
Abstract
Self-esteem refers to the individual’s perception or subjective appraisal of one’s own self-worth, self-confidence and self-respect. Self-esteem plays an important role in determining and preventing mental health disorders. There is a dearth in the knowledge of understanding self-esteem among Indian urban slum adolescents; therefore, this study was taken to assess self-esteem among adolescents of an urban poor locality using ‘The Rosenberg Self-esteem scale’. A cross-sectional survey among adolescents aged 15 to 19 years was conducted from April to June 2023 in the urban poor locality of Bangalore. Taking prevalence of low self-esteem among adolescents as 15.3%, the sample size was calculated as 200. Out of 200 subjects, 52.7% were females and 47.5% were male. We found that 28.0% were school dropouts. The study showed a majority of the subjects had normal or high self-esteem and 10.5% had low self-esteem.
Increasing age of the adolescents was found to be significantly associated with self-esteem scores (p < .05). This study identified that 10.5% had poor self-esteem and they need support from family, school and Sneha Clinic at Urban Primary Health Centre to improve their life skills and prevent mental health issues in adolescence and adulthood.
Introduction
The term self-esteem is derived from the Greek word meaning reverence for self. Reverence means respect. It refers to the individual’s perception or subjective appraisal of one’s self-worth one’s feeling of self-confidence and self-respect. Self-esteem is a positive or negative orientation towards oneself (Rosenberg 1965).[1]
Self-esteem is an emotional quality of humans that begins with birth and develops with the individual with fluctuations over the age groups. Age, gender, various cultural contexts and socioeconomic elements, including friends, family and the school environment are known to have an impact on one’s level of self-esteem.[2] Over the years researchers have validated the association of high self-esteem with educational achievement and that the low levels may influence the occurrence of mental health disorders like stress, anxiety and depressive symptoms.[3,4]
Research on self-esteem throughout an individual’s life has shown that although levels of self-esteem were high during childhood, they decreased during adolescence, gradually increases during adulthood, and then decreased once old age approaches.[5-7] Regardless of gender, socioeconomic status (SES), ethnicity or nationality, this trajectory largely held true. Thus, adolescence (10–19 years) is identified as a period of declining self-esteem.[8]
It is noteworthy that adolescents constitute 1.2 billion world’s population and account for approximately 253 million of the Indian population. As this age group later advances into adulthood, they form the future working population of the nation.[9] It becomes necessary to assess their self-esteem as adolescent boys and girls who have a high sense of self-worth exhibit greater accomplishment and outperform their classmates in comparable situations.[10,11] They also have the critical qualities of self-assurance, strong self-esteem, divergent thinking and creativity. Teenagers’ levels of self-esteem also affect their behaviour in society, attitude towards challenges, learning capacities and life skills in addition to their academic performance.
Conversely, low self-esteem is acknowledged as one of the precursors to mental illnesses such as anxiety, sadness and self-doubt. Raising children’s and teenagers’ self-esteem is, therefore, crucial for parents and educators.[12]
School health surveys concentrate on the physical health of the child/adolescent and less frequently do we think of the mental well-being of this age group. However regular screening must also be done for common social ailments like anxiety, depression and perceived stress needs to be considered as well. To tackle this, RMNCH+A by Govt of India has now brought in comprehensive health care for adolescents which includes mental health in the form of ‘Sneha Clinic’.[13] But the implementation and utilisation of the services are still in a preliminary stage leaving the adolescents still as a vulnerable population.
As we have evidence of low esteem being an important risk factor for common mental illness, evaluating the self-esteem scores among adolescents would help to identify those at high risk.
There exists a gap in the knowledge of self-esteem of adolescents living in impoverished urban areas. Since these adolescents are at high risk of other social and health issues, evaluation of self-esteem among adolescents of urban poor localities would serve as a yardstick in assessing the risk for mental health issues. In this background, this study was conducted to assess the self-esteem among adolescents using ‘The Rosenberg Self-esteem scale’[14] and to identify adolescents with low self-esteem.
