
Abstract
Background and Aims:
Laparoscopic surgery is associated with significant haemodynamic changes due to pneumoperitoneum formation. Various studies have demonstrated that α2 adrenergic agonists, such as clonidine and dexmedetomidine, prevent the haemodynamic response due to pneumoperitoneum during laparoscopic surgery.
Methods:
A total of 104 female patients undergoing laparoscopic hysterectomies were divided into three groups at random. Group D patients were administered a loading dose of 1 μg/kg of dexmedetomidine prior to induction over a period of 15 minutes and a maintenance dose of 0.5 μg/kg/h during the surgical procedure. Group CL patients were given a loading dose of 2 μg/kg of clonidine before induction over a period of 15 minutes and a maintenance dose of 1 μg/kg/h during the surgery. Group C received same volume of normal saline over same duration and maintenance infusion throughout the surgery. The primary outcome was the haemodynamic changes at different time interval. The secondary outcome was the response to verbal commands, extubation time and orientation time.
Results:
There was no significant difference in heart rate and blood pressure values between group D and group CL during whole study period. Whereas in group C, there was a statistically significant increase in heart rate and blood pressure after intubation and during pneumoperitoneum period (P < 0.05). Extubation time and orientation time were significantly delayed in group D and group CL when compared with group C and D (P < 0.05).
Conclusion:
Clonidine or dexmedetomidine effectively attenuates the haemodynamic changes in patients undergoing laparoscopic hysterectomies compared to the control group.
Introduction
Laparoscopic hysterectomy has transformed uterus surgeries and it has now become the ‘gold standard’ for hysterectomy. It provides many advantages than open hysterectomy, like less blood loss due to less tissue damage, reduced postoperative (PO) analgesic requirements, avoiding large surgical incision, thereby allowing early recovery and mobilisation, shorter hospital stay with reduced health care cost.[1] However, this procedure is also having some risk, because it causes significant haemodynamic alterations specially in elderly and haemodynamically compromised patients. Pneumoperitoneum has an impact on different homeostatic systems, resulting in changes in acid–base balance, cardiovascular, pulmonary physiology and stress response.[2-4]
There have been various studies showing that α2 adrenergic receptor agonist like dexmedetomidine and clonidine both prevent haemodynamic changes related to pneumoperitoneum during laparoscopic surgery.[5,6] Aho et al.[7] employed α2 adrenergic receptor agonist to prevent haemodynamic changes that result from laparoscopic surgery and revealed that dexmedetomidine is effective in reducing the heart rate (HR) response after intubation and pneumoperitoneum. The release of catecholamine and vasopressin is inhibited by clonidine, which regulates the haemodynamic changes caused by pneumoperitoneum.[8] Considering all these observations, this study was designed to investigate the type and extent of haemodynamic changes associated with laparoscopic hysterectomies and to find out the efficacy of dexmedetomidine and clonidine in the prevention of such haemodynamic changes.
Materials and Methods
One hundred four American Society of Anesthesiologists physical status I and II female patients, aged 30 to 60 years, planning of laparoscopic hysterectomy under general anaesthesia participated in this prospective, double-blind, randomised trial after receiving clearance from the Institutional Ethical Committee. Patients with known sensitivity to study drug, on preoperative β-blocker therapy, any degree of heart block, systemic ailments like diabetes, hypertension, hepatic failure or renal failure were excluded from the study. Using block randomisation with variable block size, three equal groups of 32 patients were randomly allotted using a computer-generated randomised schedule.
In the operating room, preloading was done with 8 mL/kg of normal saline. An independent anaesthesiologist who was not affiliated with the study prepared all the medications, which were administered in identical syringes 20 minutes before the induction of anaesthesia (Perfusor Compact S, B Braun, Germany). Five minutes after the loading dose of study drug was terminated, anaesthesia was initiated in all groups.
