
Abstract
Introduction:
Robotic assisted laparoscopic radical prostatectomy (RALRP) following endoscopic resection of the prostate is known to be feasible with good outcomes. However, the literature evidence is limited on the feasibility and outcomes of RALRP following open prostatic surgery. In this study, our aim was to report our experience with RALRP in patients who had undergone trans-vesical adenomectomy of the prostate in the past.
Patients and methods:
We reviewed our prospectively maintained database of men treated with RALRP at our institution to identify patients with previous history of open suprapubic trans-vesical adenomectomy, between 2016 and 2020. Data were collected on demographic information, interventions, oncological outcomes and follow-up.
Results:
Out of 362 patients, four individuals were identified that had previous open suprapubic trans-vesical adenomectomy. The mean age was 71 years with a mean pre-operative prostate specific antigen (PSA) of 11.35 ng/ml, and an average of 10 years after their trans-vesical adenomectomy. The mean console time was 119 min with an average estimated blood loss of 137.5 ml and 75% underwent lymphadenectomy. Post-operatively, all patients were discharged after 1 day with their urinary catheters removed at 7 days post-op. For one of the patients, a urine leak was identified, and his pelvic drain was removed at 5 days instead of 1 day as for the other three patients. No other complications were noted within 30 days. The average prostate weight was 54.7 g with all specimens being T3a R0. At 6 weeks follow-up, PSA was undetectable, three patients reported full continence and 1 was using two pads/day.
Conclusion:
RALRP following previous open trans-vesical prostatectomy is feasible and safe with excellent oncological outcomes. They are, however, more challenging and cumbersome with increased console time.
Keywords
Introduction
In the era of monopolar trans-urethral resection of the prostate (TURP), patients with prostate size greater than 80 g were often treated with open trans-vesical suprapubic adenomectomy, also known as Freyer’s prostatectomy. 1 Such procedure has excellent symptomatic outcome with significant and longstanding improvement in the International Prostate Symptom Score (I-PSS) and flow rate. 1 More recently with the use of bipolar and LASER technology, larger prostates can be managed endoscopically with lower risk of TURP syndrome. Advances in technology have also allowed for minimally invasive enucleation techniques (endoscopic and laparoscopic/robotic assisted) to take over the place of open adenomectomy, with equally excellent long-term outcomes. It is reported that 5–13% of patients undergoing surgical procedures for benign prostatic hyperplasia (BPH) will have incidental carcinoma of prostate on histology and some will be managed with radical prostatectomy.2,3 There is published evidence on the feasibility and outcome of robotic assisted laparoscopic radical prostatectomy (RALRP) following previous TURP for BPH4–7; however there is lack of evidence on the feasibility and safety of robotically assisted radical prostatectomy following open trans-vesical prostatectomy for BPH. We here report our experience with RALRP after open suprapubic trans-vesical adenomectomy for BPH and include a brief review of the existing literature on the topic to date.
Material and methods
We reviewed our prospective database of RALRP carried out in our department between June 2016 and March 2020 and identified those who were previously treated with open trans-vesical adenomectomy. Data was collected and analysed with regards to their demographics, intraoperative details, console time, estimated blood loss, hospital length of stay and 30 days postoperative complication rate. The pathological variables were collected as well as the 6 weeks prostate specific antigen (PSA) and continence function. The follow-up period did not include assessment of erectile function due to its short interval. Basic descriptive statistical analysis was performed with GraphPad Prism (Version 7.04, GraphPad Software Inc, San Diego, USA). For the literature review, the EBSCO Information Services, Cochrane Database of Systematic Reviews, Embase and Web of Science databases were accessed. Article selection search terms included RALRP, Freyer’s prostatectomy and open transvesical prostatectomy/adenomectomy. The authors identified articles published between 2000 and 2020 and those articles involving RALRP following open transvesical prostatectomy were selected to be included in the discussion section (n = 4).
Results
Amongst the 362 men who underwent RALRP for biopsy proven carcinoma of prostate at our institution, 4 (1.1%) were previously treated with open trans-vesical adenomectomy for symptomatic BPH. All patients had delayed diagnosis of prostate carcinoma and the mean (SD; range) time between trans-vesical and radical prostatectomy was 10 years (±1.15; 7–11 years). The mean age at radical prostatectomy was 70.5 years (±1.9; 68–72 years) with a mean pre-operative prostate specific antigen (PSA) was 11.35 ng/ml (±3.7;7.39–16.12 ng/ml). The preoperative Gleason score was 6 (3 + 3) for two patients, 7 (3 + 4) for one of them and 8 (4 + 4) for the last one (Table 1).
