
Abstract
Background and Aims:
Pelvic bone tumours are rare, with a guarded prognosis despite advances in radiological imaging and surgical techniques. Despite this, limb salvage surgery has become the mainstay treatment for patients presenting with primary bone sarcomas, especially those with low histological grade variants. However, the rate of peri-operative-associated complications remains high in the form of local recurrence and surgical site infections (SSI).
Objective:
We highlight our experience from a tertiary referral oncology centre of incidence and clinical and radiological features, as well as discuss the risk factors for developing pelvic stress fractures (PSFs) in patients treated with hemipelvis resection.
Materials and Methods:
We performed a retrospective search from our radiology and oncology database at our tertiary orthopaedic oncology referral centre for patients referred, diagnosed and managed for stress fractures following an internal hemipelvectomy for pelvic tumours/Sarcoma through the service between 2007 and 2019. Patient demographics, clinical characteristics, complementary imaging, clinical management outcome and peri-operative complications were documented. A focussed evaluation of patients diagnosed and managed for PSFs in patients treated with hemipelvis resection.
Results:
We identified a total of six patients with stress fractures following internal hemipelvectomy. The sacrum was the most common anatomical region (n = 3). Other areas identified with insufficiency stress fractures included the ischium and femoral neck.
Background
Bone tumours of the pelvis are rare and can present as primary lesions (sarcomas), metastatic secondary tumours or invasive conditions from adjacent soft tissue neoplasms posing diagnostic and therapeutic challenges.[1] Patients with pelvic tumours may have an insidious onset of symptoms due to the intricate topographical anatomy, and clinical signs may overlap with other pelvic pathologies.[1] Consequently, diagnosis and management of pelvic tumours are problematic in musculoskeletal oncology due to the anatomical proximity of adjacent critical neurovascular bundles, visceral organs and lack of clearly defined, independent prognostic factors.[2] Primary pelvic sarcomas have a poor prognosis, especially those with higher grade variants.[3,4]
With recent advances in diagnostic, oncological and multimodality surgical treatment options, limb salvage surgery has become the primary mainstay of surgical treatment of choice, especially in patients with low-grade pelvic sarcomas.[5-7] As a result, this has reduced the requirement for disabling and disfiguring amputations.[8]
However, given the multiple pelvic resection techniques and novel procedures, postoperative complications remain high. These include wound complications, surgical site infections (SSI), local recurrences, symptomatic venous thromboembolism, implant failure or prosthesis dislocations.[9-11]
In this study, we report a rare postoperative complication, pelvic stress fractures (PSFs), identified in some patients post-hemipelvectomy procedures, which has not been investigated in the literature. We highlight our experience from a tertiary referral oncology centre of incidence and clinical and radiological features, as well as discuss the risk factors for developing PSFs in patients treated with hemipelvis resection.
Methods
Local ethical committee approval was obtained. We retrospectively reviewed patients treated in a single specialised orthopaedic oncology unit. Patients were identified from a prospectively maintained retrospective database that records all patient episodes for patients referred, diagnosed and managed through the service. The computerised radiology information system (CRIS) was utilised to cross-reference patients who had undergone imaging through the unit. A keyword search was performed using the words ‘stress response’ and ‘stress fracture’ on radiology reports of oncology patients over 13 years (between 2007 and 2019). Our inclusion criteria encompassed patients that underwent hemipelvectomy procedures for primary bone tumours with subsequent development of pelvic insufficiency fractures. We identified six patients who fulfilled the inclusion criteria. All cases were diagnosed by magnetic resonance imaging (MRI) and were reviewed by a senior musculoskeletal radiologist to identify the presence of a stress fracture, the location of the stress fracture, the nature of previous surgery, the primary diagnosis and the extent of pelvic resection. The stress fracture was identified as a low linear signal on T1 and stirred with osseous oedema. Osseous oedema without a low linear signal was a stress response. The data was analysed on a spreadsheet using Microsoft Excel software.
