
Abstract
Background and Aims:
Pigmented villonodular synovitis (PVNS) is an uncommon but aggressive proliferative process affecting the synovium. Diffuse pigmented villonodular synovitis (DPVNS) is a type that affects the whole joint and if left untreated, it can lead to joint destruction and osteoarthritis. Only surgical excision can lead to local recurrences in DPVNS. Postoperative radiotherapy can significantly lower the incidences of local recurrences and improve functional outcomes.
Materials and Methods:
Here we present a rare case report of a lady with biopsy-proven DPVNS where postoperative radiotherapy was given.
Results:
At a 48-month follow-up, the patient is free of disease with improved joint function.
Discussion:
Given the improved local control, low morbidity and remarkable improvement in joint functions, postoperative radiotherapy should be routinely considered in cases of DPVNS if complete excision is doubtful.
Introduction
Pigmented villonodular synovitis (PVNS) is an uncommon benign but aggressive proliferative process affecting the synovium among young and middle-aged adults.[1,2] Also known as tenosynovial giant cell tumour, PVNS usually arises in the joints, knee joint being commonest and is more often monoarticular.[3] It can also involve the tendons (pigmented villonodular tenosynovitis, PVTS) and bursa (pigmented villonodular bursitis, PVB).[2] It can be localised (LPVNS) or diffuse (DPVNS). LPVNS usually presents as a solitary pedunculated lesion surrounded by normal synovium, whereas DPVNS is villous and involves the whole joint.