Patients’ pre-operative, intra-operative and post-operative data.
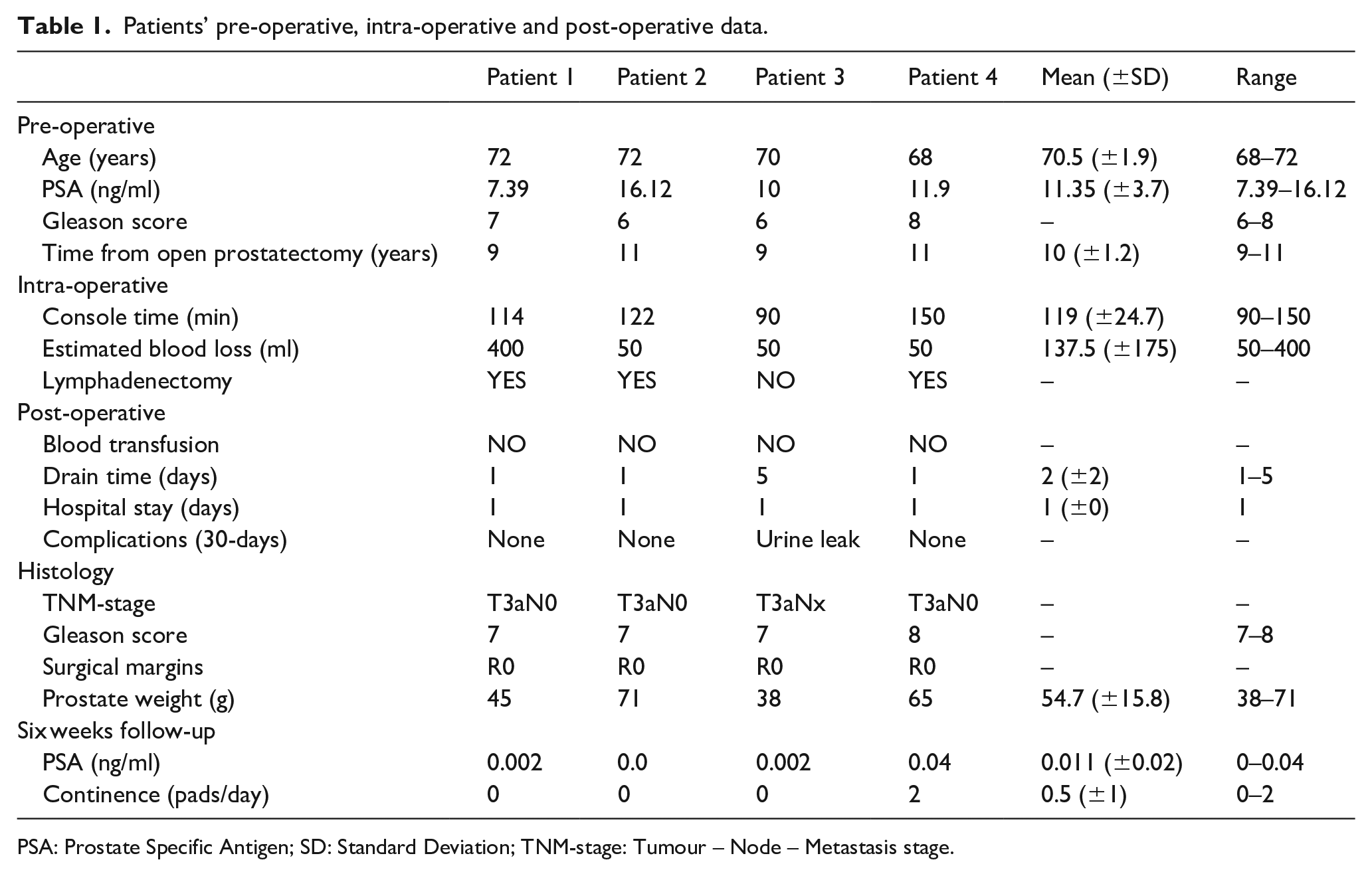
PSA: Prostate Specific Antigen; SD: Standard Deviation; TNM-stage: Tumour – Node – Metastasis stage.