Results
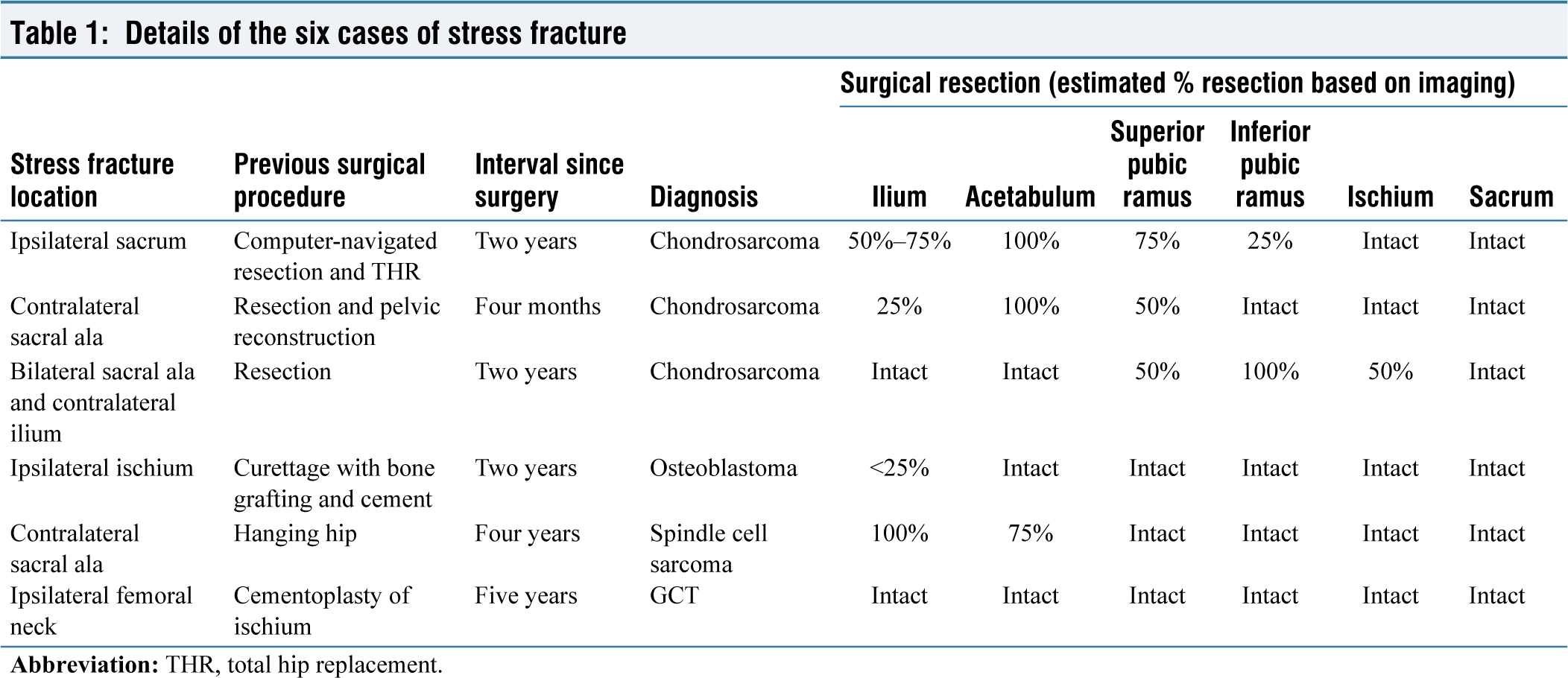
Six cases with pelvic stress fracture post-resection were identified, comprising five females and one male patient, with an average age of 43 years (range: 21-63 years). Three patients underwent pelvic resection for chondrosarcoma, one for a giant cell tumour (GCT) of bone, one for an osteoblastoma and one for a spindle cell sarcoma. Our results showed post-hemipelvectomy PSF most commonly involved the sacrum and sacral ala (n = 3).