Materials and Methods
A cross-sectional study was conducted in the urban field practice area of a medical college in Bangalore from April to June 2023. A study by George et al showed that 15.3% of the subjects had low self-esteem.[15] With an absolute precision of 5%, the sample size was calculated to be 200.
Urban field practice area, Yarab Nagar, with 14 wards and a total population of 45585 was the sampling frame. Subjects were selected by population proportion to sample size from each ward. Within each ward door-to-door survey was done and adolescent girls and boys aged 15–19 years who met the inclusion criteria were selected till the target sample size was achieved.
After obtaining informed consent and assent, the adolescents were interviewed using a pretested, semi-structured questionnaire and data regarding the sociodemographic profile, education details of the adolescents, education details of the mothers and self-esteem was assessed using the Rosenberg self-esteem scale (10-item).[14]
Rosenberg self-esteem scale: There were five items for positive self-esteem and five items for negative self-esteem. They were scored for positive self-esteem as 3 for strongly agree, 2 for agree, 1 for disagree and 0 for strongly disagree. Reverse scoring is done for negative self-esteem. The total score of self-esteem ranged from 0 to 30 for 10 items. Levels of self-esteem were classified as high self-esteem (25–30), normal self-esteem (15–25) and low self-esteem (0–15).
The Institutional Ethics Committee clearance was obtained and confidentiality of the data was maintained at all times. The data was then entered in MS Excel 2019 and was analysed for frequencies and percentages and inferential statistics like chi-squared test were used and p < .05 were considered statistically significant.
Results
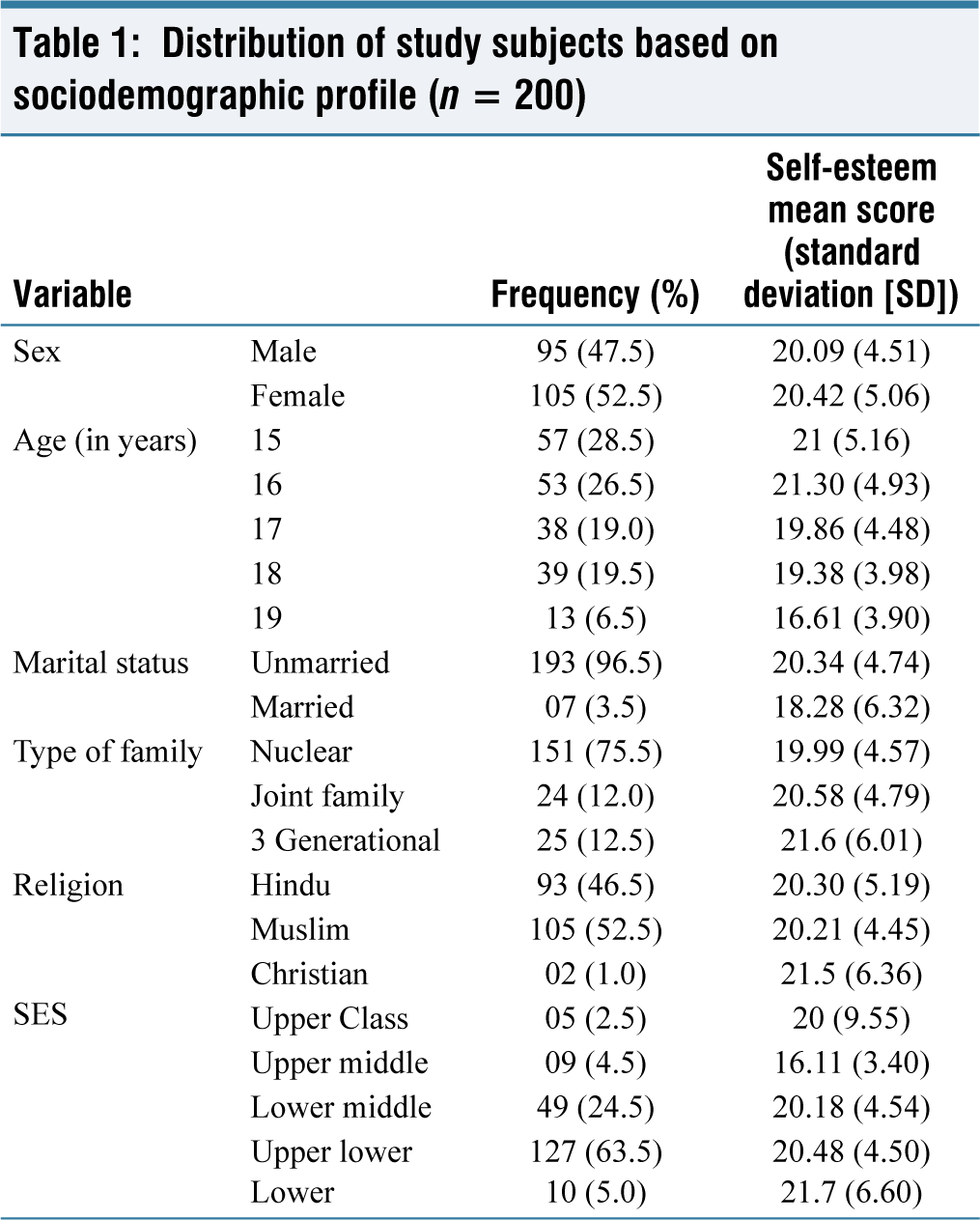
The mean age of the study population was 16.49 + 1.3 years. The youngest study subject was 15 years of age, and the oldest subject was 19 years of age. In the study population, 105 (52.5%) were females of which 7 (3.5%) were married and 47.5% were males. Majority (151; 75.5%) belonged to the nuclear family, and 105 (52.5%) subjects were Muslim by religion [Table 1].
Distribution of study subjects based on sociodemographic profile (n = 200)
The mean score of self-esteem among adolescents was 20.27 (+4.8). The majority of the study subjects (72.0%) had normal scores, 17.5% had high scores and 10.5% had low self-esteem scores [Pie chart 1].
Self-esteem of adolescents
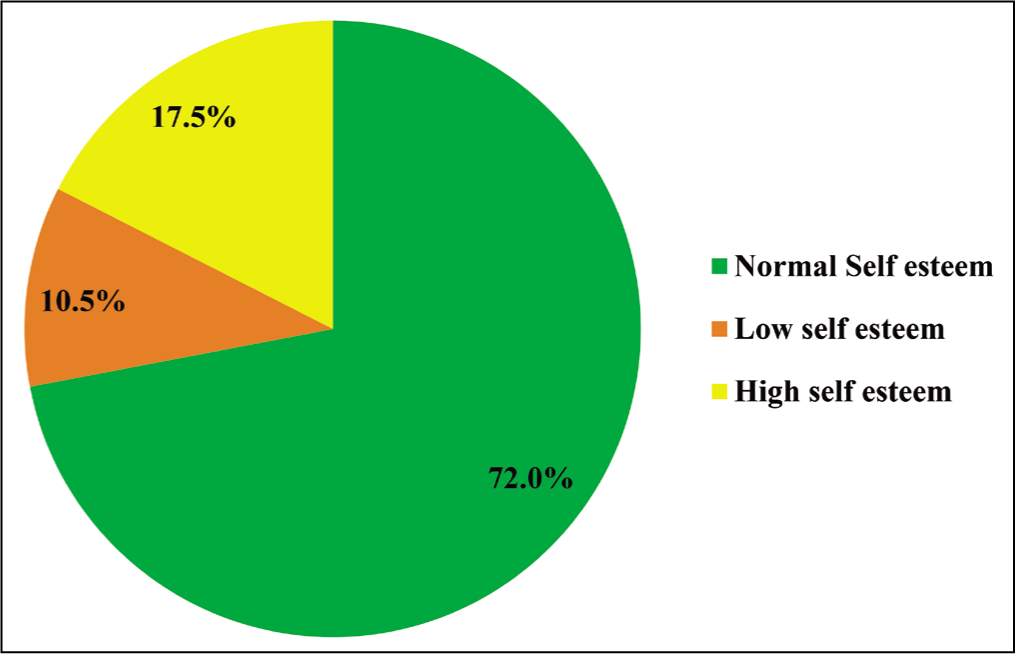
Table 2 shows the classification of self-esteem according to gender; it was observed that 73.7% of the boys and 70.5% of the girls had normal self-esteem scores and the difference in self-esteem scores between the genders was not statistically significant.
