
Abstract
Background and Aims:
Quality of life (QOL) of boys with haemophilia was severely affected due to many reasons like frequent hospital visits and joint stiffness. This study aims to analyse the impact of the prophylaxis programme on the QOL of haemophiliac boys.
Methods:
This is a twin-centre cross-sectional study that included all boys with haemophilia aged between 4 and 18 years and receiving prophylaxis. The Canadian Haemophilia Outcome – Kids Life Assessment Tool (CHO-KLAT) Version 3 was used to compare pre-prophylaxis scores with post-prophylaxis scores obtained after four months of prophylaxis.
Results:
The mean (standard deviation [SD]) age of the study participants was 10.66 (1.28) years. About 88% had haemophilia A and 66.66% had good adherence to prophylaxis. The mean pre-prophylaxis total score was 45.6 (4.9) and the mean post-prophylaxis total score was 64.3 (5.4). Significant improvement in total scores and domain scores was observed in the post-prophylaxis group.
Introduction
Haemophilia A and B are familial bleeding disorders that are caused by the deficiency of clotting factors, factor VIII and IX, respectively. They are inherited as X-linked recessive diseases and affect the boys predominantly, while the girls are asymptomatic carriers.[1] The disease manifests with spontaneous bleeds, post-traumatic bleeds, mucosal bleeds and sometimes fatal intracranial bleeds also.[2] Recurrent bleeds are associated with severe joint damage and long-term disabilities. Based on the factor levels, haemophilia is classified as mild (5%-40%), moderate (1%-5%) and severe (<1%).[3]
The quality of life (QOL) of boys with haemophilia (BWH) was severely affected due to many reasons including frequent hospital visits, joint stiffness and limitations of day-to-day physical activity.[2] Until the middle of the twentieth century, the only treatment options available were whole blood or fresh plasma transfusion which were not efficient treatment options and were not effective in preventing the bleeding episodes.[4] The idea of infusing factor VIII prophylactically into BWH started in the year 1958, with researchers from Sweden infusing factor VIII concentrate into them and converting them from severe-to-moderate phenotype reducing their bleeding rates and improving joint health.[5] Much emphasis was given to the prophylaxis and treatment regimens that improve the QOL and preserve joint functions in these boys in the past few decades.[6] Primary prophylaxis has now become the evidence-based standard of care for BWH.
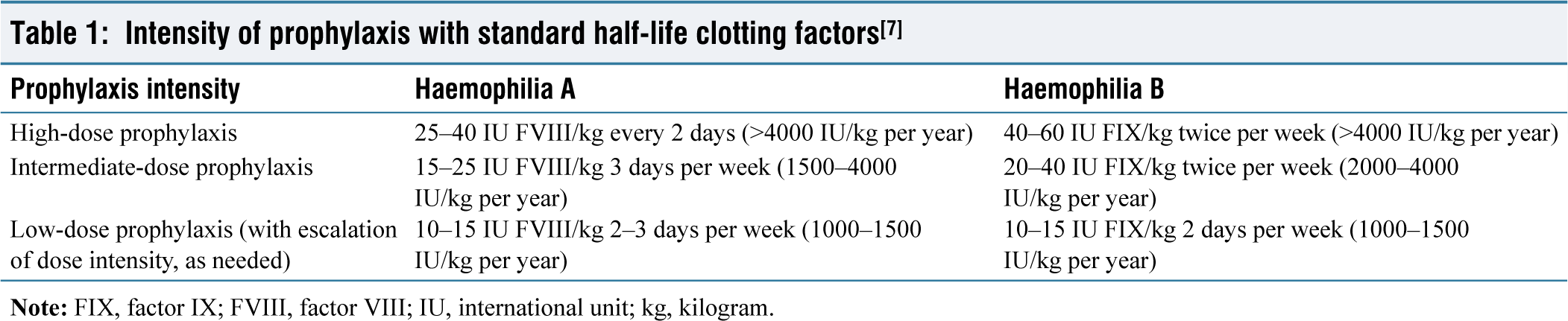
The prophylaxis programmes are classified based on the intensity of prophylaxis and are summarised in Table 1.[7] The regular infusion of clotting factor concentrates (CFCs), even at lower doses, under the prophylaxis programmes has been associated with improvements in joint functions, reduction in bleeding rates and improvement in QOL.[7-10] The main objective of the prophylaxis programme is to prevent bleeding and joint damage and maintain normal musculoskeletal function.[9,10] The challenges in the implementation of these programmes are the huge costs involved and adherence to therapy by the BWH. A conservative estimate of annual expenditures incurred for a boy weighing 20 kg with haemophilia A and haemophilia B is ₹12.06 lakhs (USD 14365.90) and ₹19.6 lakhs (USD 23347.56) respectively (as of 12 August 2024, on the maximum retail price of factor VIII and factor IX CFCs).
