
Abstract
Background:
Splenic cysts are uncommon ailments and are incidentally discovered either during imaging procedures or while examining the cause of left upper abdominal pain. The origin of splenic cysts can be either parasitic or non-parasitic. Non-parasitic cysts can be classified as primary or secondary. Primary cysts are also referred to as true, congenital, epidermoid or epithelial cysts. On the other hand, secondary cysts are commonly known as pseudocysts. Splenic cysts are usually asymptomatic and can be found incidentally. Symptoms are usually related to the size of the cyst. Patient may present as local or referred pain, abdominal fullness, local tenderness or symptoms due to compression of the adjacent organs.
Case report:
We present a case report involving a 56-year-old male patient who was diagnosed with a sizable splenic cyst, initially suspected to be a hydatid cyst. The patient underwent splenectomy, and subsequent microscopic evaluation revealed a diagnosis of a mesothelial cyst, a condition that is considered rare.
Conclusion:
The clinical history, radiological findings and pathological examination of the cyst are discussed to highlight the diagnostic challenges and management considerations associated with this unusually large mesothelial splenic cyst in adults.
Introduction
Non-parasitic splenic cysts are infrequent and are often incidentally detected during imaging studies or diagnostic evaluations for left upper abdominal pain. Mesothelial cysts arise from the mesothelial cell lining of the splenic capsule.[1] These rare cysts typically do not show any symptoms for an extended period, yet they possess the capability to induce various symptoms and complications, thereby necessitating additional investigation.[2]
Of all of these splenic cysts, primary splenic cyst constitutes 10% of all non-neoplastic cysts of spleen. These cysts are predominantly seen in paediatric and adolescent age groups.[3,4]
Among the other types of splenic cysts, hydatid cysts caused by Echinococcus granulosus are the most common type of splenic cyst worldwide.
Most cases are asymptomatic, however, as the cyst enlarges patient generally presents complaining of abdominal symptoms.
The primary imaging modality for diagnosis consists of abdominal ultrasonography and computed tomography (CT), with the most accurate method being CT.
Splenectomy is the typical treatment for splenic cysts; however, recent studies over the past few decades show that conservative treatment for splenic cysts has reduced short- and long-term complications.
We report a case of a 56-year-old male with a large splenic cyst with a significant mass effect on left kidney as well as on the pancreas causing its medial displacement and compression.
Case presentation
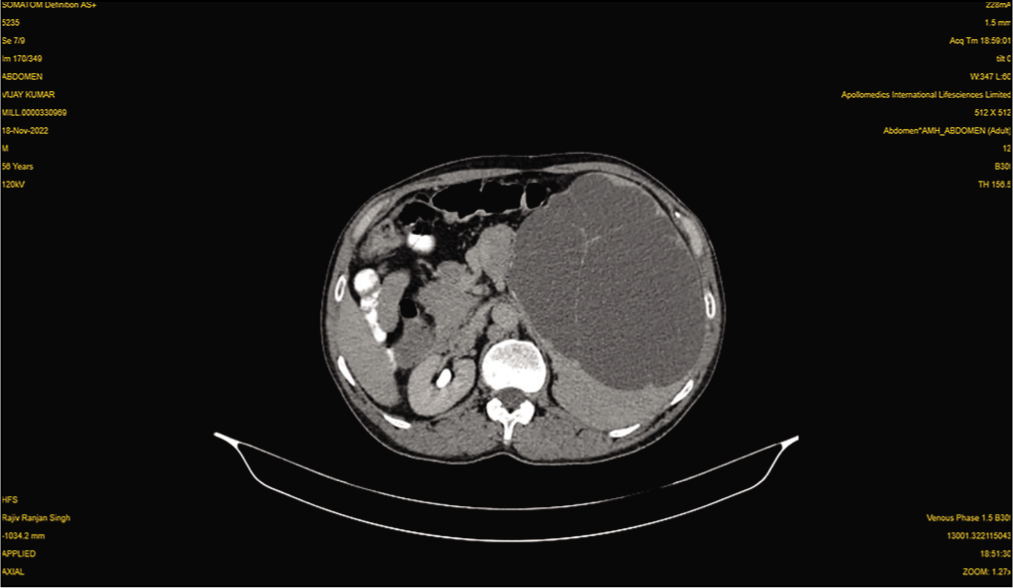
A 56-year-old male presented with a four-month history of abdominal distension. The abdominal examination revealed mild tenderness in left hypochondriac region and splenomegaly. There was no history of trauma, significant medical illness, or surgical intervention in past. CT revealed enlargement of spleen due to irregularly marginated heterogeneous non-enhancing lesion showing thick septations causing significant mass effect on left kidney as well as pancreas causing its medial displacement and compression; based on these findings, clinical suspension of hydatid cyst was raised [Figure 1].
CT scan: shows spleen with irregularly marginated heterogeneous non-enhancing lesion showing thick septations
Due to the suspicion of a hydatid cyst, the patient underwent an elective open splenectomy.