All four patients had robotically assisted radical prostatectomy under general anaesthetic with the XI DaVinci robotic system (Intuitive Surgical, Sunnyvale, CA, USA). The procedures were carried out by one console surgeon with a bedside assistant through a 6-port transperitoneal approach. Intraoperative difficulties were reported on developing the retropubic space of Retzius, dividing the bladder neck, on dissecting the vas deferens/ seminal vesicles and developing the pre-rectal plane. No intraoperative complications were reported. None of the patients underwent a nerve sparing approach. The mean console time was 119 min (±24.7; 90–150). The mean estimated blood loss was 137.5 ml (±175; 50–400 ml) and no peri-operative blood transfusion was required. All four patients had a pelvic drain at the end of the procedure.
The mean postoperative hospital length of stay was 1 day. For all patients their urethral catheter was removed after 7 days. The drain was removed in three patients (75%) after 1 day and one (25%) of them was discharged to his usual residence with a drain in situ for 5 days to manage a urine leak. No other 30-day complications were reported.
On final histology from the extracted specimens, three patients had Gleason 7 (3 + 4) and one Gleason 8 (4 + 4) disease; all had T3a pathological staging with clear surgical margins. Lymphadenectomy was carried out in three patients (75%) with lymph nodes examined being clear of cancer in all cases. The mean prostate weight was 55.75 g (±15.8; 38–71 g). At 6 weeks all four had an undetectable PSA. Three (75%) reported full continence with no pads at 6 weeks whereas one needed two pads/day at 6 weeks (Table 1).
Discussion
Men treated surgically for symptomatic BPH may be diagnosed with prostate carcinoma either incidentally on histology of the BPH surgery specimen (incidental carcinoma) or at a later stage during their routine PSA follow-up (delayed carcinoma). It is reported that incidental prostate carcinomas are found in 5–13% of BPH specimens. 1 The risk of delayed prostate carcinoma in men who underwent BPH surgery in the past is the background risk of the general population for that age. Men with incidental or delayed prostate carcinomas may be offered RALRP. There are reports in the literature on the feasibility and safety of minimally invasive radical prostatectomy following endoscopic BPH related surgery and they suggest that this is feasible and safe.4–7 The evidence on the feasibility and safety of RALRP following previous open trans-vesical adenomectomy is scanty.6,8–10 The available evidence to date is limited to three case reports and a small series of five patients. The reason for the scanty available evidence may be the fact that open trans-vesical adenomectomy has these days been largely replaced by laparoscopic/robotic and endoscopic enucleation techniques. Nevertheless, open suprapubic trans-vesical adenomectomy remains a very effective treatment for symptomatic men with BPH and prostates larger than 80 g. The more advanced the age in this group of patients, especially the ones with delayed diagnosis on follow-up, makes the option of radical prostatectomy less popular and this is another reason for the small numbers of cases and reports on men undergoing radical prostatectomy following open suprapubic trans-vesical adenomectomy. On reviewing our RALRP database, we identified only those four men who had previously undergone open suprapubic prostatectomy, which represents just over 1% of the cohort. Three belonged to our centre’s cohort of trans-vesical prostatectomy patients and one was referred to us from another institution.
The mean time elapsed between the open prostatectomy and the diagnosis of prostate cancer and robotic prostatectomy was 10 years with the mean age at robotic prostatectomy being 71 years. This is a few years higher than the average age reported by most RALRP series. The median preoperative PSA was again a little higher than most robotic prostatectomy series at 11.35 ng/ml, whereas the preoperative biopsy Gleason score is comparable to other published series.