We administered inj. midazolam 0.03 mg/kg, inj. fentanyl 1 µg/kg, inj. propofol 1.5–2 mg/kg and inj. vecuronium 0.1 mg/kg body weight for the induction of anaesthesia. The process of endotracheal intubation was performed using a Macintosh laryngoscope and an appropriate size endotracheal tube. To achieve a target bispectral index (BIS) of 40–60, oxygen: nitrous oxide (O2:N2O), sevoflurane and propofol infusion were used to maintain anaesthesia. The consumption of propofol was observed every hour. If there is hypertension (mean blood pressure above 20% from preoperative) or tachycardia with a BIS that maintains between 40 and 60, fentanyl 0.5 μg/kg was used. Patients were monitored throughout the perioperative period. The ventilation was altered to ensure that the end-tidal carbon dioxide value remained within 35 and 40 mm Hg. The pressure inside the abdominal cavity was maintained at 14 mm Hg during the laparoscopic procedure. The target range for surgical anaesthesia is a BIS of 40–60. All groups had the same surgical technique. The drug infusion was discontinued after the pneumoperitoneum was released. Once the skin is closed, all infusion drugs were stopped, and neostigmine and glycopyrrolate were used to reverse neuromuscular blockade before extubation.
HR, systolic blood pressure (SBP), diastolic blood pressure (DBP) and mean arterial pressure (MAP) were measured preoperative, after study drug, after induction, after intubation, after pneumoperitoneum at 15 minutes intervals, post-pneumoperitoneum (PP), post-surgery and PO period after 15 minutes (primary outcome). Response to verbal commands, orientation in time and the interval between the end of anaesthesia and tracheal extubation were also measured (secondary outcome)
Any incidence of bradycardia (HR<50/min) was treated with inj. atropine 0.6 mg intravenous (IV) Any hypotension (MAP below 20% preoperative) treated with a fluid bolus of normal saline 200–300 mL. If fluid bolus did not alleviate the hypotension, an IV injection of 5 mg of mephentermine is given. Dopamine infusion was started to maintain blood pressure if hypotension did not improve after two mephentermine doses. Hypertension (MAP>20% of baseline values) was managed with anaesthetic agents and nitroglycerin infusion.
