
Abstract
Background and Aims:
Plain film radiography is the first imaging modality in the detection of most foreign bodies. However, it is not sensitive for detection of radiolucent objects such as organic material including plant thorns.
Case report:
Herein, we present the case of a 19-year-old male patient, presenting with an 8-month history of right knee pain and laxity, whose radiographic appearance mimicked that of pigmented villonodular synovitis (PVNS) but was found to have a retained neglected plant thorn in his knee. Upon ultrasound evaluation for image-guided biopsy to confirm the provisional diagnosis of PVNS, he was found to have a retained neglected plant thorn in his knee.
Discussion:
Plant thorn injuries can present as knee synovitis, as in our case, and should be kept in the differential diagnosis. An ultrasound-guided removal is possible and is a useful minimally invasive procedure.
Introduction
Thorn-induced penetrating injuries are a frequent occurrence in rural settings and primarily affect exposed extremities.[1] The imaging modality of choice for detecting most radio-opaque foreign bodies is plain film radiography.[2] However, radiolucent objects such as organic material, including plant thorns, can have similar densities to soft tissue, rendering plain film imaging less effective and increasing the likelihood of retained organic foreign bodies being missed on imaging.[3] When lodged in or near bone, retained plant thorns can produce a pathological response in surrounding osseous structures that mimic the appearance of bone tumours.[4] Maylahn et al. found that these changes can appear osteoblastic, osteolytic, or as a combination of the two on imaging—similar to how bone neoplasms could appear.[5]
