
Abstract
Background and Aims:
Dupuytren’s contracture is a prevalent, hereditary fibroproliferative disorder affecting the palmar aponeurosis, which can resemble various neoplastic and non-neoplastic disorders of the hand. This resemblance poses a diagnostic challenge for healthcare professionals. This observational study aims to evaluate the range of conditions that can be mistaken for Dupuytren’s contracture over a 12-year period (2008–2020) at a specialised orthopaedic oncology centre.
Materials and Methods:
A retrospective analysis of palmar lesions referred to our tertiary orthopaedic oncology hospital was conducted. Data were gathered from oncology, radiology and histopathology databases. We specifically examined lesions located solely on the palmar aponeurosis, excluding the thenar and hypothenar regions. Patient demographics, clinical features, imaging results and clinical management outcomes were documented for descriptive analysis.
Results:
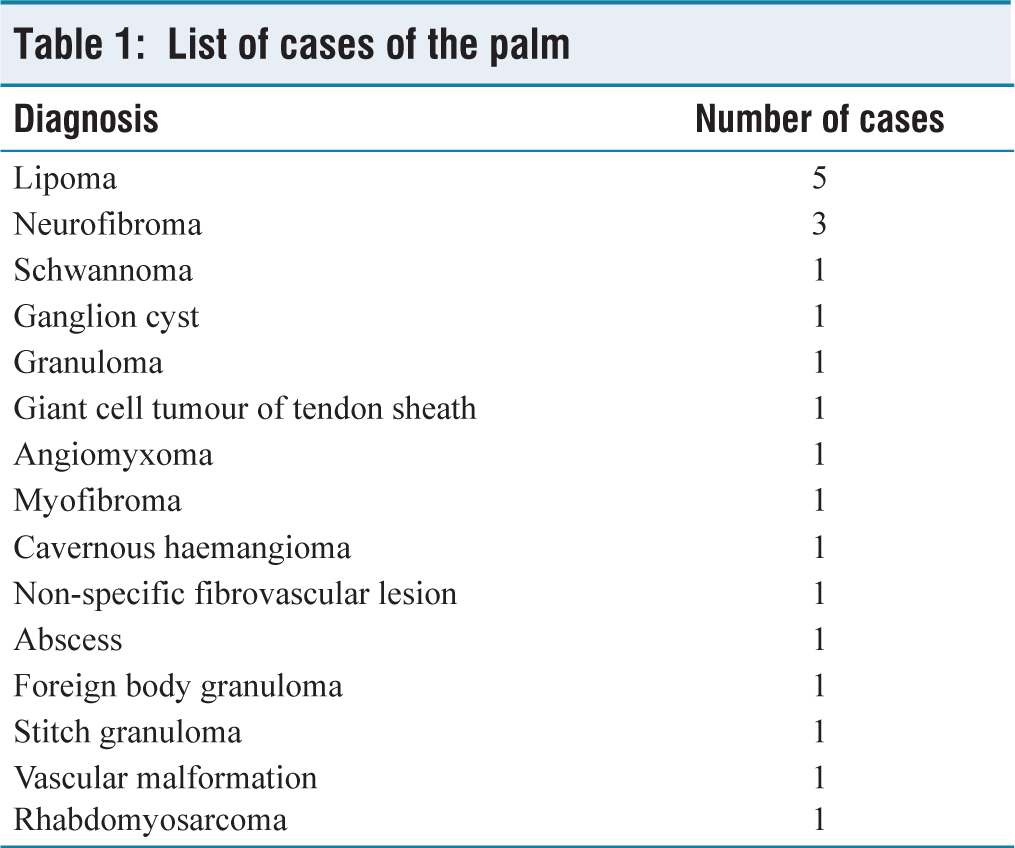
A total of 21 palmar lesions meeting the inclusion criteria were identified. The average age of the participants was 48 years (ranging from 3 to 69 years). There was no significant difference in gender distribution, with 11 females and 10 males represented in the cohort. The majority of the identified lesions were benign tumours (16), with one case of malignant rhabdomyosarcoma. Among the benign tumours, lipomas were the most common (n = 5). Other benign tumours included three neurofibromas, a schwannoma, a granuloma, a ganglion cyst, a giant cell tumour (GCT), an angiomyxoma, a myofibroma, a cavernous haemangioma, a non-specific fibrovascular lesion and four additional non-neoplastic lesions.