A similar study[9] previously reported that the mean HR would decrease by 30% after therapy; the sample size was determined. To achieve statistical significance (power of 80% and α = 0.05), each group needed to have 28 patients. To consider possible dropouts or breaches of the protocol, we included 32 patients in each group.
The GraphPad prism 6.0 (statistical software) was used to perform the statistical analysis. For continuous variables, one-way analysis of variance (ANOVA) and the Chi-square test for categorical variables were used to analyse the demographic data. Haemodynamic variables (HR, SBP, DBP and MAP) were compared between groups using one-way ANOVA, which was followed by an unpaired t-test. The means of haemodynamic variables were compared intragroup to baseline parameters using repeated measure ANOVA with the post-hoc Tukey test. A P value of less than 0.05 was considered statistically significant.
Results
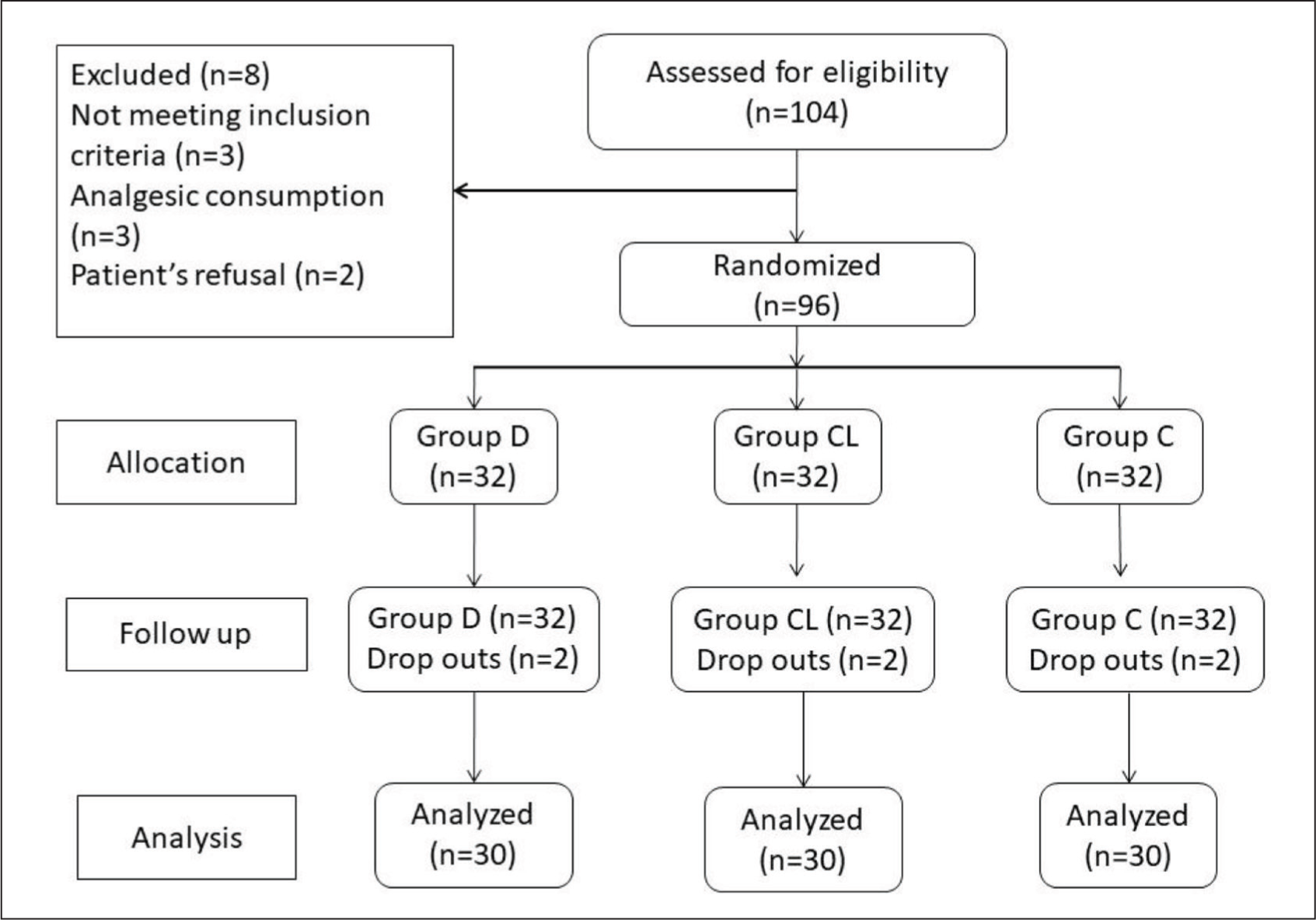
A total of 104 patients were assessed for eligibility, out of which 96 patients were included in the study after randomisation and 90 patients (93.75%) completed the study (Figure 1). One hundred four patients in total had their eligibility evaluated; 96 of those patients were randomised into the study, and 90 patients (93.75%) completed the study. Eight patients were eliminated from the study because three of them did not meet the inclusion criteria, two of the patients refused to participate and three of the patients used analgesics. Six patients were excluded from this study due to blood loss (one patient in group CL), bradycardia (one patient in group D), hypotension (one patient in group D) and the need for open surgery (three patients, one patient in group CL, and two patients in group C). Although their data has been incorporated into the comparison of demographic profiles, additional statistical analysis was not conducted on them.
Study Design
Regarding the groups’ demographic characteristics, there was no significant difference (P > 0.05) (Table 1). Compared to group C, the induction dose of propofol in groups D and CL was significantly lower (P < 0.0001).
Demographic data
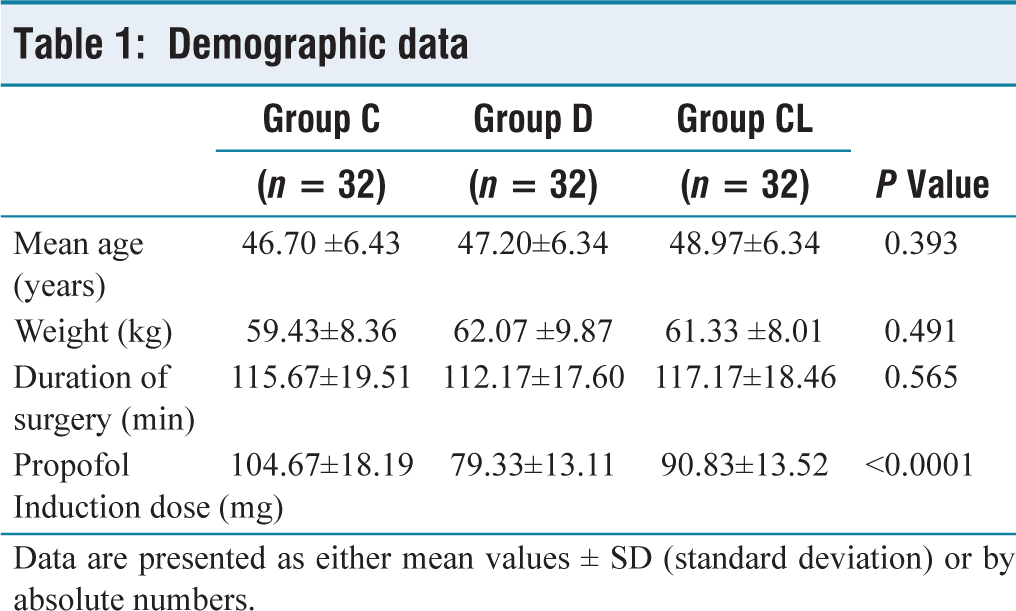
Data are presented as either mean values ± SD (standard deviation) or by absolute numbers.