Levels of self-esteem and the associated risk factors
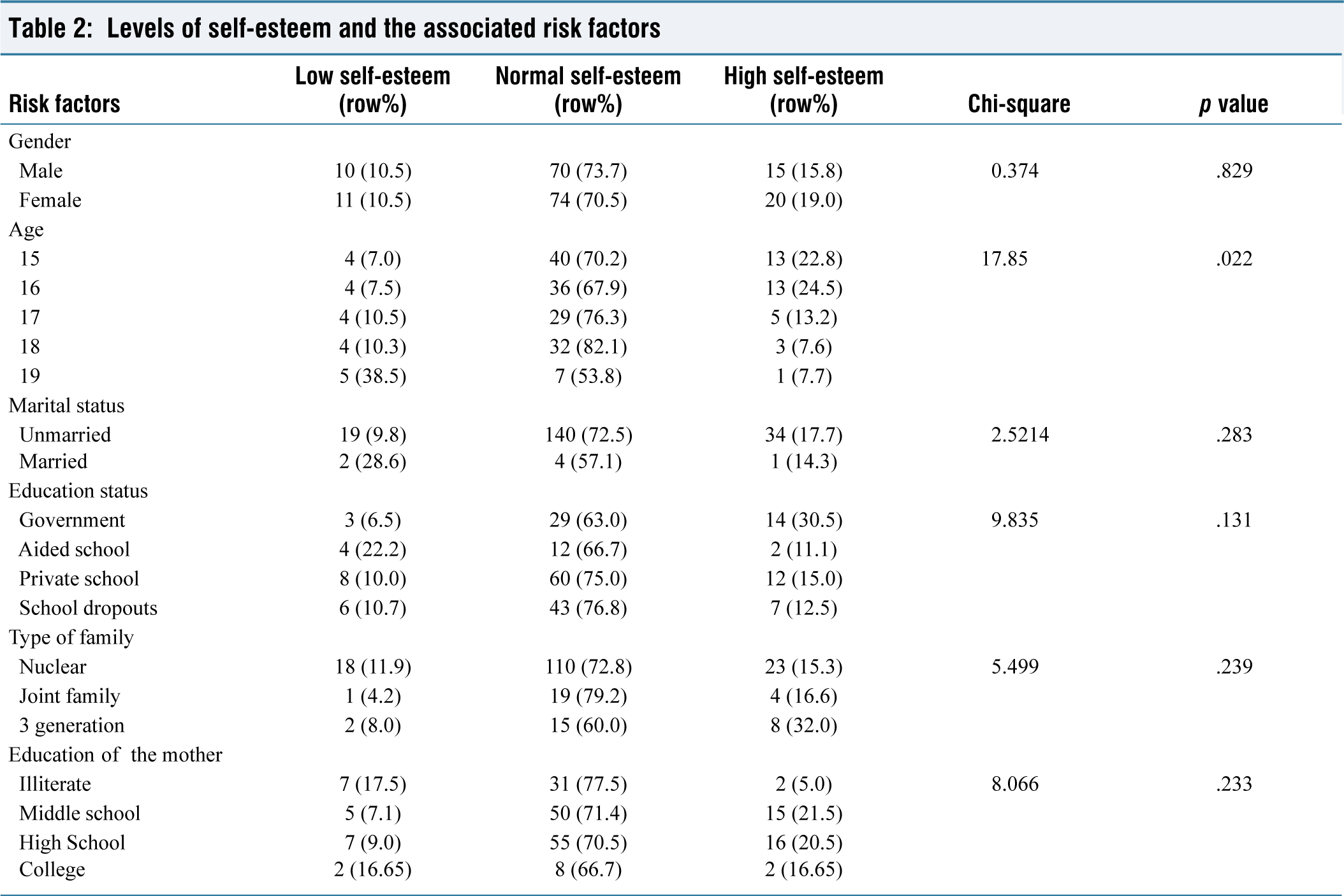
The score of self-esteem of the study subjects and the risk factors present in them were assessed using analytical statistics (chi-squared test). Self-esteem scores were found to be significantly influenced by the age of the study subjects (p < .05). Majority with high scores (74.3%) and normal self-esteem scores (52.8%) belonged to young adolescent age group (15 and 16 years.) No statistically significant association was found between the self-esteem scores and the other sociodemographic risk factors like gender, marital status, type of school, type of family, SES and mother’s education [Table 2].