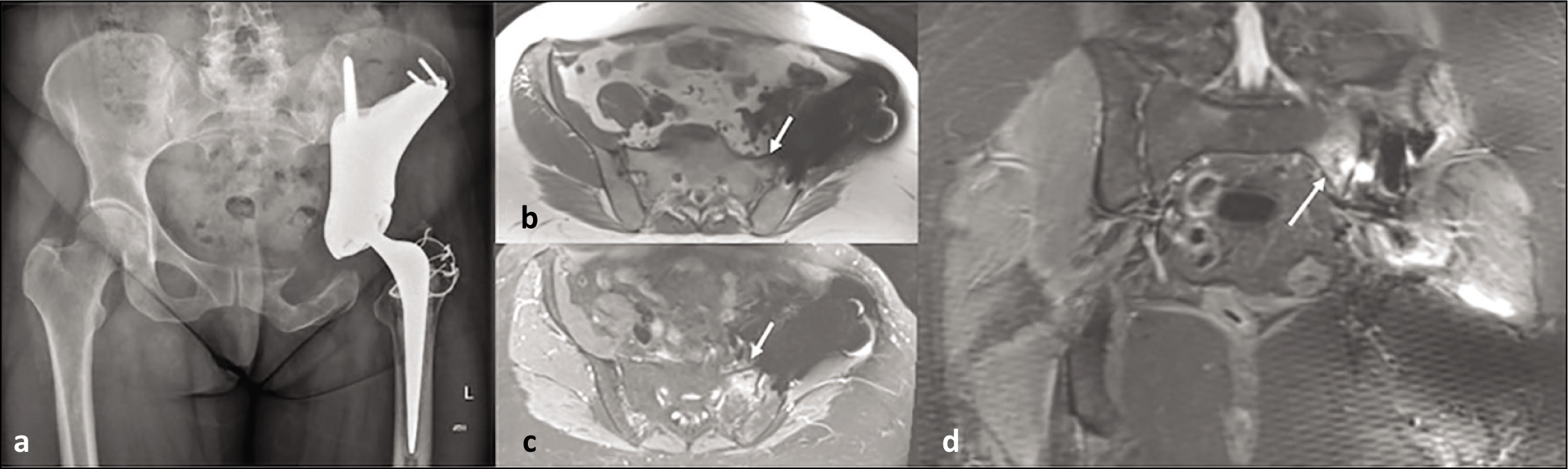
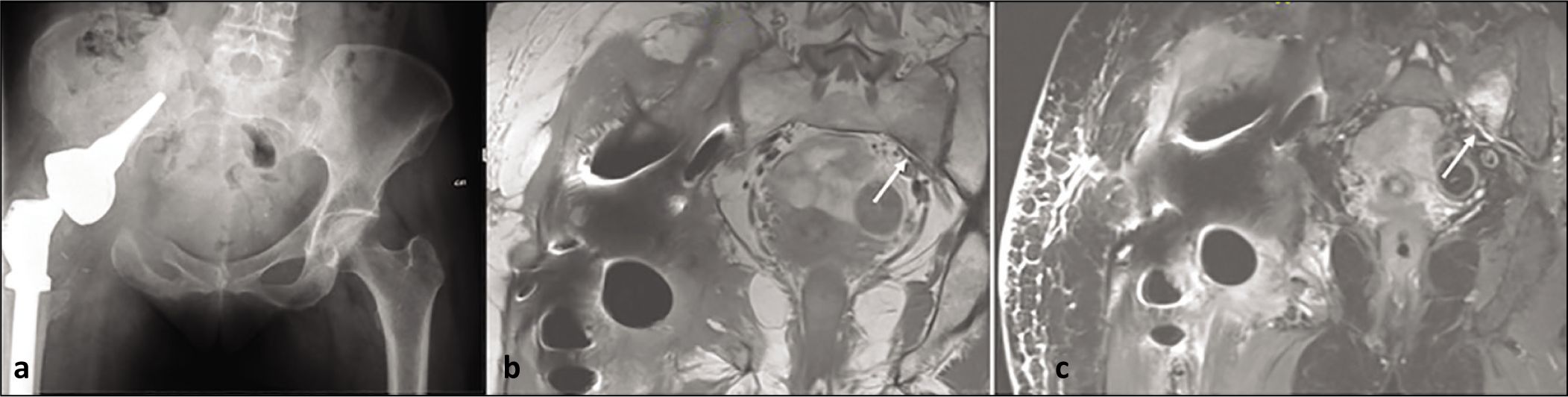
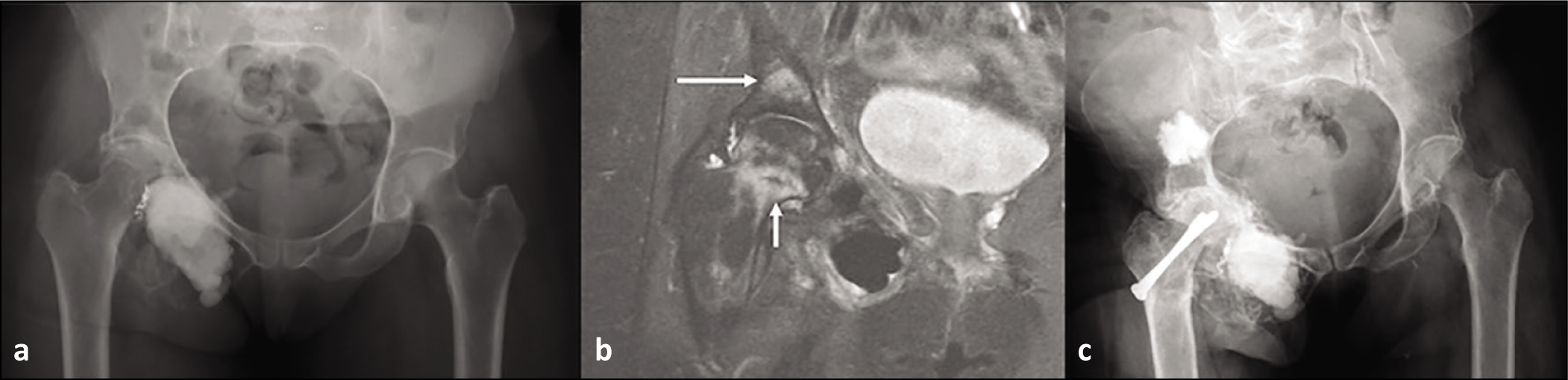
Of the three patients with pelvic chondrosarcoma, one patient underwent computer-navigated partial resection of the ileum, superior and inferior pubic rami and complete resection of the affected acetabulum, with periacetabular reconstruction and total hip arthroplasty. This patient went on to develop an ipsilateral sacral ala insufficiency fracture [Figure 1]. The second patient underwent partial resection of the ilium and superior pubic ramus, complete resection of the affected acetabulum and complex pelvic reconstruction. The latter patient developed a contralateral sacral ala PSF [Figure 2]. The final patient with chondrosarcoma underwent partial resection of the superior pubic ramus and ischium and complete resection of the inferior pubic ramus on the affected