The study groups did not show any significant variance in preoperative haemodynamic parameters. There was a significant decrease in HR in group D, after administration of the study drugs (P < 0.05). After intubation, there was no difference in HR values between groups D and CL (P = 0.144). Intubation and pneumoperitoneum caused an increase in the HR in the group C only (P < 0.05). There was no significant difference in HR values between group D and group CL, during post-surgery (P = 0.073) and PO period (P = 0.713) (Table 2).
Heart rate
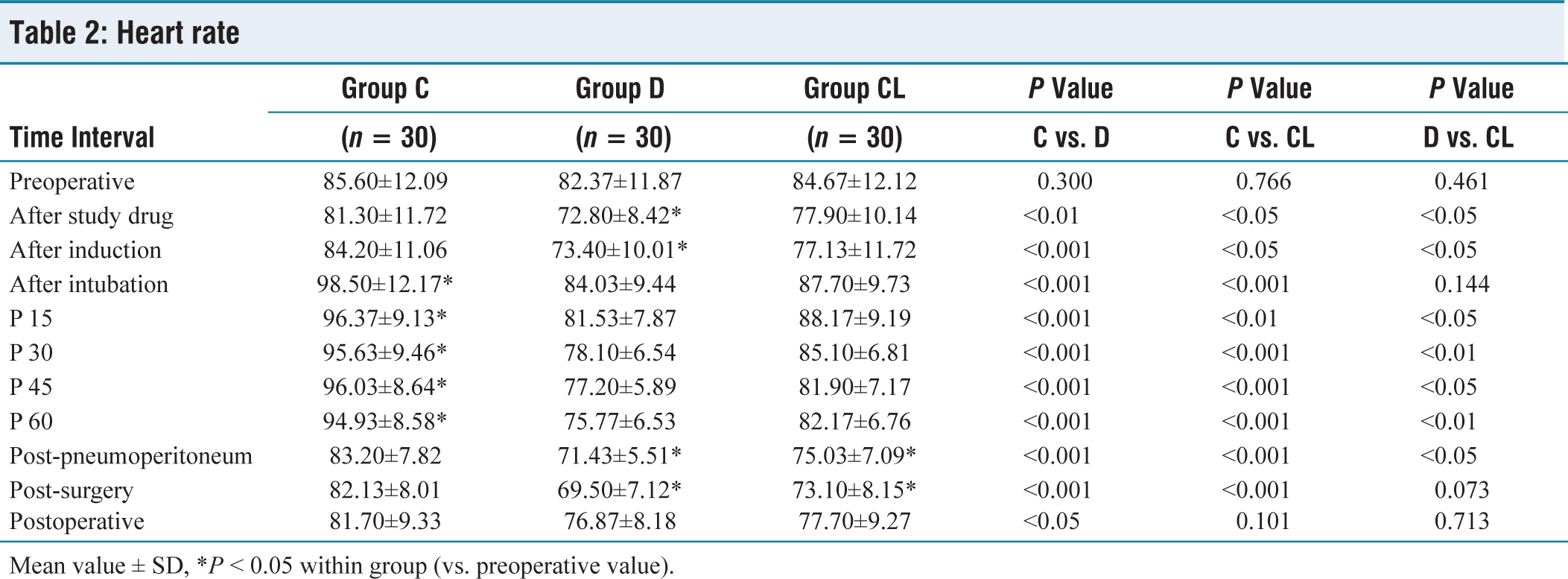
Mean value ± SD, *P < 0.05 within group (vs. preoperative value).