[2,3] Microscopic features include fibrous stroma, hemosiderin deposits, giant cells and lipid-laden macrophages. Left untreated, PVNS can lead to joint destruction and osteoarthritis due to its locally aggressive nature. Surgical resection is the primary modality for the management of PVNS. Postoperative Radiotherapy can improve the local control rate.[3] Here we present a case in which long-term local control was achieved by using postoperative radiotherapy.
Case Report
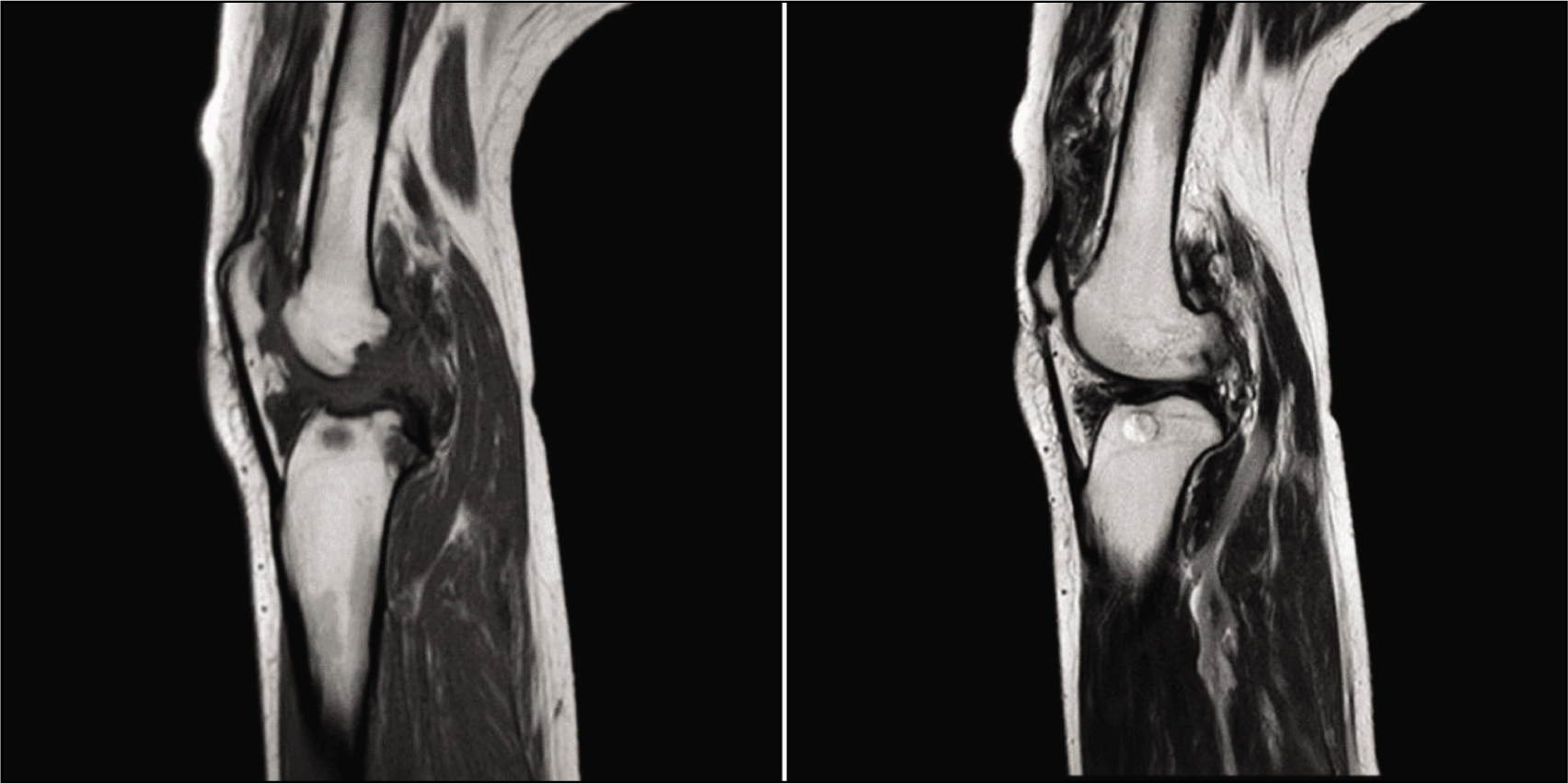
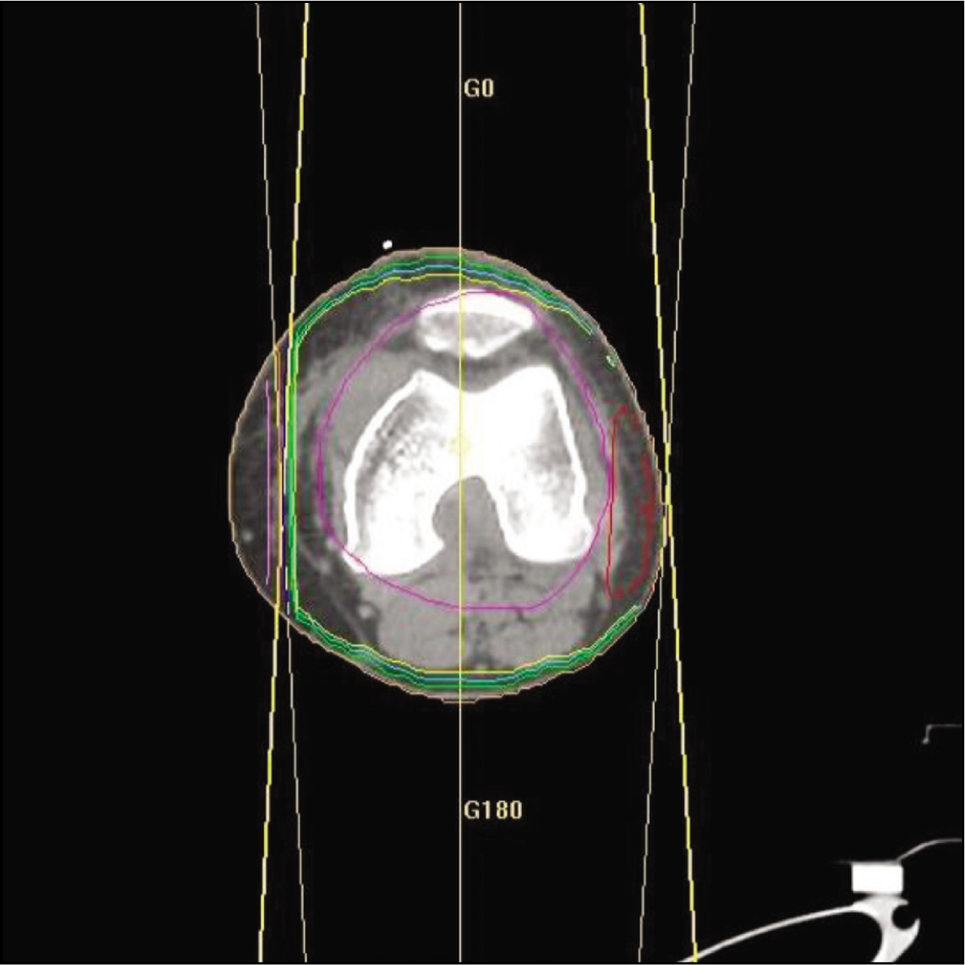
A 35-year-old lady presented with complaints of pain and swelling in the right knee for one year. Following the finding of an osteolytic lesion in the right knee X-ray, a magnetic resonance imaging (MRI) was done which showed diffuse irregular synovial thickening and a frond-like appearance within the knee joint space raising the suspicion of chronic synovitis [Figure 1]. She underwent synovectomy and postoperative histopathology showed synovial hyperplasia within fibrin nodules, siderophages and chronic non-specific inflammation, suggestive of PVNS. Given the diffuse nature of the disease, she received postoperative external beam radiotherapy to a total dose of 30Gy using the three-dimensional conformal radiation therapy (3D-CRT) technique [Figures 2 and 3]. She had significant pain relief and maintained good functionality of the joint at the end of radiotherapy. Treatment course was uneventful with no adverse effects. At a 24-month follow-up, patient is pain-free with no functional limitations. Thus, we were able to achieve excellent local control with surgery followed by postoperative radiotherapy in this case.
MRI knee; features raised the suspicion of chronic synovitis (diffuse irregular synovial thickening and a frond-like appearance within the knee joint space raising the suspicion of chronic synovitis)