side which did not require any formal pelvic reconstruction. This patient went on to develop bilateral sacral ala and contralateral ileum PSF [Figure 3].
AP (anteroposterior) radiograph (a), axial T1(b), STIR (short tau inversion recovery) (c) and coronal STIR showing complex reconstruction of left hemipelvis with an incomplete ipsilateral stress fracture of sacral ala (arrow)
AP radiograph (a), coronal T1 (b) and STIR (c) showing ice cream cone reconstruction of right hip and contralateral incomplete stress fracture of sacral ala (arrow)
AP radiograph (a), coronal T1 (b), STIR (c) and axial STIR showing osseous oedema involving both sacral ala and left posterior ilium

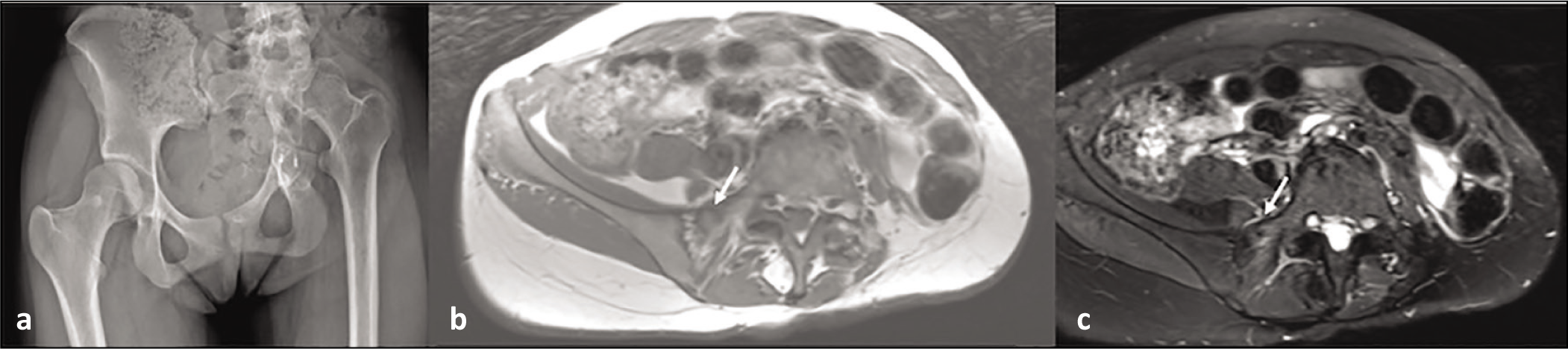
The patient with an osteoblastoma underwent partial (<25%) ileum curettage with bone cement grafting. This patient went on to develop an ipsilateral ischial PSF [Figure 4].