Intensity of prophylaxis with standard half-life clotting factors[7]
Understanding the importance of the prophylaxis programmes, the National Health Mission, Tamil Nadu, has rolled out the Haemophilia Prophylaxis Programme in five integrated centres for haemophilia and haemoglobinopathies (ICHH) in the state in the year 2023.[11] In these centres, BWH A and B were enumerated and tested for inhibitors. The inhibitor-negative boys were enrolled in a low-dose prophylaxis programme and were offered CFCs free of cost. Apart from prophylaxis, these boys were also given comprehensive care including treatment for breakthrough bleeds, physiotherapy and health education.
Aims and objectives
This study aims to analyse the impact of the prophylaxis programme on the QOL of BWH by comparing the Canadian Haemophilia Outcome – Kids Life Assessment Tool (CHO-KLAT) scores obtained before and after starting the prophylaxis.
Methods
This is a twin-centre cross-sectional study done in two of the ICHHs in March and April’2024. A convenient sampling of all the willing BWHs in the two selected ICHHs was done. Institutional Human Ethics Committee approval was obtained from both centres. Written consent was obtained from the parents.
Inclusion criteria
All BWH, aged between 4 and 18 years, and receiving prophylaxis in the two selected ICHH centres were included in the study.
Exclusion criteria
The following are the exclusion criteria:
The BWH who were not willing for the study, Boys with other bleeding disorders, and BWH who were not receiving prophylaxis were excluded.
The data extracted from the records from BWH included socio-demographic and clinical details like name, age, diagnosis, severity of the disease, level of prophylaxis, annual bleeding rate (ABR) and haemophilia joint health score (HJHS). The adherence to the prophylaxis was taken as good, intermediate and poor, if the BWH has not missed any dose, missed one to four doses and missed five or more doses in a month, respectively.
Study tool
The tool used in this study for analysing QOL in BWH was the CHO-KLAT Version 3.[12] For BWH aged between four and six years, CHO-KLAT parent-proxy version was used and for BWH aged above seven years, CHO-KLAT child self-reported version was used alongside parent-proxy report version. The CHO-KLAT is a cross-culturally validated tool that was extensively used by researchers in India and around the world for assessing the QOL in BWH.[2,13] This tool consists of 41 questions in seven domains – activity, autonomy, bleeding, emotional health, haemophilia knowledge, social functioning and treatment. In the study hospitals, the prophylaxis programme was started in October 2023 and is progressing successfully. The parents were asked to respond to the questions about the QOL of their BWH, with the CHO-KLAT scoring sheet. For analysing the pre-prophylaxis scores, the parents were asked to respond to it considering a four-week period immediately preceding the start of the prophylaxis. For analysing the post-prophylaxis scores, the parents were asked to respond to it considering a four-week period, four months after the start of the prophylaxis programme. The same parent did both pre-prophylaxis and post-prophylaxis scorings but on different sittings. Before administering, the questionnaire debriefing for the parents was done. The results were tabulated and analysed.
Statistical analysis
Data was analysed using R software version 4.1.1. All categorical data were presented using frequency and percentage and all continuous measurements were presented as mean (standard deviation [SD]) or median (interquartile range [IQR]) after assessing the normality assumption using Shapiro-Wilk test. The change in CHO-KLAT total score and domain score from pre-prophylaxis to post-prophylaxis was assessed using a paired sample t-test. The post-prophylaxis CHO-KLAT scores, breakthrough bleeds and distance from ICHH were compared between different levels of adherence using a one-way analysis of variance (ANOVA) test or the Kruskal-Wallis test based on the distribution. P value was considered significant at a 5% level of significance.