Pigmented villonodular synovitis (PVNS) is one such neoplastic disorder of the synovium affecting the soft tissue lining of tendon sheaths, joints and bursae.[6] Specifically, it refers to a subtype of tenosynovial giant cell tumours and usually affects people between 20 and 40 years of age. Intra-articular PVNS is a rare disease, with an estimated prevalence of around 1.8 cases per million population.[7] Although it rarely undergoes malignant transformation, PVNS is a locally invasive disorder that can cause significant bone erosion, has a high recurrence rate and requires surgical excision.[7,8]
We present the case of a 19-year-old male patient who was provisionally diagnosed with PVNS but was found to have a retained plant thorn in the knee upon ultrasound imaging which was removed under ultrasound guidance.
Case Report
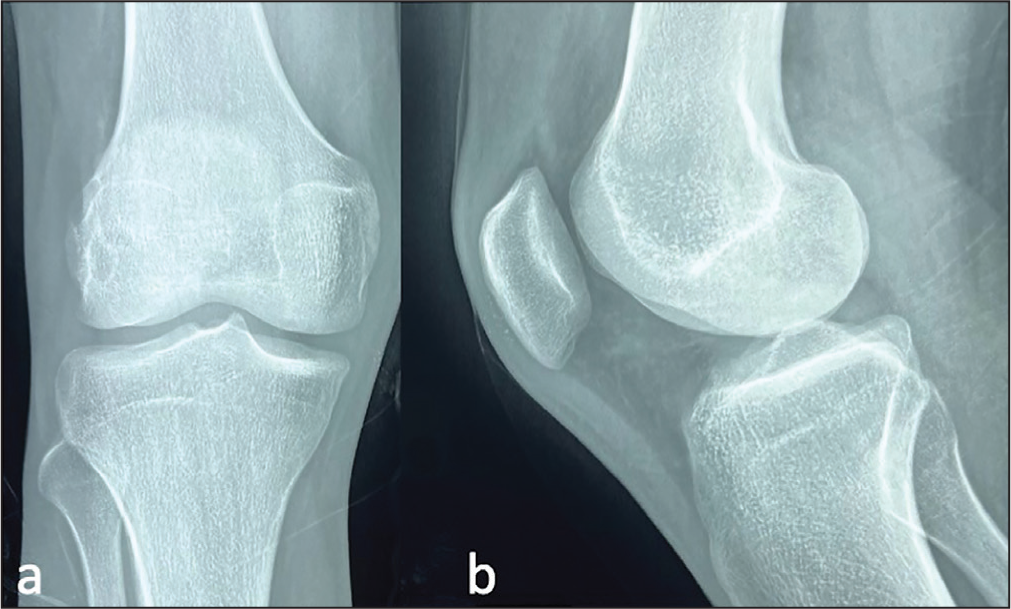
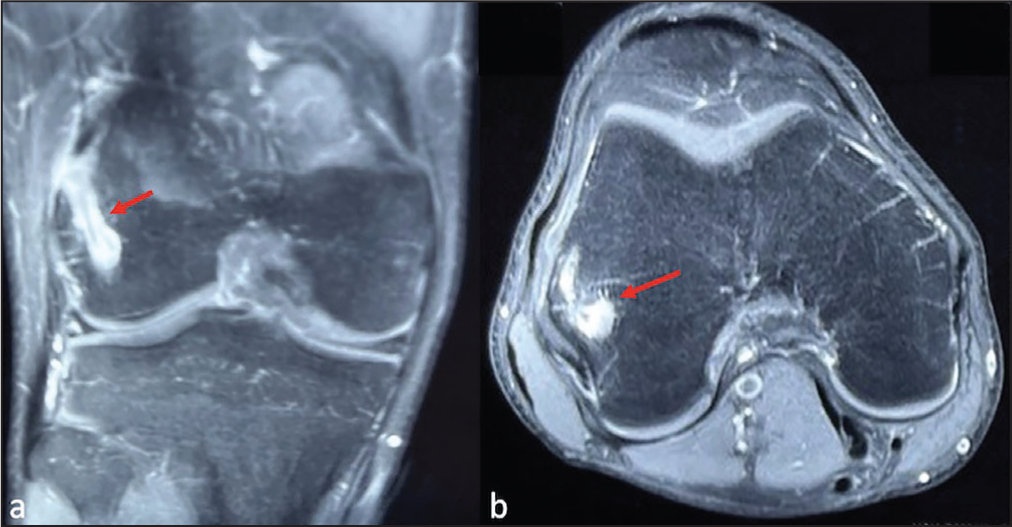
A 19-year-old male patient presented with primary complaints of persistent right knee pain and laxity for 8 months without any history of trauma or puncture wounds. On initial assessment, the skin was normal, without effusion and the range of movement of the knee was restricted due to pain. No joint tenderness was noted. Magnetic resonance imaging (MRI) revealed a tear of the anterior cruciate ligament (ACL) and he was scheduled for ACL reconstruction. However, on radiographs and MRI, a burrow lesion was also noted on the lateral femoral condyle, coinciding with the path of the femoral tunnel intended to be used for ACL reconstruction (Figures 1 and 2). This was suspected to be PVNS burrowing into bone thus, the patient was referred for ultrasound-guided biopsy and subsequent histopathological examination to confirm the provisional diagnosis of PVNS.
Anteroposterior (a) and Lateral (b) Radiographs of Knee
PDFS (Proton Density Fat Suppressed) Coronal (a) and Axial (b) of Knee Showing Oedema in Relation to Lateral Femoral Condyle (Arrow)
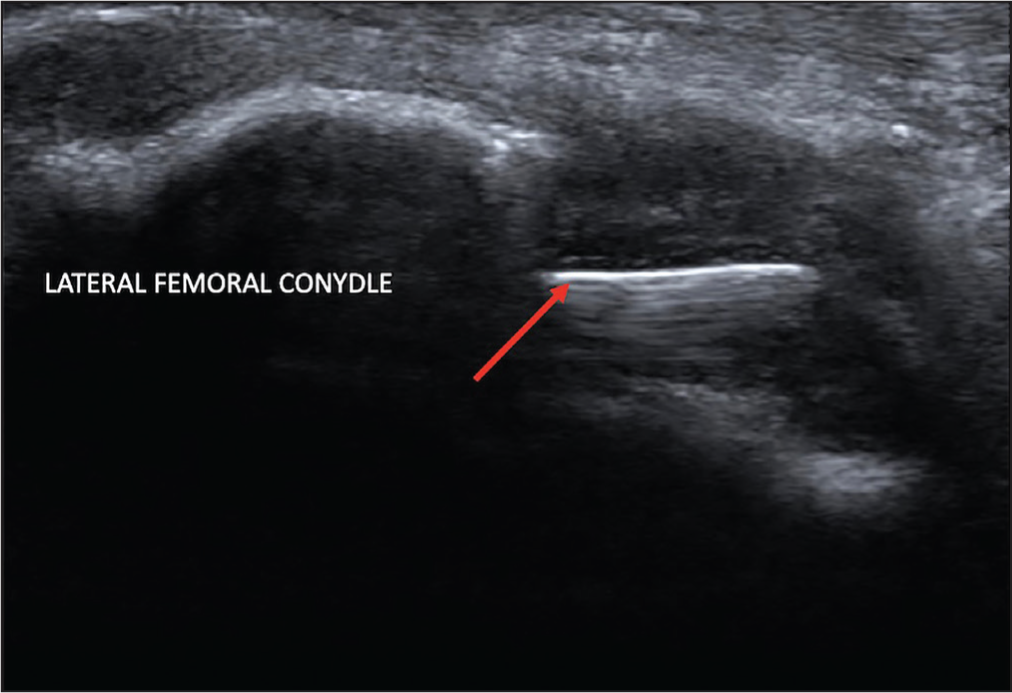
Ultrasound (US) examination, used for the purposes of guiding biopsy, surprisingly revealed an intraosseous linear foreign body (27 mm in length) into the lateral femoral condyle with overlying soft tissue swelling (Figure 3).