Conclusion:
A variety of benign, malignant or neoplastic conditions of the hand can closely resemble Dupuytren’s contracture, particularly in the initial stages of their development. A thorough clinical examination, combined with a high level of suspicion, along with supplementary investigations and histopathological analysis, is essential for accurate diagnosis and effective management of patients.
Introduction
Dupuytren’s disease (also known as Dupuytren’s contracture, DC) is a relatively uncommon condition that affects the palm and can cause significant morbidity to the working population.[1] DC originate from the palmar aponeurosis (PA), an important superficial structure in the palm. Initially, DC appears as palpable nodules and masses that are difficult to distinguish with clinical examination.[2] The differential diagnosis at the early stages is wide and may range from benign or malignant tumours to non-neoplastic lesions.[3]
We have come across several lesions within our tertiary orthopaedic oncology hospital found to affect the area over the PA which can easily be confused with DC. We, therefore, decided to perform this study and report the largest case series of lesions affecting the palmar area. We highlight the importance of awareness of such lesions in this area, to aid clinicians with the appropriate clinical diagnosis and management.
Methods
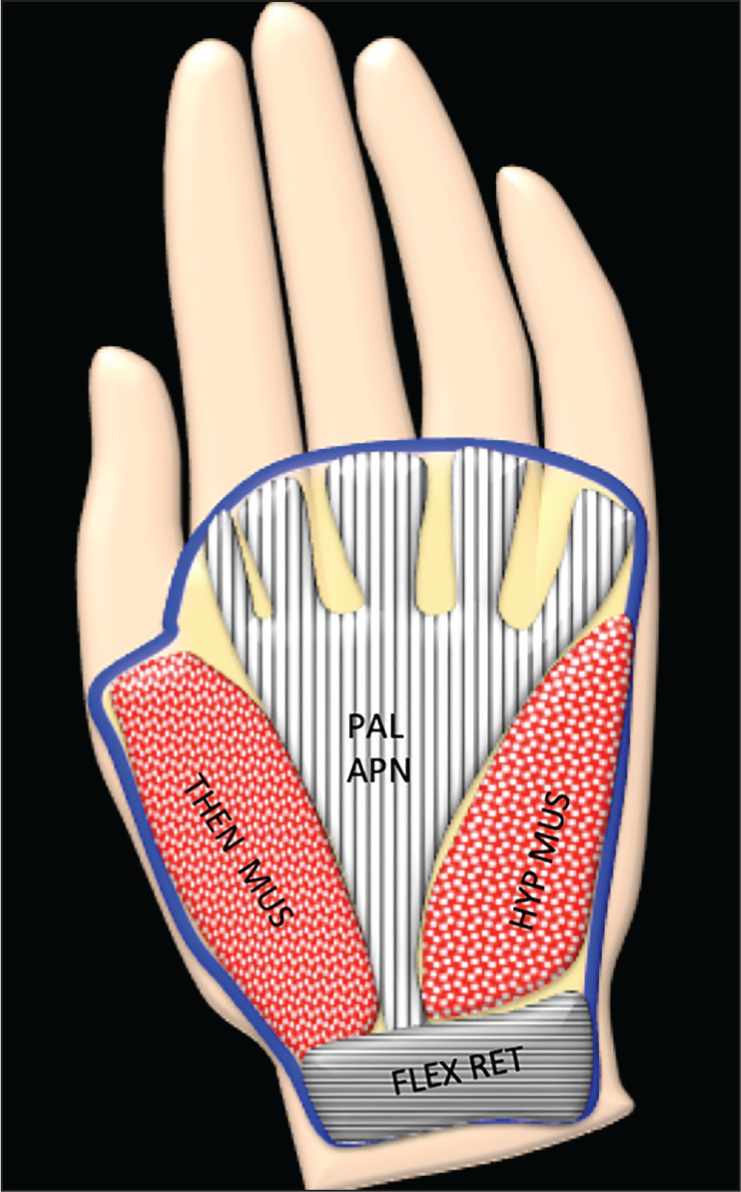
We performed a retrospective review of our oncology and radiology database for all lesions affecting the palm. We further evaluated lesions found only over the PA, with the proximal end corresponding to the origin of the PA and the distal end corresponding to the distal hand crease, excluding the thenar muscles (laterally) and hypothenar (medially) regions [Figure 1]. DC and osseous lesions were excluded from the study. A fellowship trained musculoskeletal radiologist, with 10 years’ experience, reviewed all images.