On gross examination, specimen of spleen weighed 3.0 kg and measured 22×19×13 cm. Outer surface was globular, fluctuant and smooth. On cut almost the whole of the spleen was replaced by a multilocular cyst measuring 20×16×9.0 cm, showing multiple small septations. The cyst wall was pearly white at places and thinned out measuring 0.1-0.2 cm in thickness. Normal appearing spleen was identified at periphery.
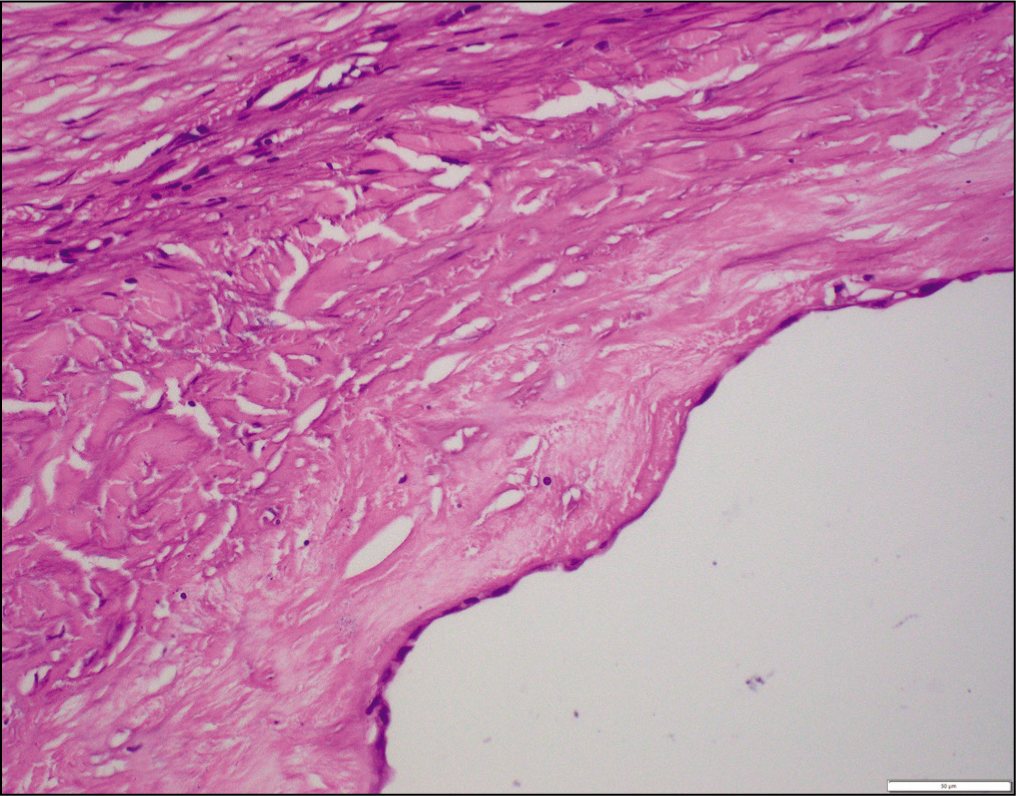
Histopathological examination of the surgical specimen confirmed a splenic cyst composed of thick collagen tissue and lined by a single layer of mesothelial cells [Figure 2]. Sections of spleen close to cyst showed markedly prominent red pulp and atretic white pulp. No protoscoleces, laminated membranes or hooklets typically seen in hydatid cysts were identified. Additionally, no evidence of active inflammation, infection or malignancy was observed.