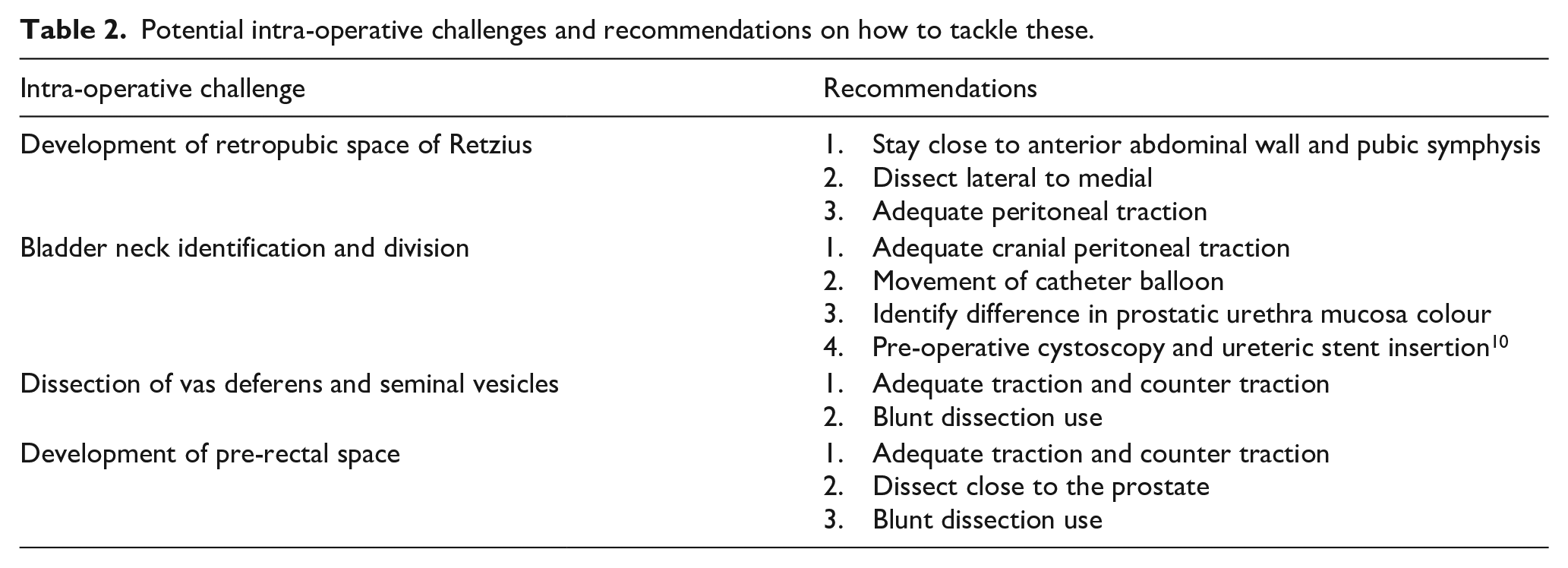
Intraoperative difficulties were first noted at the development of the retropubic space of Retzius due to adhesions between the bladder and the anterior abdominal wall (Table 2). We recommend that one should stay close to the anterior abdominal wall and lateral dissection first may facilitate the more difficult development of the space in the midline. The next difficulty appears to be at the identification and division of the bladder neck. This may be facilitated by good cranial peritoneal traction to enhance the ‘hour-glass’ shape of the bladder neck. Movement of the catheter balloon can also help at this step. Tsui et al. 10 recommend preoperative cystoscopic assessment of the bladder neck anatomy and the proximity of the ureteric orifice to the bladder neck. They go on to recommend intraoperative ureteric stenting to avoid ureteric orifice injury. We found that there is a visible colour difference between the more lively pink colour of the bladder mucosa and the more pale colour of the previously operated scarred prostatic urethral mucosa (Figure 1). This colour difference helps to decide on the division of the posterior bladder neck and prevent ureteric orifice injury. Dissection of the vas deferens and seminal vesicles has also been noted to be more challenging, as well as the dissection of the lateral and posterior pre-rectal space. Difficulties encountered during these steps may be helped by the use of blunt dissection in addition to adequate traction and counter traction. The blunt/finger enucleation technique of open trans-vesical adenomectomy usually prevents prostate capsule perforation and limits extravasation of urine and irrigation fluid and that may account for the limited periprostatic inflammation and fibrosis. All of our patients required bladder neck reconstruction. Tugcu et al. 6 report an 80% bladder neck reconstruction rate compared to only 2% in the cohort of BPH surgery naïve patients. The aforementioned difficulties seem to increase the operative/console time.
Potential intra-operative challenges and recommendations on how to tackle these.