SBP values were statistically significantly increased in group C after intubation and 15 minutes PP period only, while DBP values were statistically significantly increased in group C after intubation and the whole pneumoperitoneum period. SBP and DBP values in group D and CL did not significantly increase over preoperative values at any point in time (Tables 3 and 4).
Systolic blood pressure
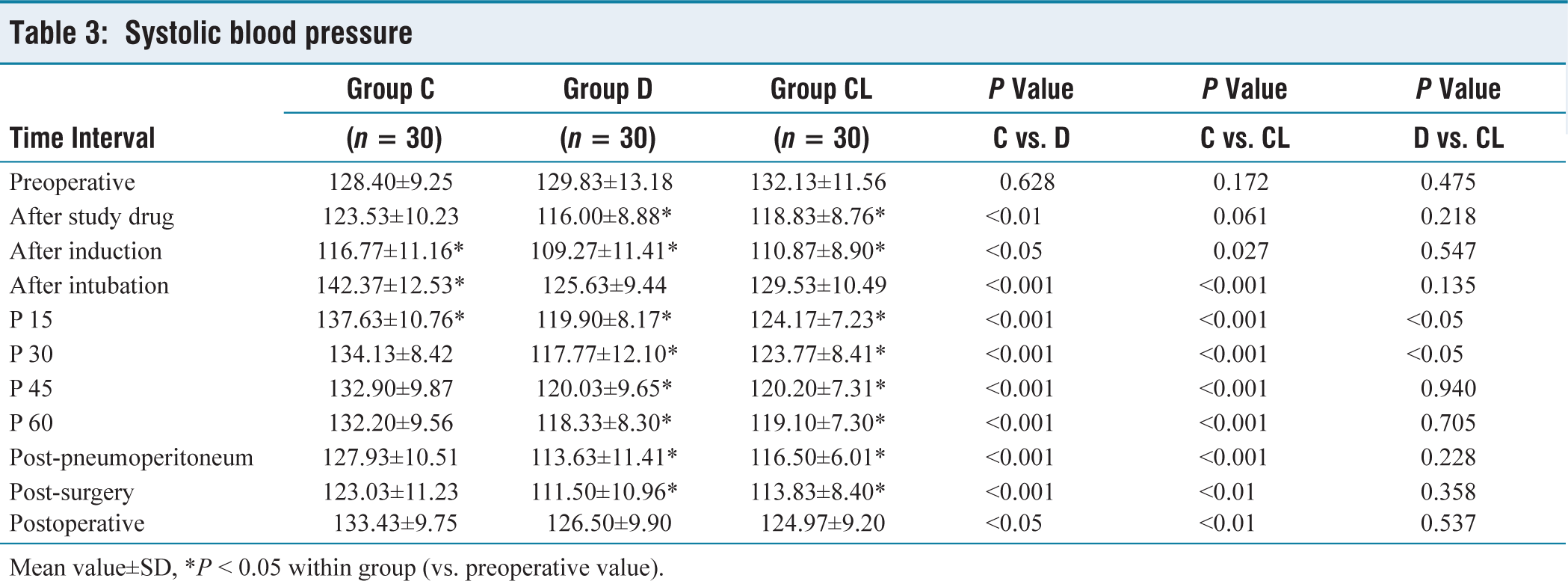
Mean value±SD, *P ˂ 0.05 within group (vs. preoperative value).
