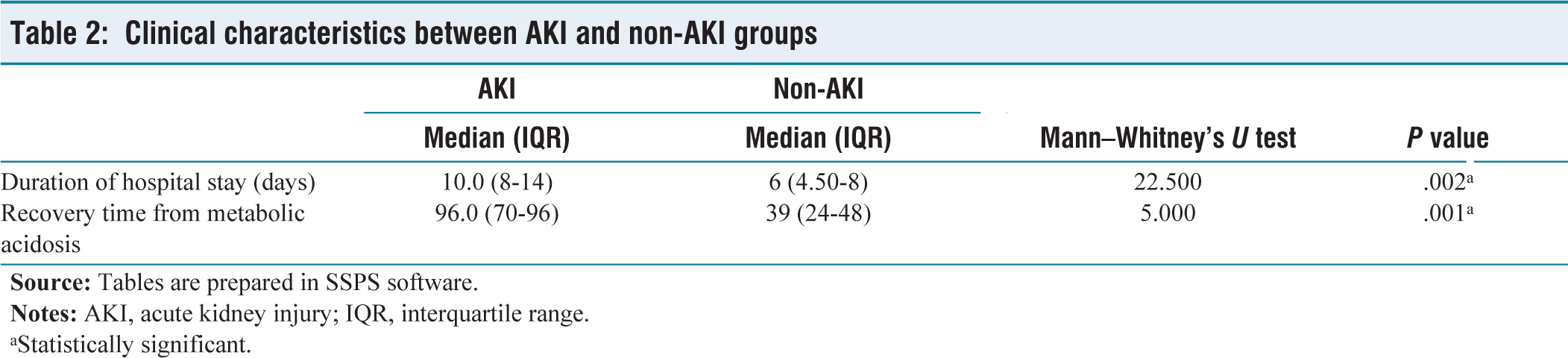
The median duration of hospital stay in the AKI group was 10 days (8-14) statistically significant as compared with non-AKI group’s 6 days (4.5-8). The median time taken to recover from metabolic acidosis was 96 hours (70-96) statistically significant as compared with non-AKI group’s 39 hours (24-48) [Table 2].
Clinical characteristics between AKI and non-AKI groups
aStatistically significant.
Discussion
In this study, 22.6% of children admitted with DKA had AKI which is similar to studies done in developing countries. A study done in India by Baalaaji et al.[8] reported that 35% of children admitted with DKA had AKI. According to a study done by Kanwal et al.,[9] 7.2% of children with DKA developed AKI.
A prospective study done in Italy[10] compared the prevalence of AKI in Type 1 DM with and without DKA. About 65.2% of T1DM patients with DKA developed AKI; 33.3% reached AKI stage 2, and 66.7% of patients reached AKI stage 1. A total of 1,359 DKA episodes were studied by Huang et al.,[11] and AKI occurred in 584 episodes (43%; 95% confidence interval [CI], 40%-46%). A total of 252 AKI events (43%; 95% CI, 39%-47%) were stage 2 or 3.
A study done at the Mackay Children’s Hospital, Taiwan[11] reported AKI in 56.5% of patients who had DKA episodes; mild and severe AKIs were found in 38.5% and 18.0%, respectively.
Hursh et al.’s[12] study showed that 64.2% of patients developed AKI during admission. Of those with AKI, 34.9% were of AKI stage 1, 45.3% were of AKI stage 2 and 9.8% were of stage 3. In a study done in Israel,[13] of the 82 children, 24 (30%) had AKI: 18 (75%) stage 1, 5 (21%) stage 2 and 1 (4%) stage 3.
In our study, we compared the clinical characteristics of the AKI and non-AKI groups, and the differences in age, BMI, corrected sodium and blood urea were statistically significant. According to Hursh et al.,[12] adjusted analysis showed that a lower serum bicarbonate level of less than 10 mEq/L increased fivefold odds of severe AKI, and an increase of 5 beats/min in initial heart rate increased 22% odds of severe AKI. Initial corrected sodium of 145 mEq/L or more increased threefold odds of mild AKI.
A study done by Huang et al.[11] showed recurrent DKA, age, higher initial glucose and sodium concentrations, acidosis and PCO2 levels were statistically more significant in children with AKI than those without AKI. These clinical characteristics show that children who were more severely dehydrated had an increased risk of AKI.
In our study, median duration of hospital stay in the AKI group was 10 days (8-14), statistically significant as compared with non-AKI group’s 6 days (4.5-8). The median time taken to recover from metabolic acidosis was 96 (70-96) hours, statistically significant as compared with non-AKI group’s 39 (24-48) hours. Baalaaji et al.[8] showed the time to resolution of acidosis in AKI group was 31 (24, 77) versus 26 (20, 35) hours, P = .006 in non-AKI group. A study done in Taiwan[11] showed no statistically significant difference in time required for recovery from metabolic acidosis.
Conclusion
This study highlights the significant impact of AKI on children with DKA in a tertiary hospital setting in South India. We found that 22.6% of children admitted with DKA developed AKI, emphasising the need for heightened awareness and monitoring for renal complications in this vulnerable population. Our findings underscore the importance of early recognition and management of AKI to prevent prolonged hospital stays and delayed recovery from metabolic acidosis. The study also identifies specific clinical characteristics, such as age, BMI, corrected sodium and blood urea levels, as significant factors associated with the development of AKI in children with DKA. These insights can guide clinicians in early identification and tailored management strategies for children at risk of AKI, ultimately improving outcomes in this population.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
The institutional ethical committee approval number is SDMIEC/2022/253.
Informed consent
The informed consent was obtained from all the participants in the study.
Credit author statement
Conception and design, or acquisition of data, or analysis and interpretation of data - Sabana S Chaukimath, Satish Tadkanhalli, Shriharsha Badiger
Design, or acquisition of data, or analysis and interpretation of data - Sabana S Chaukimath, Satish Tadkanhalli, Shriharsha Badiger
Drafting the article or revising it critically for important intellectual content - -Satish Tadkanhalli, Shriharsha Badiger
Final approval of the version to be published - Sabana S Chaukimath , Satish Tadkanhalli, Shriharsha Badiger
Data availability
Data is included in the manuscript,
Use of artificial intelligence
The use of artificial intelligence is not relevant to this article, as it does not involve AI technologies or methodologies in its analysis or conclusions.