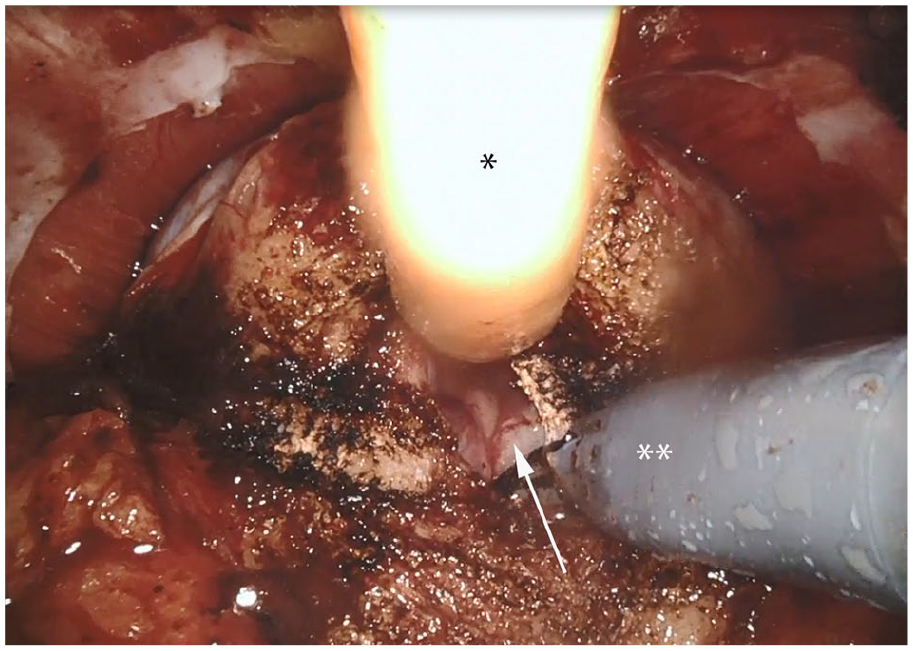
The colour difference of the paler scarred prostatic urethra mucosa (arrow) compared to the pink bladder mucosa may help in the identification and division of the posterior bladder neck, avoiding ureteric orifice injury.
In our series of robotic prostatectomies, the median console time is 90 min compared to the 119 min seen in the four patients who underwent previous open trans-vesical adenomectomy. Suardi et al., 7 in a study comparing robotic prostatectomy after Holmium LASER enucleation of the prostate (HoLEP), TURP and open prostatectomy report increased operative time in the open prostatectomy group compared to the TURP and HoLEP groups of patients. Tugcu et al. 6 compared robotic prostatectomy in BPH surgery naïve patients to a group of 25 patients who underwent previous BPH surgery; they report increased console time of 260 min in the open prostatectomy group compared to 195 min and 160 min in the TURP and BPH surgery naïve group of patients. The same study reports more blood loss of 240 ml in the open prostatectomy group of men compared to 187 ml and 116 ml in the TURP and BPH surgery naïve group of men respectively. In our series the mean estimated blood loss was 137.5 ml, which is less than the so far reported literature.
In our institution, we usually discharge patients on the first post-operative day after their RALRP, this was not an issue for our patients with previous trans-vesical adenomectomy. In one patient (25%) we observed a urine leak and he was discharged from hospital with the pelvic drain, which remained in situ for 5 days. Tugcu et al. 6 report a 12.5% urine leak rate, which they defined as urine leak that necessitated catheterisation for longer than 10 days. In our patient with the urine leak his catheter was removed as per our protocol at 7 days because his leak was judged to be minor.
Three of our patients reported full continence at 6 weeks follow-up without use of pads. This is consistent with the continence rate reported by others. Tugcu et al. 6 reported a 72% continence rate at 3 months in patients who underwent previous bladder outlet surgery. This continence rate increased to 88% at 12 months and compared to the continence rate in surgery naïve patients (75% and 80% at 3 and 12 months). The same group, as well as Suardi et al., 7 report no difference in the continence and erectile functional outcomes between patients who previously underwent transurethral or even open adenomectomies compared to patient s who did not undergo any previous surgery. Unfortunately, our reported follow-up of 6 weeks was too short to report on erectile functional outcomes.
Finally, the oncological outcome of RALRP following previous open trans-vesical prostatectomy appears not to be compromised and is comparable to the outcome of patients who did not undergo previous outlet surgery. All of our patients had specimen confined disease (T3a R0) with negative lymph nodes and an undetectable PSA at 6 weeks. Others report a biochemical recurrence of 12% at 12 months which is comparable to that reported in surgery naïve patients (11%). 6
Conclusion
RALRP following previous open trans-vesical prostatectomy is feasible and safe with excellent oncological outcomes. They are, however, more challenging and cumbersome with increased console time.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.