Diastolic blood pressure
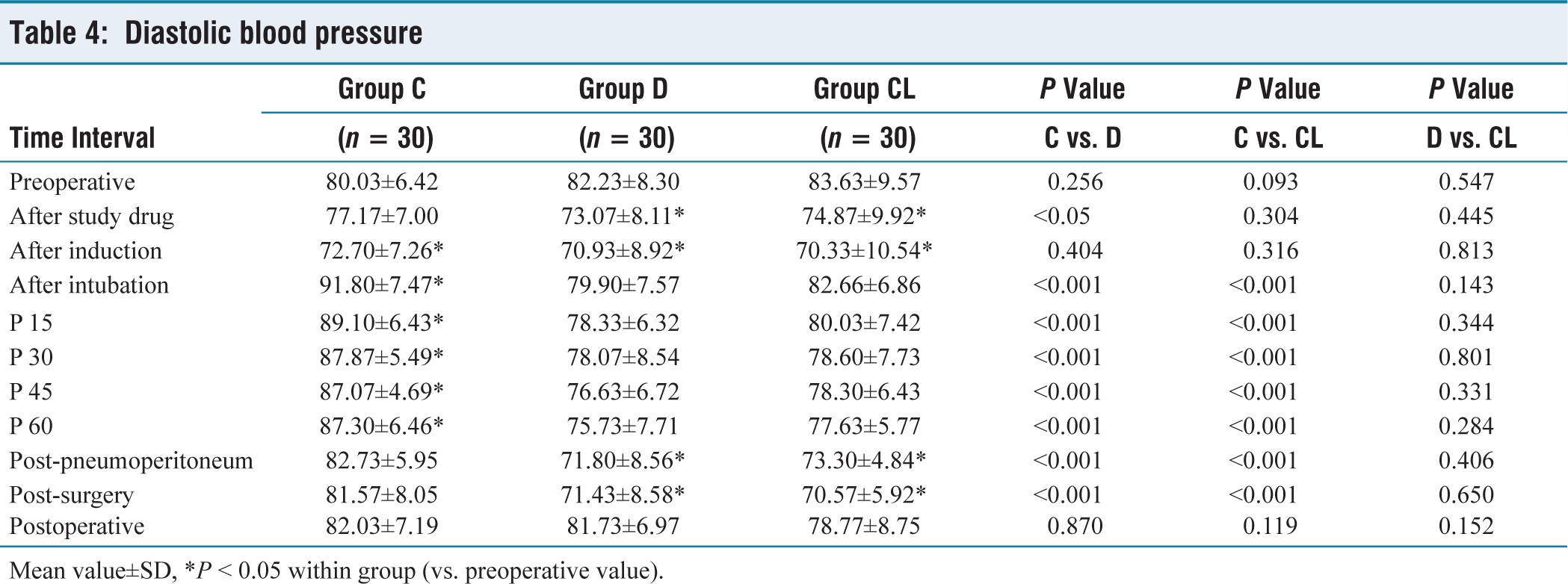
Mean value±SD, *P ˂ 0.05 within group (vs. preoperative value).
There was no significant increase in MAP in either group D or group CL during any time periods of pneumoperitoneum, in contrast to the significant increase observed in group C following intubation and throughout the pneumoperitoneum period (P ˂ 0.05), except for 60th minute of pneumoperitoneum compared to preoperative values (P ˂ 0.05) (Table 5) There was no significant difference in blood pressure values between group D and group CL during whole study period (Tables 3–5).
Mean arterial pressure
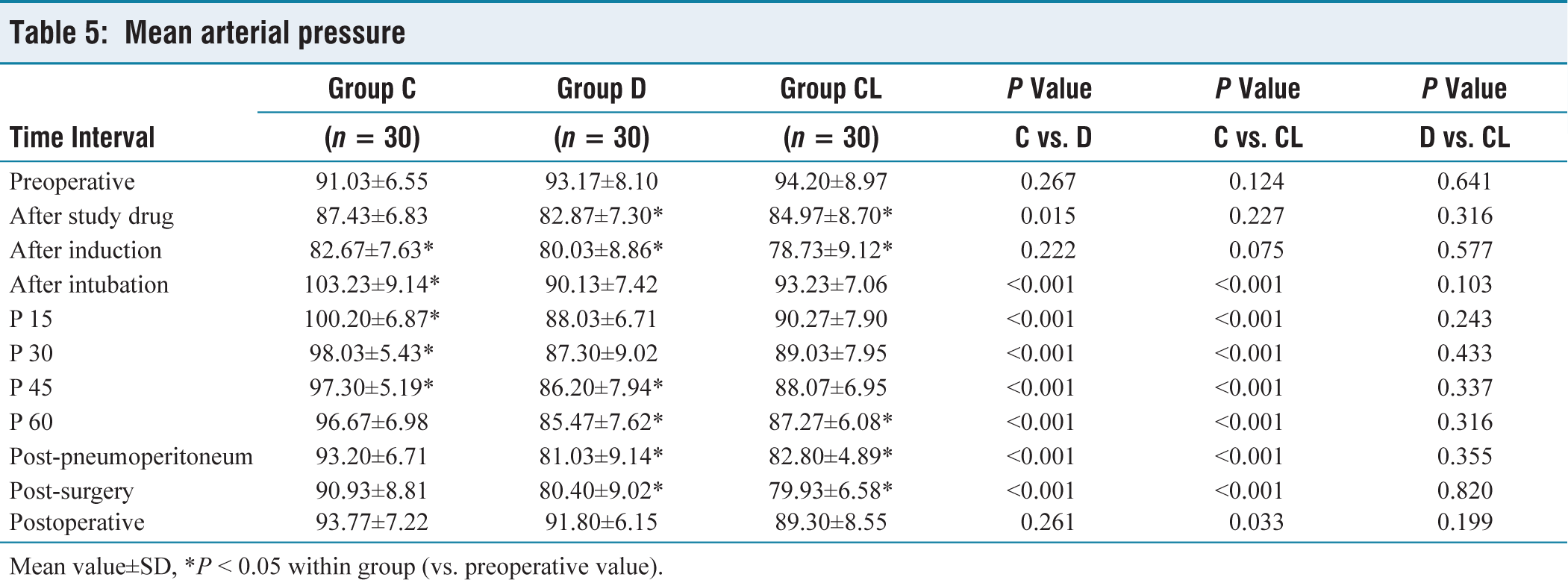
Mean value±SD, *P ˂ 0.05 within group (vs. preoperative value).