Schematic diagram showing the palmar aponeurosis overlying the palmar aponeurosis (PAL APN), THEN MUS (thenar muscles) and HYP MUS (hypothenar muscles)
Results
We identified a total of 21 lesions of the palm that fulfilled the inclusion criteria. The mean age of our cohort was 48 years (3–69 years.) There was no significant gender predominance with 11 females and 10 males within our cohort.
The majority of these lesions were benign tumours (16) and one malignant rhabdomyosarcoma within our study. The bulk of the benign tumours were lipomas (n = 5). Other benign tumours included three neurofibromas, one schwannoma, one granuloma, one ganglion cyst, one giant cell tumour (GCT), one angiomyxoma, one myofibroma, one cavernous haemangioma and one non-specific fibrovascular lesion.
The remaining four cases constituted non-neoplastic lesions, formed of an abscess, vascular malformation (VM), stitch granuloma and a foreign body [Table 1].
List of cases of the palm
Discussion
The PA is an important superficial structure in the palm that has a key role in protecting the underlying muscles and neurovascular structures and functions mainly to stabilise the skin during grasping. The PA originates from the transverse carpal ligament at the distal end of the carpal tunnel and extends distally in a triangular shape before dividing into four fibrous digital sheaths (FDS), one for each finger, anterior to the flexor tendons and sheaths.[2] The FDS are critical to the maintenance of the flexor tendons of the fingers, ensuring all finger movements are performed perfectly and efficiently.
The PA is important clinically since it can undergo fibroproliferation, a benign idiopathic condition known as DC.[4] DC is common and has geographic variability with a prevalence ranging from 0.2 to 56% worldwide. Contractures initially develop in the subcutaneous tissues, forming nodules in early stages, that later elongate into cords leading to flexion contractures.[5] Those contractures are known to cause significant psychosocial and physical morbidity, due to the limitations in daily activities.[6]
Diagnosis of DC is quite straightforward when there are deformities/contractures of fingers and cords. However, early in the disease, patients may present with palpable nodules or masses that are difficult to distinguish with clinical examination and imaging is often warranted. This case series highlights other potential mimickers of DC during the initial phases of the disease.