Planning CT images (axial) showing the isodose lines. Using 6MV photon beams, a dose of 30Gy was prescribed to the 98% isodose line (sky blue line)
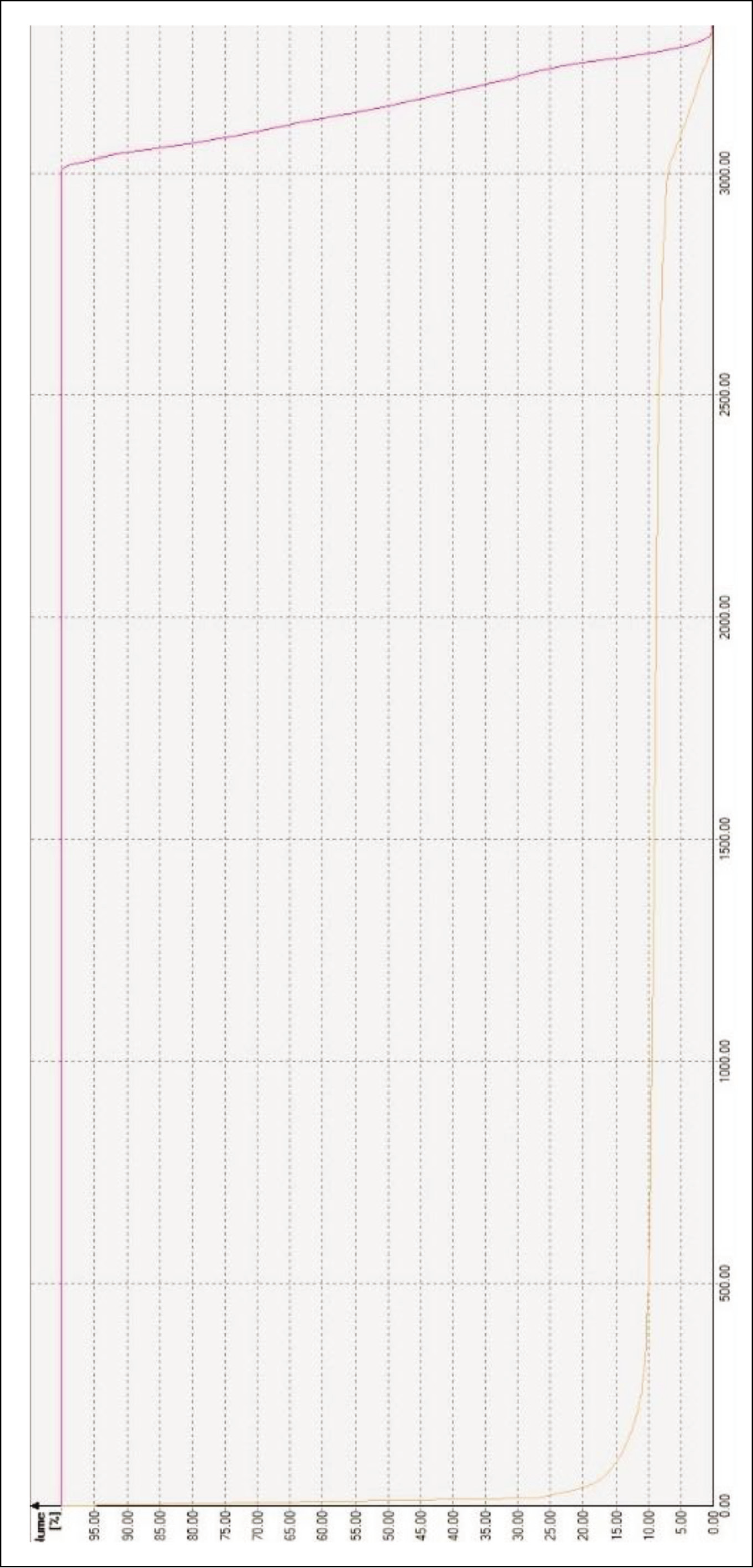
Dose-volume histogram
Discussion
Despite several suggestions, best standard of care for PVNS is still an issue causing dilemma. Staals et al. suggested open surgical resection as the gold standard management for DPVNS.[4] van der Heijden et al. advocated for a cohesive and multidisciplinary treatment protocol for DPVNS.[5] Surgical resection is often the primary treatment modality. While LPVNS has good local control rates with surgery alone, DPVNS is reported to have approximately 50% recurrence rates.[6] In a retrospective analysis of 214 cases, there were 47.6% and 8.6% local recurrence rates for DPVNS and LPVNS respectively after surgery, with arthroscopic techniques having a higher risk than open synovectomy.[7]
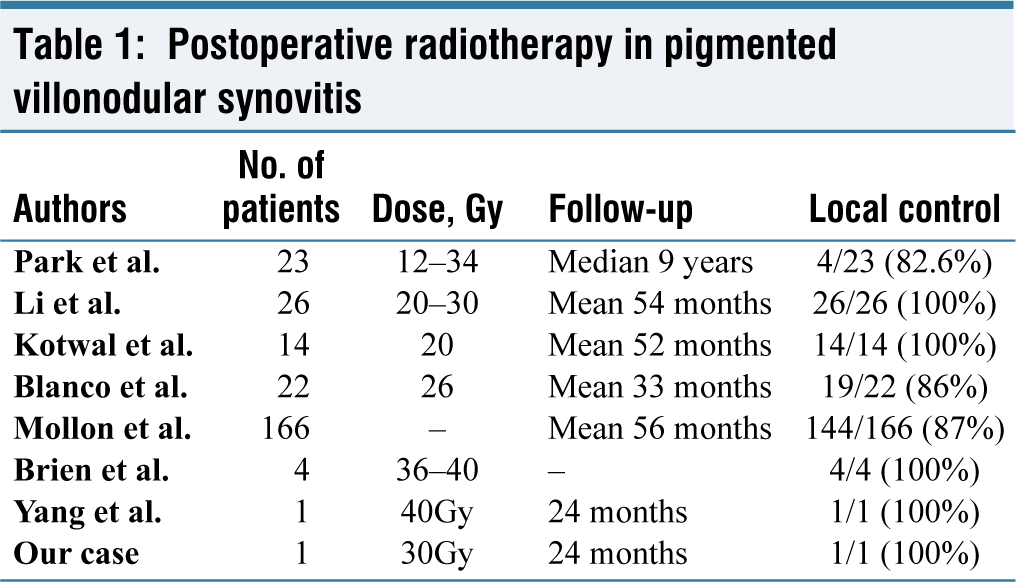
Park et al. reported the outcomes of postoperative low-dose external beam radiotherapy in 23 DPVNS patients. Patients who received a median dose of 20Gy (12-34Gy) had a median disease-free interval of five years. At a median follow-up of nine years, only four patients had recurrences. There were no severe early or late radiation-related adverse events or functional impairments. Twenty-two patients had excellent or good joint function post-radiotherapy.[8] In a retrospective study, 26 DPVNS patients received the planned 10 fractions of radiation (dose range: 20-30Gy). None of the patients who received postoperative radiotherapy (PORT) showed recurrence. Two patients who did not complete the planned 10 fractions had in situ recurrence after six months.