Results
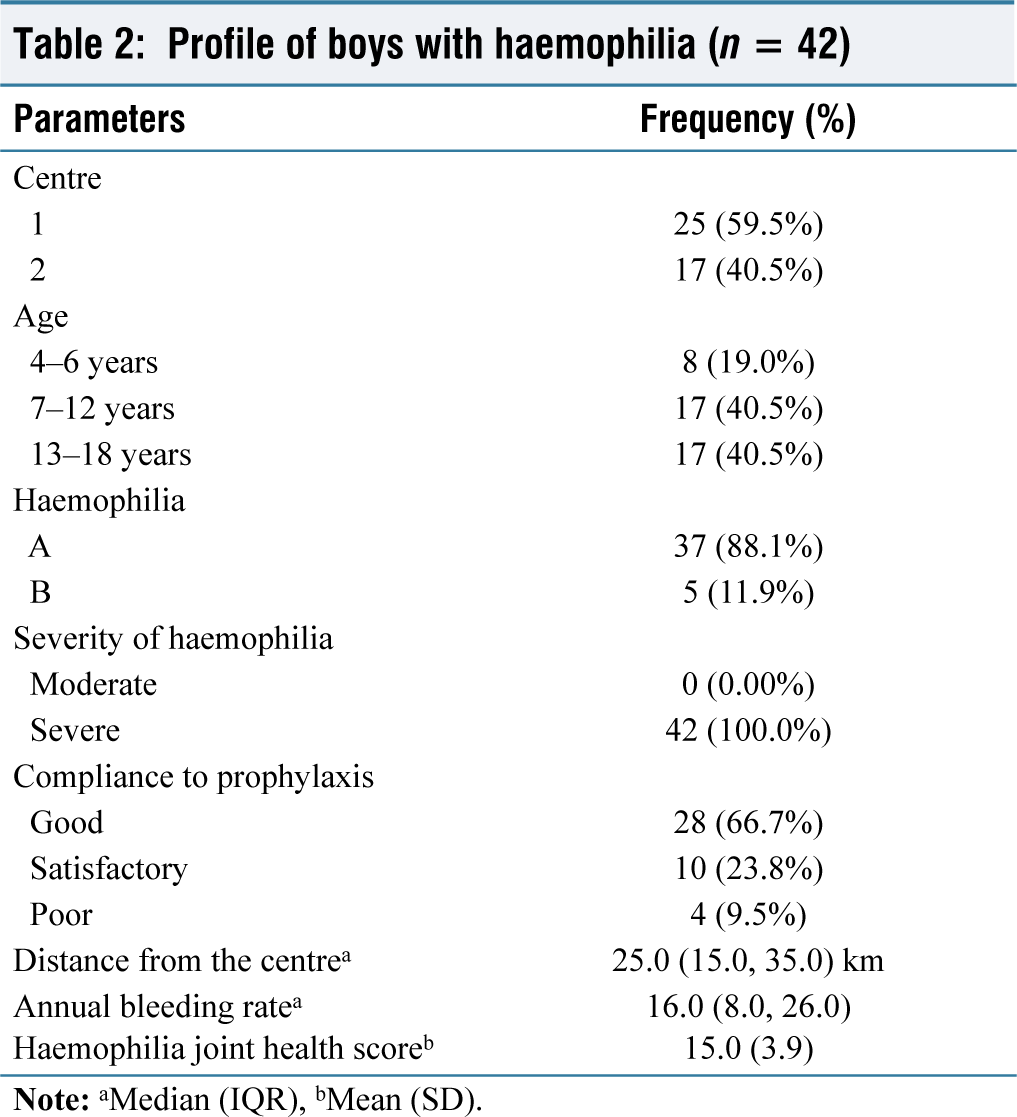
The results are shown in Tables 2 and 3. After excluding 6 BWH who were on-demand treatment, there were about 42 BWH (25 from the first centre and 17 from the second centre) who formed the study group. The mean (SD) age of the study participants was 10.66 (1.28) years. Haemophilia A was observed in 88% of the study participants and haemophilia B in 12%. All of the study participants had severe haemophilia. Good adherence to prophylaxis was seen in 66.66% and poor adherence to prophylaxis was seen in 9.53%. The median distance from the residence of the BWH to the ICHH was 25.0 (15.0, 35.0) km. The median ABR was 16.0 (8.0, 26.0). The mean HJHS was 15.0 (3.9).