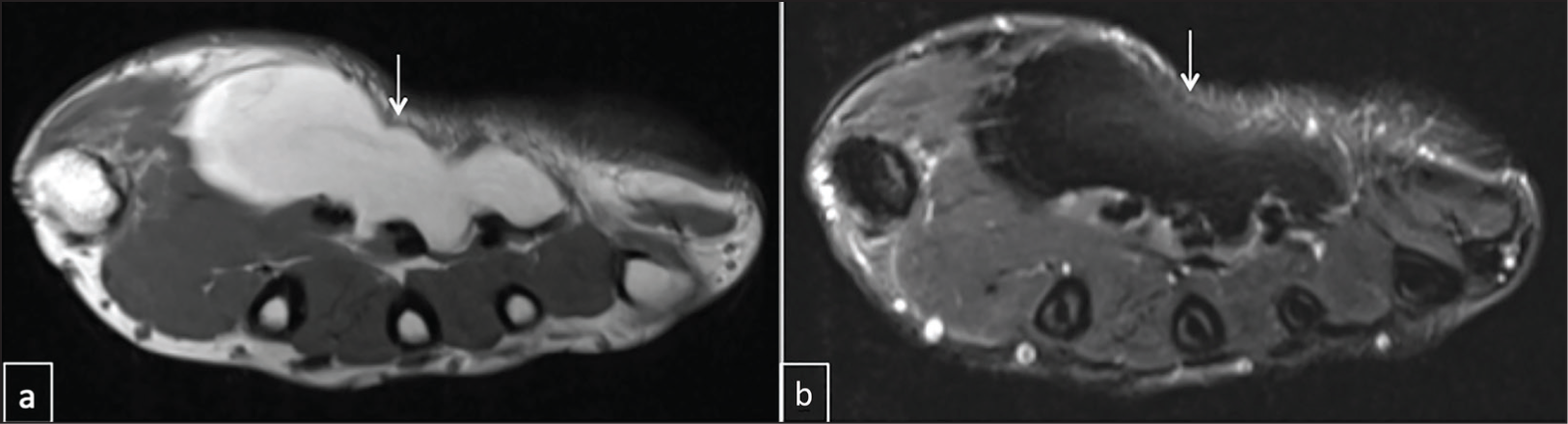
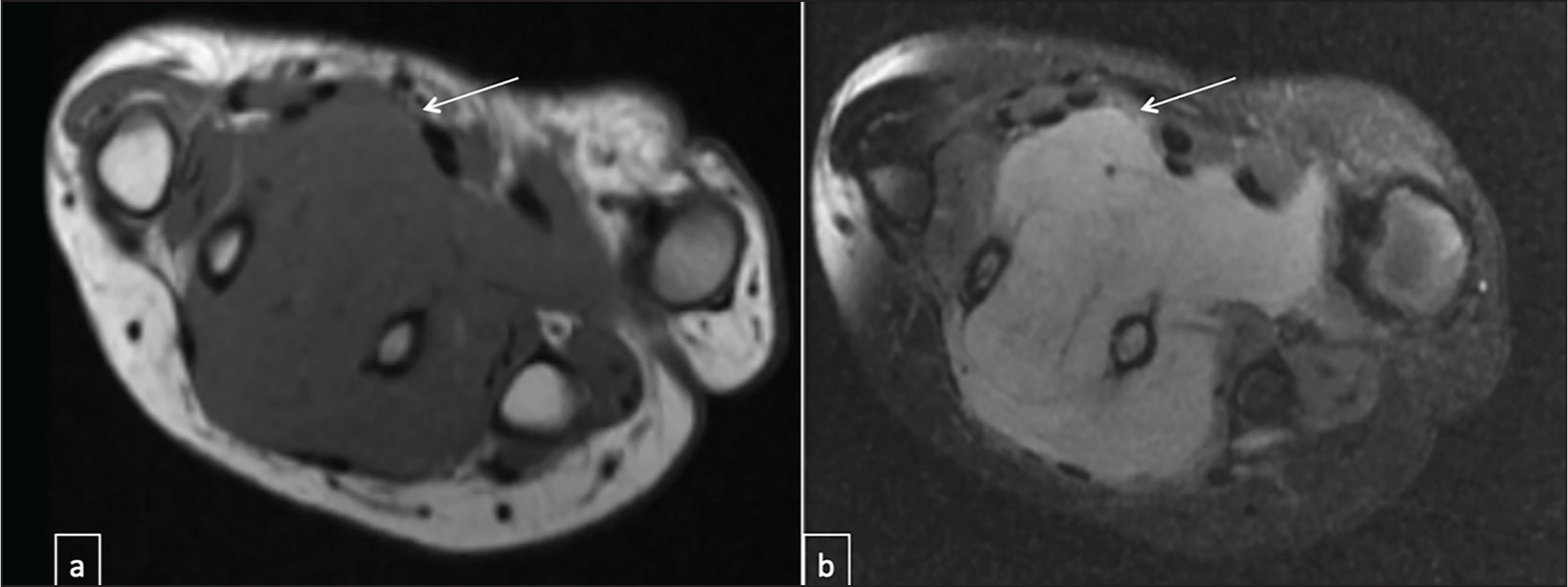
STT (soft tissue tumour) of the hand accounts for 15% of all tumours, and their incidence in the PA is unknown.[8] The most common benign tumour in our series was lipomas. Lipomas are generally the most common STT and can affect any part of the body.[7,8] However, they very rarely affect the palm and we could only identify a few case reports in the literature.[9,10] Lipomas clinically present as a mobile painless superficial lump. Rarely in the palm can they produce pain, when compressing nerves located around the deep palmar surface or carpal tunnel. These are high signal on T1 and demonstrate homogenous signal suppression on fat suppression sequences [Figure 2].