Ultrasound Image of the Lateral Femoral Condyle Showing Foreign Body (Arrow)
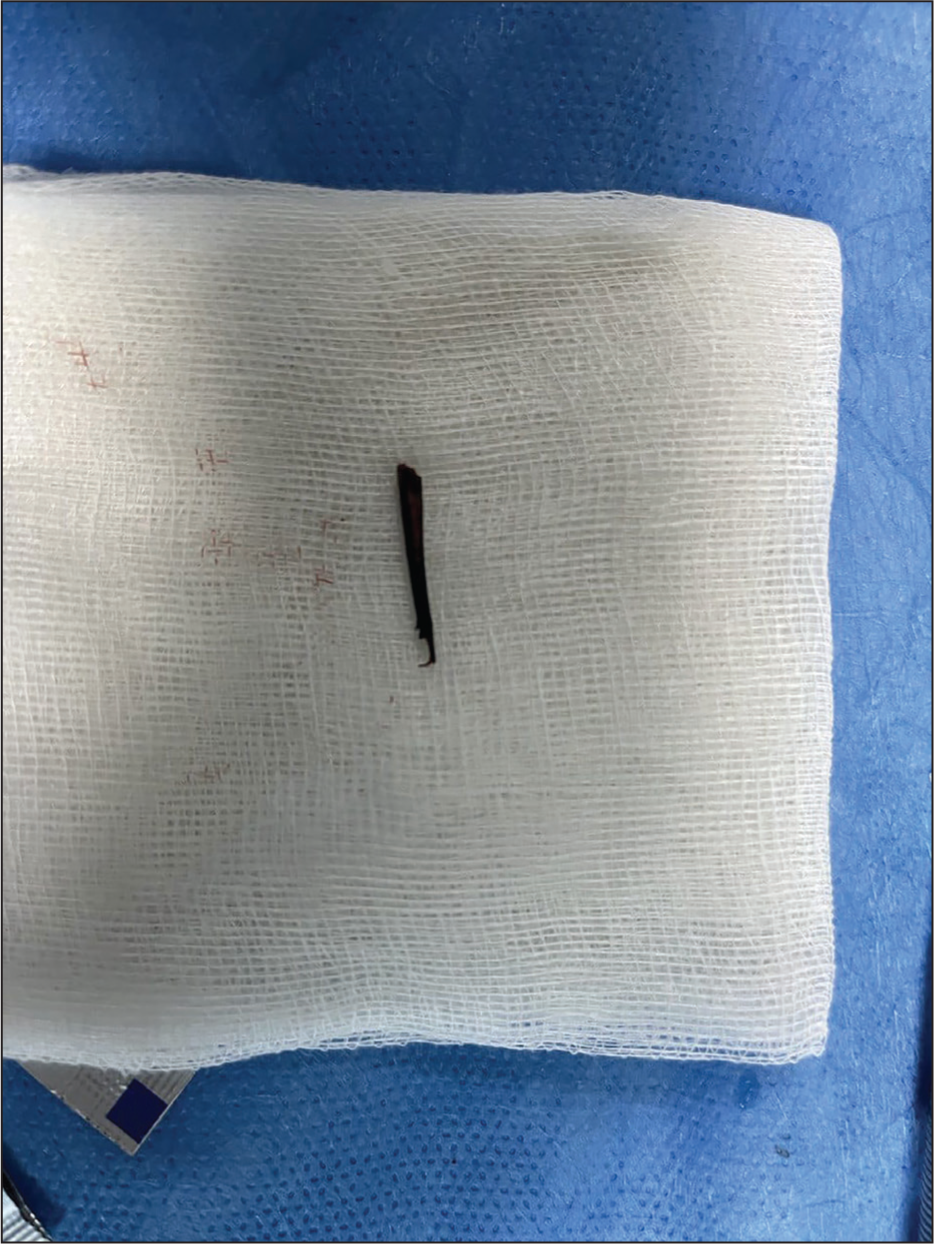
A decision was made to proceed with US-guided removal of the foreign body, which was successfully achieved (Video 1) (Figure 4). Post-procedure monitoring and follow-up indicated significant improvement in knee stability, pain reduction and functional status in the patient.
Discussion
Various types of foreign bodies in the knee have been discussed in past literature, including glass, needles and plant thorns[9-11]; however, most of these cases have been attributed to specific traumatic events, history of self-harm or iatrogenic causes. In our case, the absence of a specific traumatic event in the patient’s history made detection of the foreign body more challenging—which bears resemblance to the case presented by Sharma et al.[12] It is believed that in penetrating wounds involving the musculoskeletal structure, initial wound healing is followed by an asymptomatic period after which clinical and radiological signs manifest. This period is quoted to range between 4 and 16 weeks and may cause the patient to forget or overlook the traumatic incident[13] which is what we suspect may have happened in our patient. It is particularly important to highlight the importance of clinical history and degree of clinical suspicion for foreign bodies in those exposed to greater risk—including children, patients with psychiatric illnesses, and those with sensory deficits or substance misuse disorders.
The incidental discovery of foreign bodies in the musculoskeletal system is a rare occurrence, as reported by Jarraya et al.[14] Typically, patients with foreign bodies embedded in the musculoskeletal system present with signs of complications, with up to 25% of patients developing infection, neurovascular/soft tissue injuries, or granulomatous reactions around the foreign body.