AP radiograph (a) showing cementation and curettage of left ilium; axial T1(b) and STIR (c) showing incomplete stress fracture of the left posterior acetabulum (arrow)
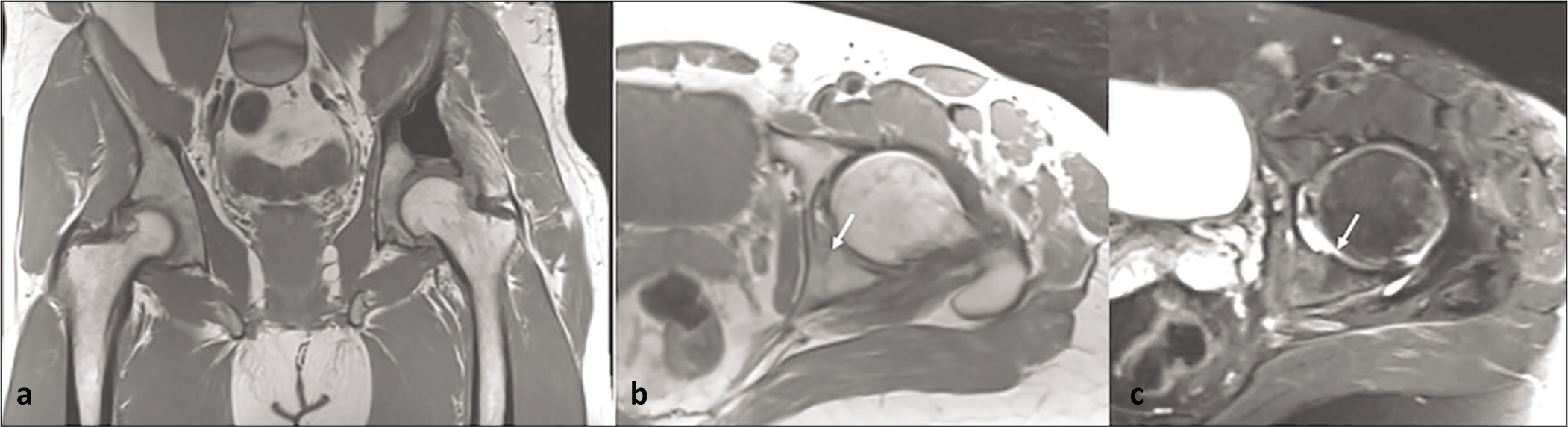
The patient with a spindle cell sarcoma underwent partial acetabulum (75%) and complete ileum resection on the affected side. This patient went on to develop a contralateral sacral ala PSF [Figure 5].
AP radiograph (a) showing resection of left ilium with hanging hip. Axial T1 (b) and STIR (c) showing contralateral incomplete stress fracture of right sacral ala
Lastly, there was one patient with an ischium GCT that underwent cementoplasty. This patient went on to develop an ipsilateral femoral neck and acetabular PSF [Figure 6]. All these results are further summarised in Table 1.