Lipoma. Axial T1 (a) and short tau inversion recovery (STIR) (b) showing large lipoma (arrow)
Other benign tumours identified within our study were peripheral nerve sheath tumours (PNST). These constitute neurofibromas and schwannomas.[11] Schwannoma are the most common benign PNST [Figure 3]. They are found in approximately 5% of all upper extremity tumours. However, they are a rare differential for hand tumours, and their incidence in the palm is unknown. Schwannomas originate from Schwann cells, often found along the course of the affected nerve. They commonly present in middle-aged adults and may present with pain or paraesthesia of the affected nerve or may be asymptomatic. Imaging appearances can be non-specific and often biopsy is required to confirm the diagnosis.[12]
Neurofibroma. Axial T1 (a) and STIR (b) showing neurofibroma (arrow)
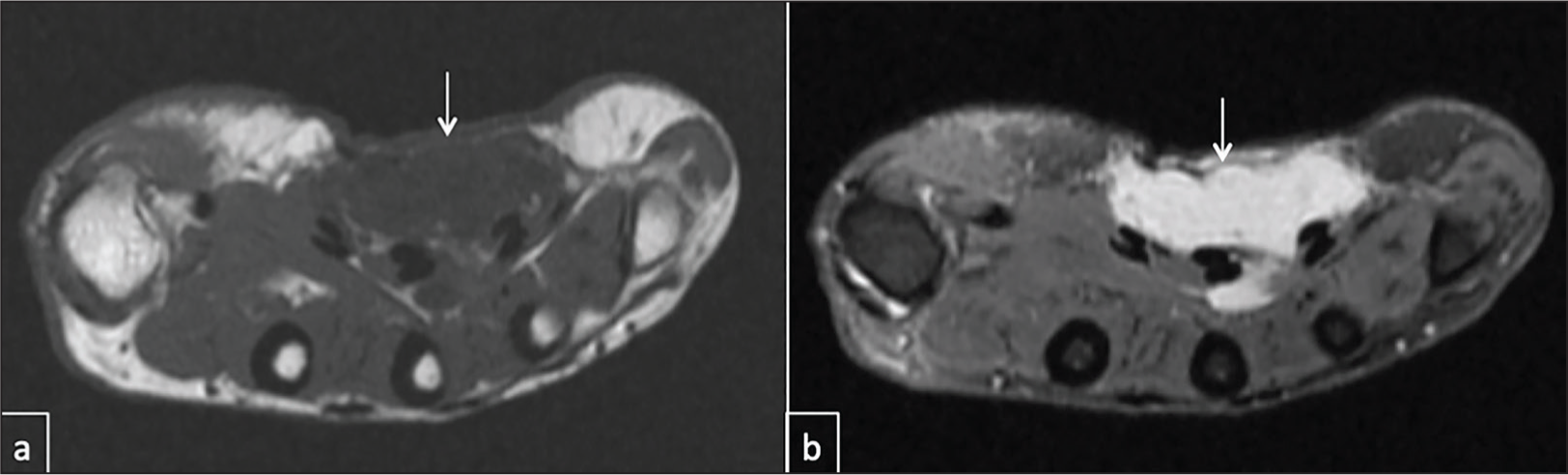
Malignant soft tissue sarcomas (STS) of the hand are rare and only found in 2% of all hand lesions.[13] We only identified a single case of rhabdomyosarcoma within our study. Rhabdomyosarcomas are the most common childhood STS constituting 50% of all paediatric lesions.[14] They are very rarely found affecting the palm, and to the best of our knowledge, we could not identify a single case in the literature. Their diagnosis is often difficult since their presentation can initially be like other STTs and imaging appearances can be non-specific.[15] [Figure 4]. These can metastasise to lymph nodes; hence, clinicians need to have a high index of suspicion in those presenting at a younger age, as late diagnosis carries a poor prognosis and outcome.