[9] In another study, out of 48 PVNS patients, 14 underwent PORT (20Gy) due to incomplete excision or the presence of mitotic figures. No recurrences or complications were observed in those who underwent postoperative irradiation.[10] Blanco et al. treated 22 PVNS patients with postoperative radiotherapy using Cobalt-60 to a dose of 26Gy. At 33 months post-treatment, only four patients had recurrence.[11]
In a large meta-analysis, while 166 out of 448 DPVNS patients received PORT, only 12 patients (12%) had a recurrence. In comparison, 36.9% of the no-radiotherapy DPVNS group had a recurrence. Multivariate analysis showed that peri-operative radiotherapy lowered the recurrence rates irrespective of the type of surgery (open vs. arthroscopic).[3] Brien et al. used repeat excision followed by PORT in four cases that recurred after initial surgery. No recurrences were observed following a higher radiation dose in the range of 36-40Gy which was used given the location of the disease (knee, wrist and ankle joints) where surgery would cause significant functional limitations.[12] Yang et al. reported a case that was managed by surgery and postoperative radiotherapy to a dose of 40Gy. Patient tolerated radiotherapy well and had no local recurrence at a two-year follow-up.[13]
Thus, the available literature on the topic recommends postoperative radiotherapy to prevent local recurrence in extensive tumours, those with positive margins, incomplete excision and/or inaccessible sites of the disease [refer to Table 1]. At a 24-month follow-up, our patient is pain-free with no functional limitations thus achieving excellent local control. Hence, our experience also proves the effectiveness of postoperative radiotherapy in limiting the recurrence.
Postoperative radiotherapy in pigmented villonodular synovitis
Conclusion
Postoperative radiotherapy offers excellent local control in diffuse pigmented villonodular synovitis. Given the improved local control, low morbidity and remarkable improvement in joint functions, postoperative radiotherapy should be routinely considered in cases of DPVNS if complete excision is doubtful.
Footnotes
Acknowledgements
The authors convey their deep-felt gratitude to all those who helped in the process of drafting the manuscript. We thank our colleagues, medical physicists, radiation technologists and sisters for all their work, dedication and cooperation
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional Ethical Committee Approval Number
Not applicable.
Informed consent
Informed consent for radiotherapy was obtained before the treatment.
Patient consent
The authors certify that they have obtained informed consent from the patient. The patient has given his consent for the usage of images, and other clinical information for publication in the journal. The patient understands that his name or initials will not be published, and while all attempts will be made to conceal his identity, complete anonymity cannot be guaranteed.
Credit author statement
This manuscript has been read and approved by all the authors. All the authors believe that the manuscript represents an honest work that contributes to the knowledge pool in the field of radiotherapy.
Data availability
The authors confirm that the data supporting the findings of this study are available within the article.
Use of artificial intelligence
None.