200×: Hematoxylin and Eosin: Splenic cyst wall lined by attenuated single layered mesothelial lining
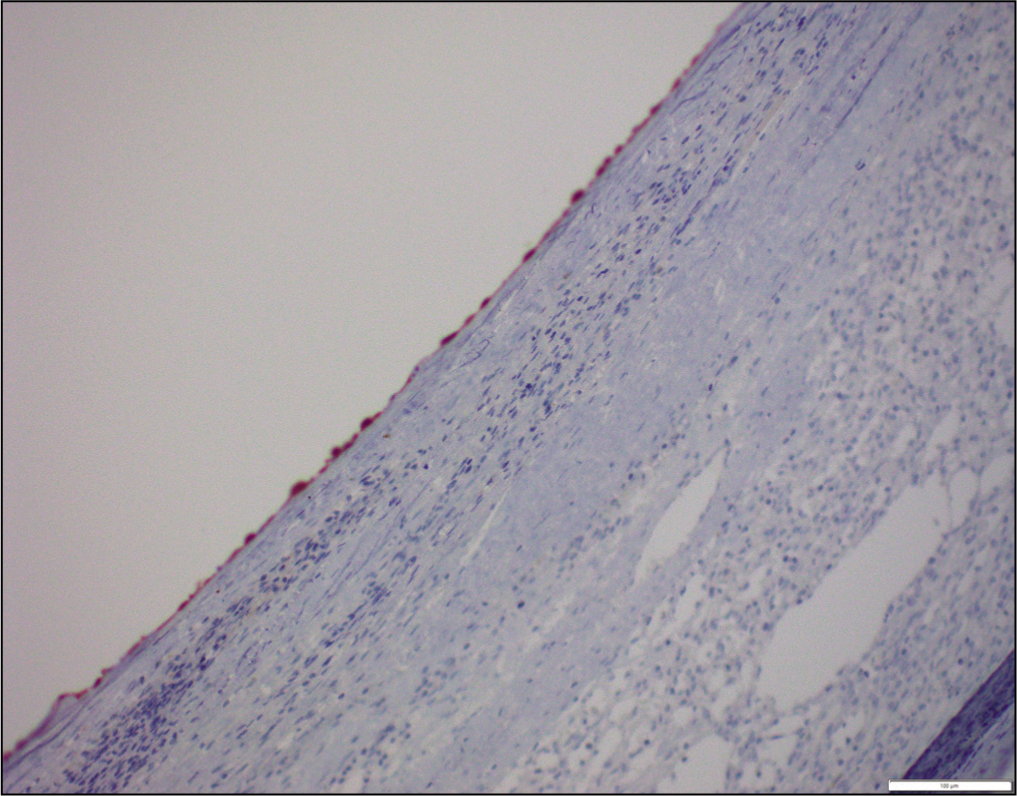
Immunohistochemically, the splenic cyst lining cells were positive for pan-cytokeratin, and calretinin [Figure 3] and negative for CD34 (an endothelial marker) and D2-40 (a lymphatic epithelial marker).
200×: Immunohistochemistry: Calretinin highlights the mesothelial lining of the cyst wall
Thus, a final diagnosis of a large mesothelial splenic cyst was rendered.
Discussion
Splenic cysts pose a diagnostic dilemma because of their wide range of causes and unpredictable clinical manifestations. According to the available literature, the classification of these abnormalities has undergone significant changes since Andral’s initial report in 1929, resulting in the current classification system.[5]
Splenic cysts are categorised based on various factors such as the presence or absence of lining, aetiology and pathogenesis. Martin distinguished splenic cysts into two types: type 1, which are true cysts with an epithelial lining, and type 2, which are false cysts without an epithelial lining.[6,7]
Splenic cysts can be broadly categorised as either parasitic or non-parasitic. Non-parasitic cysts are then divided into primary (epithelial, true) or secondary (pseudo or false) cysts.[8]
True or primary cysts are typically congenital or neoplastic in nature and are characterised by a lining of mesothelial, squamous or transitional epithelium. Secondary cysts, on the other hand, are generally caused by trauma, failed organisation of subcapsular or parenchymal haematomas, necrosis following an infarction, or in rare cases, abscesses, infections, infarctions or trauma.[9]
There are several theories proposed to explain the origin of these congenital cysts, including the development of capsular surface mesothelial invaginations leading to cyst formation. Another theory suggests that embryonic inclusion of epithelial cells from the neighbouring structure or epithelial cell metaplasia might contribute to their formation. Additionally, it is hypothesised that these cysts could arise from vascular endothelium in peritoneal inclusions.[8,9]
It is uncommon to make an accurate preoperative diagnosis of mesothelial cyst, but the presence of a unilocular cyst without a history of trauma, infection or exposure to hydatid disease can raise suspicion for this condition.[10]
New research has shown an increase in tumour markers CA19-9 and carcinoembryonic antigen (CEA) levels in relation to primary mesothelial cysts. Following the removal of the cysts, there has been a significant decrease in serum levels of CA 19-9, presenting a potential screening method for detecting recurrences following splenic preserving surgeries.[11]
Conclusion
This case report highlights the diagnostic challenges associated with large splenic cysts and emphasises the need for a comprehensive diagnostic approach. Although the clinical suspicion of a hydatid cyst was raised based on radiological findings, the pathological examination excluded it, confirming a diagnosis of a large mesothelial splenic cyst. Awareness of the various types of splenic cysts and their distinct clinic-pathological characteristics is crucial for appropriate diagnosis and management. Further research is warranted to better understand the pathogenesis and optimal management strategies for splenic cysts.
Footnotes
Declaration of conflicting interest
The authors declare no conflict of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Clearance from the ethics department was taken, before publishing, with reference number: AMH: cs-22/01a/23.
Institutional ethical committee approval number
Approval Number DG/56/2023.
Informed consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Patient consent
Consent form was taken and duly signed by participant of the case reported.
Credit author statement
Kavita Somani contributed to case diagnosis and writing of the manuscript.
Pretty Singh helped in drafting and critical appraisal.
Sujatha Poduval contributed to reporting.
Data availability
The data that support the findings of this study are available on request from the department of pathology, hospital information system and medical records department, on request. The data are not publicly available as containing information can compromise the privacy of research participants.
Use of artificial intelligence
Artificial intelligence was not used for this study.