Rhabdomyosarcoma. Axial T1 (a) and STIR (b) showing large rhabdomyosarcoma (arrow)
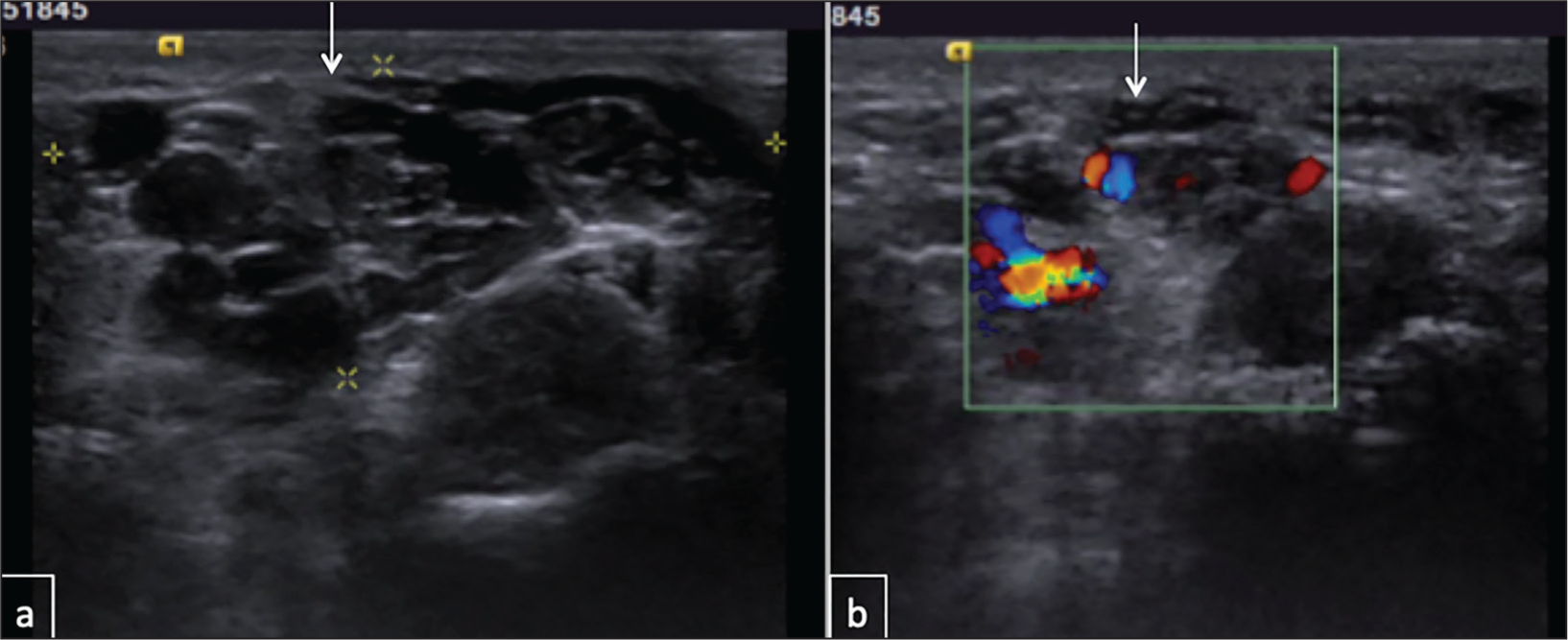
Our study also revealed other non-neoplastic lesions affecting the palm including a vascular malformation (VM), an abscess and a foreign body [Figures 5–7]. The latter two cases can easily be distinguished with appropriate history and clinical examination. VM, however, are difficult to distinguish clinically and usually warrant imaging. VM are commonly discovered during adolescence or young adulthood and affect the upper extremity in 40% of cases.[16] Their incidence in the palm is unknown. VM are formed of soft dysplastic vessels and have nonspecific symptoms, presenting as painless or painful nodules, sometimes with bluish skin discolouration. Patients suspected of having VM undergo MR imaging which usually confirms the diagnosis.