[14] Symptoms can be variable. Intra-articular foreign bodies, specifically, have been reported to mimic various pathologies including monoarticular arthritis, torn menisci, chondral lesions, and neoplasms.[15] Vaishya et al. described thorn-related synovitis in children as well as acacia thorn injuries and related complications.[16,17] In our case, a burrow lesion in the lateral femoral condyle was noted on the MRI which was initially suspected to be PVNS given the absence of other explicable causes. Although a characteristic ‘blooming’ appearance is seen on gradient echo images due to haemosiderin deposition in patients with PVNS, it is notably less pronounced in cases of focal PVNS, as suspected in our patient, for which we could not rule it out.
Ultrasound has been shown to be highly specific and sensitive for detection of such organic foreign objects and should be used even in the presence of a negative plain radiograph, if a retained foreign body is suspected.[18] Ultrasound-guided retrieval of foreign bodies in accessible locations is a minimally invasive daycare procedure.
Conclusion
This report describes the case of a 19-year-old male patient who was suspected to have PVNS but later found to have a retained neglected foreign body (plant thorn) which could not be detected radiographically. In such cases, ultrasound may be utilised to pick up on possible retained foreign bodies and guide their percutaneous removal.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author Rajesh Botchu is a member of the Editorial Board of Apollo Medicine. The author did not take part in the peer review or decision-making process for this submission and has no further conflicts to declare.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
No ethical committee approval was required as its a case report with anonymised images.
Informed consent
Written informed consent was obtained from the patient.
Credit author statement
All authors contributed significantly towards the project.
Data availability
Not applicable.
Use of artificial intelligence
No.