Recovery parameter
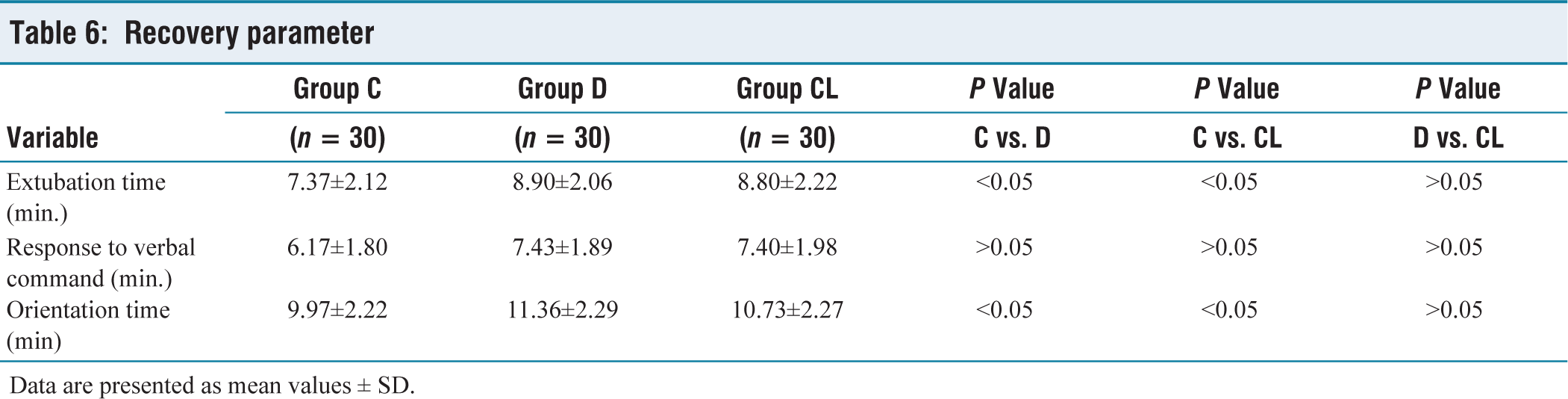
Data are presented as mean values ± SD.
Extubation time and orientation time were significantly delayed in group D and group CL when compared with group C (P ˂ 0.05). However, there was no significant difference in response to verbal command among the all-study groups (P ˂ 0.05) (Table 3).
One patient in group D had hypotension, which improved after receiving mephentermine 5 mg IV Bradycardia was also observed in one patient in group D which is resolved by the use of atropine 0.6 mg IV. No other adverse effects were noted in any of the group.
Discussion
Our study confirms that dexmedetomidine and clonidine maintain haemodynamic stability of patients undergoing laparoscopic hysterectomy and avoid fluctuations in haemodynamic parameters due to cardiovascular stress responses of pneumoperitoneum.