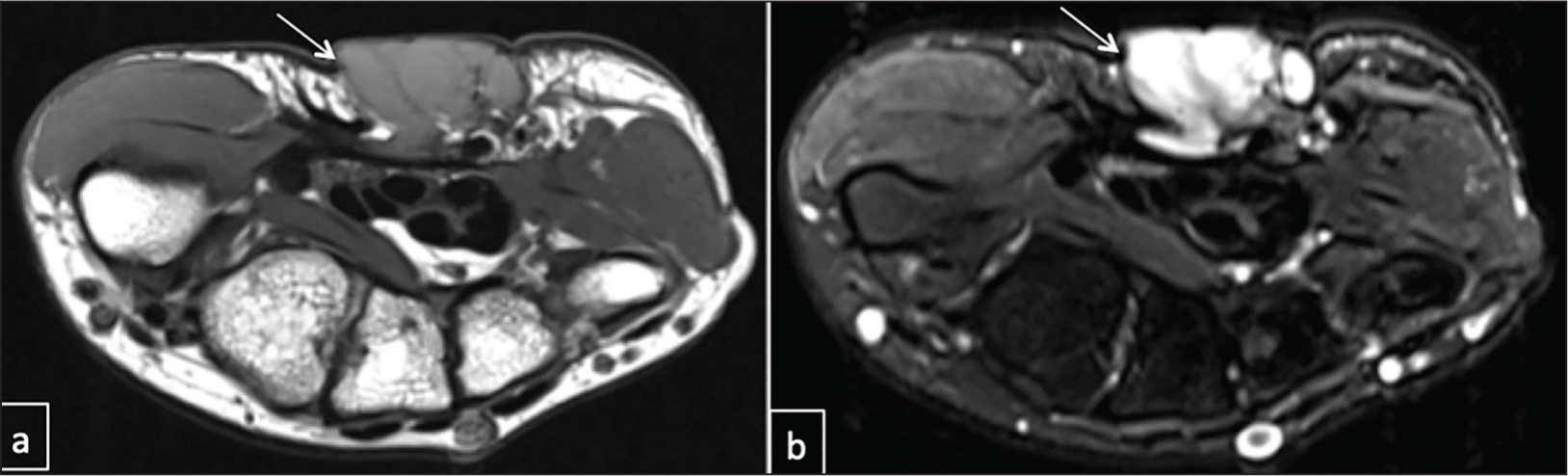
Angiomyxoma. Axial T1 (a) and STIR (b) showing angiomyxoma (arrow)
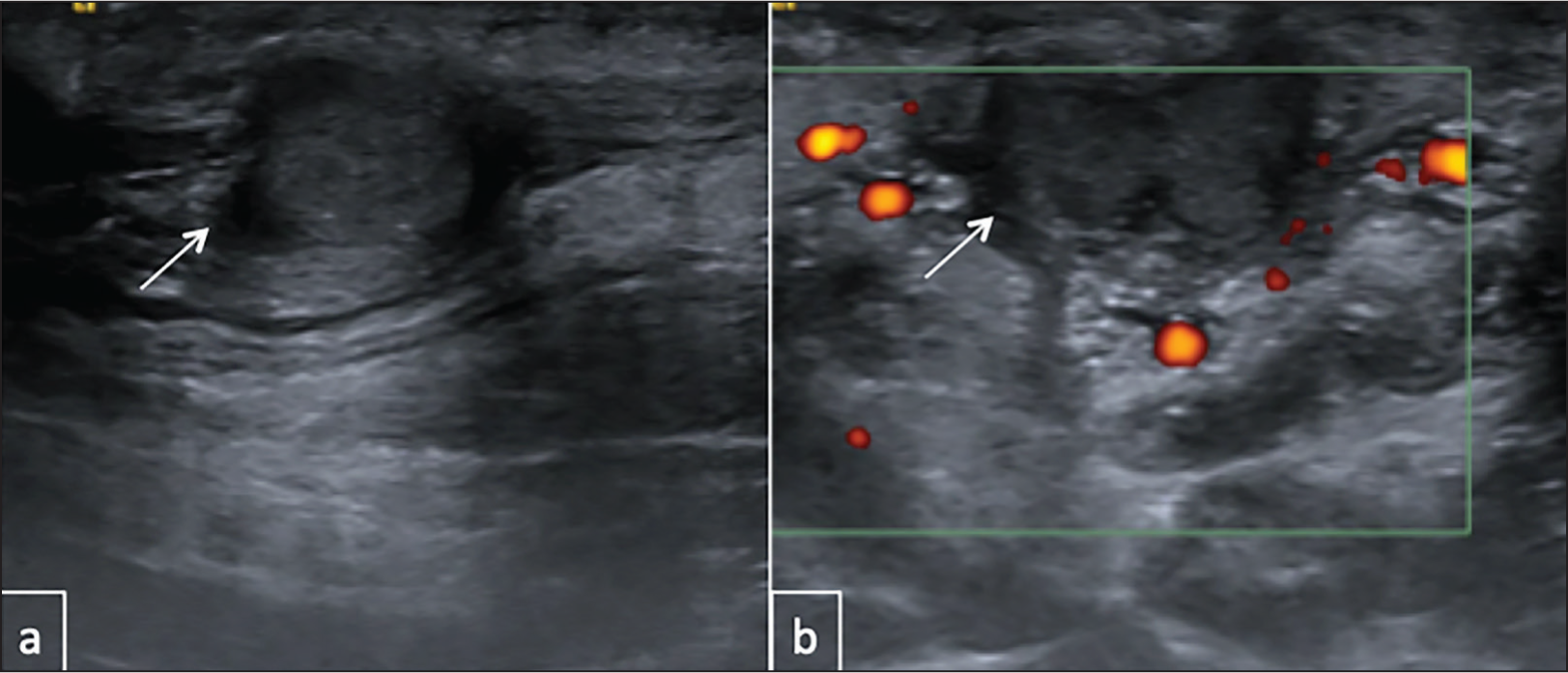
Abscess. Ultrasound image (a) showing an abscess with moderate increased signal on Doppler (b)
Vascular malformation. Ultrasound image (a) showing a vascular malformation with moderate increased signal on Doppler (b)
Conclusion
The early stages of DC can be challenging to diagnose. We report the largest case series of lesions affecting the palmar area. We highlight the importance of awareness of such lesions in this area since they can easily mimic DC.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Authors Rajesh Botchu and Karthikeyan P Iyengar are members of the Editorial Board of Apollo Medicine. The authors did not take part in the peer review or decision-making process for this submission and have no further conflicts to declare.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
This study was approved by our local committee review board as a service evaluation.
Informed consent
Anonymous data was used and local ethical committee was obtained for this study.
Credit author statement
All authors contributed to the design of the study and collected the study data.
AS wrote the first draft of the manuscript and RB is the guarantor for the study.
All authors critically revised the final manuscript, have approved the final version and agreed to be accountable for all aspects of the work.
Data availability
Data is available to share on request.
Use of artificial intelligence
No Artificial Intelligence was used.