AP radiograph (a and c) showing curettage and cementation of right ischium (a). STIR coronal showing trabecular fractures with osseous oedema of right acetabulum and right femoral neck (b) treated with cannulated screws and cementoplasty (c)
Details of the six cases of stress fracture
Discussion
Primary tumours of the pelvis are rare, comprising 10%-15% of all primary bone malignancies.[12] This site has a preponderance for chondrosarcoma and Ewing sarcoma.[1,3] The incidence of metastatic disease is far more common, with the pelvis the second most commonly affected site.[13]
Historically, the mainstay of treatment for primary malignancies of bone affecting the pelvis was external hemipelvectomy (also known as hindquarter - amputation).[1] However, advances in surgical techniques and the establishment of neoadjuvant chemotherapy and radiotherapy have translated into limb salvage surgery as the principal surgical treatment.[1,14]
In parallel to this advancement has been the development of reconstruction techniques to restore function following tumour resection. The musculoskeletal tumour society categorises pelvic resection surgeries into four different groups, including Iliac resection (type I), periacetabular (type II) os pubis, ischiopubic (type III) and sacral (type IV).[14-16] The difficulty in reconstruction reflects the complexity of each resection.
Depending on the primary location and extension of tumours, various reconstruction methods have been described in the literature. The basic principle of internal hemipelvectomy follows to achieve wide tumour resection margins, with subsequent complex reconstruction, restoring function and improvement in postoperative quality of life.[12]
Despite this, it is estimated that 18%-65% of patients undergoing pelvic resection and reconstruction develop postoperative surgical complications. These may include wound infection, haematoma, recurrence, implant failure, thrombosis or chronic pain.[16-19] To our knowledge, no previous report has looked into the presence of stress fractures following major pelvic reconstructive surgery. In this study, 10.3% of cases developed postoperative stress fractures, visible on follow-up MRI.
Stress fractures are described as ‘fatigue’ or ‘insufficiency’ fractures in the literature, attributed to recurrent submaximal load on the bone.[20,21] They most commonly affect the tibia and metatarsals. PSFs account for only 1.6%–7.1% of all stress fractures.[22] PSF can cause considerable pain, leading to loss of independence and disruption of postoperative rehabilitation. Therefore, early diagnosis and management are essential to ensure patients achieve positive outcomes.
The diagnosis of PSF can be challenging, given the vague clinical presentation and complex interpretation of plain radiographic imaging. Therefore, a high index of suspicion coupled with the clinical context of patients undergoing pelvic resection is warranted. MRI is the gold standard imaging technique to diagnose such lesions and is, furthermore, sensitive to detecting occult PSF.[23] MRI depicts bone marrow oedema with low signal-intensity fracture lines on T1-weighted images.[24]
The reason stress fractures occur following pelvic resection and reconstruction is not known. However, we hypothesise that iatrogenic disruption of the pelvic ring during surgery results in altered biomechanics that lead to stress fractures of the sacrum and pubis. Pelvic radiation for the adjuvant treatment of primary bone tumours is also a risk factor.
Limitations
The strength of study is that we demonstrate a rare complication in series of patients who undergo pelvic resection with or without reconstruction. The limitation of the study is a retrospective study with relatively low numbers; however, considering the complexity of these cases, the findings have a clear message.
Conclusion
PSFs are a potential complication in patients who have undergone pelvic resection with and without reconstruction surgery. Recognition and awareness of this phenomenon are essential to avoid misdiagnosing stress fractures as tumour recurrence on postoperative follow-up MRI imaging and to initiate appropriate treatment.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Institutional Ethical Committee Approval Number
Local committee approval obtained as service evaluation.
Informed consent
Informed consent was obtained.
Credit author statement
Conception and design, or acquisition of data, or analysis and interpretation of data - Kurisunkal V, Parry M, Botchu R Design, or acquisition of data, or analysis and interpretation of data - Saad A, Botchu R Drafting the article or revising it critically for important intellectual content - Saad A, Iyenagar KP, Kurisunkal V, Parry M, Botchu R Final approval of the version to be published - Saad A, Iyenagar KP, Kurisunkal V, Parry M, Botchu R
Data availability
Available further on request.
Use of artificial intelligence
None.