Profile of boys with haemophilia (n = 42)
Distribution of CHO-KLAT scores
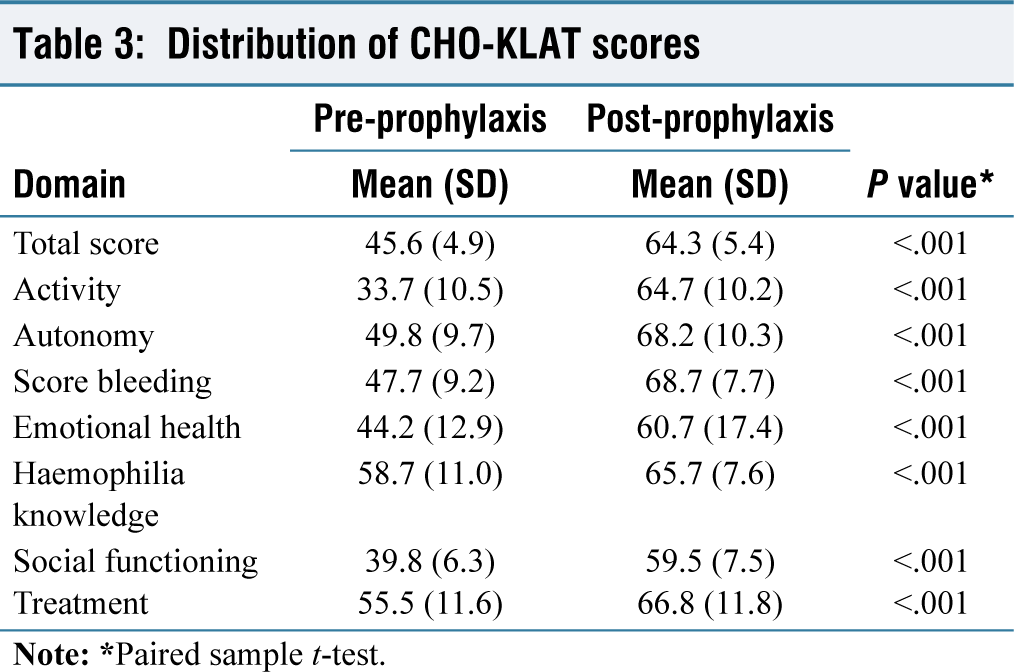
The mean CHO-KLAT scores before and after prophylaxis are tabulated in Table 3. The mean pre-prophylaxis total score was 45.6 (4.9) and the mean post-prophylaxis total score was 64.3 (5.4). The mean pre-prophylaxis and post-prophylaxis scores in the seven domains of activity, autonomy, bleeding, emotional health, haemophilia knowledge, social functioning and treatment are also shown in Table 3. Significant improvements were observed in the mean total scores and in all the seven domain scores in the post-prophylaxis group (P <.001). The largest improvement in scores after prophylaxis was seen in the activity domain and the smallest improvement was seen in the knowledge domain.
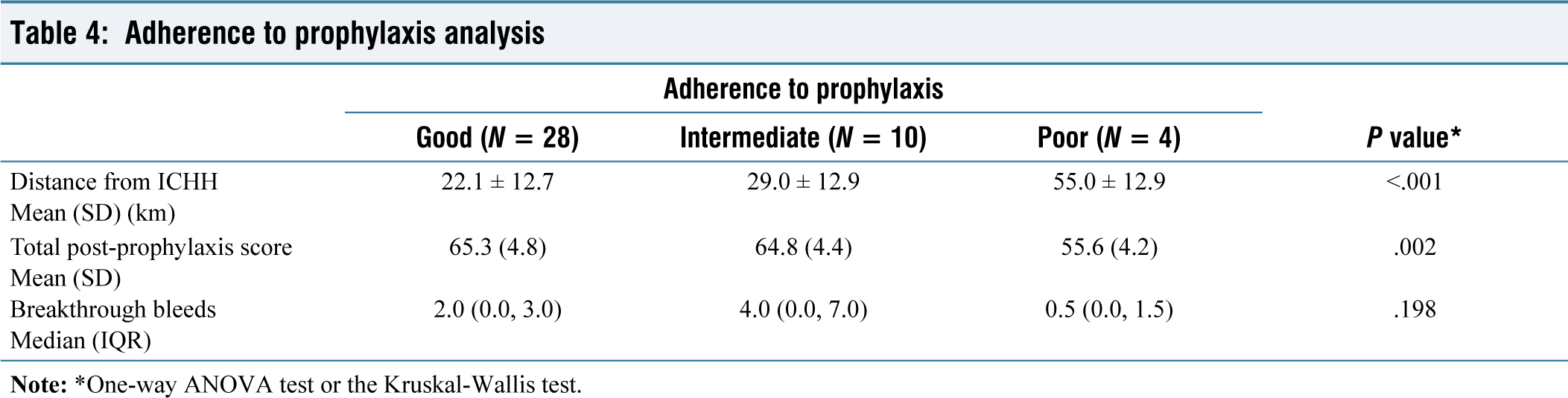
On analysis of the correlation between adherence to the prophylaxis and the post-prophylaxis scores, significantly lower total scores were observed in the poor adherence group (P <.001) [Table 4]. No significant difference in the number of breakthrough bleeds was observed between the adherence groups (P = .143). The four boys who had poor adherence to prophylaxis were residing at a longer distance from ICHH (P <.001). The mean distance from their home to the ICHH was significantly longer (mean distance: 55.0 km [SD: 12.9]) and reported longer distance as the barrier to adherence.