Laparoscopic hysterectomy has gained a lot of popularity in recent years because of the faster PO recovery, low rates of early and late PO complications, early mobilisation and discharge. Laparoscopic surgery poses various difficulties for the anaesthesiologist. Requirement of pneumoperitoneum during laparoscopic surgery and Trendelenburg position have significant effects on the haemodynamics. Pneumoperitoneum has consistently been shown to increase MAP, systemic and pulmonary vascular resistance and HR.[10] In addition, the Trendelenburg positioning used in hysterectomy to improve the surgical field view certainly is likely to increase MAP.
Dexmedetomidine is a more potent, α2-adrenergic agonist that is highly selective, specific and has a shorter half-life compared to clonidine.[6] Dexmedetomidine was studied in attenuation of haemodynamic changes during various laparoscopic surgeries. Dexmedetomidine was widely used intravenously at a recommended bolus dose of 1 µg/kg followed by a continuous infusion ranging from 0.2 to 0.7 µg/kg throughout the surgery.[9,11] Studies comparing the dosage equivalency of clonidine and dexmedetomidine are few and far between. As a result, the dose of clonidine was chosen based on earlier research that had determined its most efficient dosage for intraoperative use.[12,13] Because rapid administration of these drugs can cause bradycardia and hypotension, so the bolus dosage was given during a 15-minute duration in our study as confirmed by various authors.[9,12,14]
Clonidine and dexmedetomidine inhibited norepinephrine release by presynaptic activation of the α2 adrenoceptor thereby disrupting the propagation of pain signals. Postsynaptic activation of α2 adrenoceptors in the central nervous system suppresses sympathetic activity, which can decrease blood pressure and HR.[6]
In our study, dexmedetomidine and clonidine provide intraoperative haemodynamic stability, which has been demonstrated by various authors in previous studies.[9,12,14] Similar to our results, Ashwini et al. also confirm the haemodynamic stability in laparoscopic hysterectomy surgery by the use of dexmedetomidine.[9] A meta-analysis and systematic review done by Li et al. also conclude the same results as in our study.[14] Choi et al. also used the same dose of dexmedetomidine and haemodynamic changes which is similar with our study.[15]
Dexmedetomidine and clonidine potentiate anaesthetic effects of all intraoperative anaesthetics.[16] It was demonstrated that central α2 adrenergic receptors mediated the significant reduction in anaesthetic requirement.[6] We also observed that dexmedetomidine and clonidine significantly reduce induction dose of propofol (24 and 14%).
In this study, patients received dexmedetomidine and clonidine which were associated with significantly longer recovery time (extubation time and orientation time) compared to control group; this effect was also observed in previous studies.[17] But Bellaïche et al. have noticed no significant delay with the use of clonidine premedication.[18] Such discrepancy in results among studies might arise due to different route and dose of clonidine. There was no significant difference in response to verbal command time, this is because of dexmedetomidine- and clonidine-induced natural sleep pattern.
Altan et al. and Ray et al.[19,20] used clonidine 3 μg/kg IV over a period of 15 minutes before induction and 2 μg/kg/hour by continuous infusion intraoperatively and observed significant incidence of bradycardia and hypotension. We used clonidine 2 μg/kg IV over 15 minutes before induction and continuous infusion to 1 μg/kg/hour during intraoperative period and noticed no significant episode of hypotension and bradycardia.
There were some limitations of the study. Firstly, the results may not be generalisable to the entire population due to the small sample size and relatively homogeneous patient ages. Secondly, the pharmacokinetics were not assessed because concentrations of the drugs in plasma was not measured. Thirdly, a manually controlled infusion of propofol was administered rather than the suggested target-controlled infusion.
Conclusion
We highlight the use of dexmedetomidine and clonidine in laparoscopic hysterectomy to maintain haemodynamic response to pneumoperitoneum. Furthermore, the requirement of induction dose of propofol and intraoperative fentanyl requirement are decreased by dexmedetomidine and clonidine. However, dexmedetomidine and clonidine cause delayed extubation and orientation time.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
AHB/CR/123/10-07-2018.
Informed consent
Informed consent was obtained from all patients.
Credit author statement
All authors contributed to the study conception and design.
VKS: Data analysis, Manuscript prepartation, Manuscript editing and review.
YRK: Literature search, Data acquisition, Manuscript preperation.
SK: Literature search, Manuscript preparation, Manuscript review.
DSA: Data acquisition, Manuscript preparation and editing.
VSH: Literatute search, Manuscript review.
DG: Literature search, Data acquisition, Manuscript editing.
Data availability
Data should be available as required.
Use of artificial intelligence
None.