Adherence to prophylaxis analysis
Discussion
Prophylaxis programmes have become the standard of care for BWH in developed countries. However, due to resource limitations, prophylaxis has not yet become the standard of care for BWH in developing countries. As prophylaxis is the standard of care, there are not much of studies available to compare the QOL reported in the pre-prophylaxis group in this study. However, a few studies have reported QOL in BWH who were on-demand treatment and were taken for comparison.[14] Also, only a few studies have reported QOL of BWH in India.[15] In this study, we have described the pre-prophylaxis QOL and the short-term changes in QOL after the implementation of the prophylaxis programme.
The mean pre-prophylaxis CHO-KLAT score in this study is 45.6 (4.9). A pooled study of nine studies done by Usuba et al. reported a pooled mean score of 71.7 (13.1) for BWH who were on-demand treatment.[14] In a study by Zhang et al., the mean score of the on-demand group was 52.64 (19.26).[2] The mean post-prophylaxis score observed in this study is 64.3 (5.4). Many studies are available that have reported the mean post-prophylaxis scores ranging from 57.1 (12.6) to 82.5 (8.6).[16,17] There has been considerable heterogeneity in the scores that are influenced by sociocultural and other factors.
There has been significant improvement in the post-prophylaxis scores in all seven domains in this study with the largest improvement in activity and the smallest improvement in knowledge domains. In a study by Price et al., better scores were observed in knowledge and treatment domains.[12] The authors in their study have also compared the scores among the BWH receiving standard half-life and extended half-life CFCs and reported better scores in those receiving extended half-life CFCs. The extended half-life bio-engineered factors hold a promising future in the prophylaxis programmes for BWH.
In this study, adherence to the programme was poor in four BWH. All four were residing at a longer distance from the centre. The adherence to therapy directly impacts the QOL in BWH. In some countries, home injections are prescribed to improve adherence to the programme.[18] The feasibility of home infusions in developing countries is not yet studied.
The QOL of BWH is poised to improve in the future with the prophylaxis programme and the use of newer treatment options like extended half-life CFCs, gene therapy and immunomodulators. The governments have now committed to expanding the prophylaxis programme universally to all BWH and India can witness a giant leap in the QOL of BWH in the coming years.
Limitations of the study
Only a short-term change in QOL was analysed in this study and no long-term changes were analysed.
The changes in ABRs and HJHS were not studied, as the study was done in a short term of four months after the implementation of the prophylaxis programme.
The parents might have exercised some recall bias during CHO-KLAT scorings.
Conclusion
This study has demonstrated a significant improvement in the QOL of BWH in the short term of four months after the implementation of the prophylaxis. The prophylaxis programme is a giant leap in the QOL for these boys. BWH residing at a longer distance from the centre had poor adherence to prophylaxis and their QOL was also significantly lower. A universal prophylaxis programme for all BWH is recommended for the improvement of their QOL.
Footnotes
Acknowledgements
The authors would like to thank all the participants and the nurses working in both centres.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Institutional Ethical Committee Approval Number
Ethical approval was obtained from the following institutions:
Govt Mohan Kumaramangalam Medical College, Salem Ref No.710/ ME-G/2024–96 dated 01.03.2024. Govt. Dharmapuri Medical College, Dharmapuri Ref No. 2/2024 dated 31.01.2024.
Informed consent
A written consent was obtained from the parents.
Credit author statement
M. Danishraja, K. Sujitha, S. Shylaja and C. Rathinavel were involved in the acquisition, analysis and interpretation of data.
V. Anurekha, B. Rameshbabu, K.S. Kumaravel and D. Sampathkumar drafted the article and revised it critically for important intellectual content.
All the authors have participated sufficiently in the work and take public responsibility for appropriate portions of the content.
All the authors read and approved the final version before submission.
Data availability
The data that support the findings of this study are available on request from the corresponding author.
Use of artificial intelligence
Not used in this study.