Discussion
Adolescence bridges childhood and adult life with transitions in physical, physiological and psychological aspects of life. Self-worth/self-esteem and self-identity are the emotions that adolescents start looking for. Robins and Trzesniewski found that although self-esteem levels were high in childhood, it declined during adolescence and then steadily increased throughout adulthood, once again declining in old age. Regardless of gender, socioeconomic level, ethnicity or nationality, this tendency largely held true. Thus, adolescence is identified as a period of decreased self-esteem.[8]
This study quantified the prevalence of low self-esteem among the adolescents of the urban poor locality of Bangalore city. Among 200 study subjects, 10.5% had low self-esteem. Majority had normal and high self-esteem scores. This is similar to the findings of Raju, which showed 8.33% had low self-esteem scores.[7] A study by D’Mello in Dakshina Kannada district shows 24% of the adolescents’ studies with low self-esteem scores. This difference may be because of the exclusion of young adolescents in this study. The latter study was done exclusively among low academic performers (<60%) of the school. Hence, the proportions of low self-esteem students were comparatively higher than in our study.[10]
Factors known to influence the self-esteem were studied as per the feasibility. Evidence of gender, age, education status, parents’ education and SES effecting self-esteem were documented in this study.
The mean scores of self-esteem were similar among both genders. While boys and girls report similar levels of self-esteem during childhood, a gender gap appears by adolescence, with adolescent boys reporting greater levels of self-esteem than adolescent girls.[8] However, in a study done by Mandal et al among rural adolescents in West Bengal, girls showed higher levels of self-esteem than boys. The difference may be due to the change in the study settings.[16]
With respect to age in relation to self-esteem scores, adolescents <15 years had higher self-esteem than older adolescents. The association of the self-esteem scores with the age of the study subjects was found to be statistically significant (p = .02) [Table 2]. The findings are convergent with those of Hirsch and DuBois where 120 adolescents were followed up for transition from elementary to junior high school.[17] The fact that self-esteem declines with age also supports the findings of our study.[8]
Marital status of the individual did not seem to contribute to the scores of self-esteem [Table 2]. However, we regard the results to be unconclusive as majority of study subjects were unmarried and the comparison is not appropriate with very few married individuals. A larger sample size is needed to correlate with these findings. On the contrary, a study by Ahmed et al showed that early marriages resulted in decline in their self-esteem, the reasons possible being domestic pressure, fear of husband/in-laws etc.[18] Meta-analysis of longitudinal studies by the American Psychological Association has relieved that social relationships (general/specific) are reciprocally related to self-esteem at all stages of human life.[19]
Mean scores of self-esteem were found to be similar across all the SES groups except for the upper middle which had low scores of self-esteem but no statistically significant association was found between them. The findings were similar to the study by Rosenberg et al., which explains that self-esteem remains unaffected by SES among children, has a moderate effect among adolescents and can significantly impact theself-esteem of adults.[20]
Information on the education status of study subject’s mothers showed no significant relation with the self-esteem of the study subjects. This is similar to the study in Iran by Solanti et al.[21] Likewise, school where they study and type of family also did not yield any statistically significant differences in the self-esteem scores of the individuals under study. Both school-going and school dropouts had normal self-esteem scores. However, studies done by others have documented education status of mothers, parenting, SES and family to have an influence on the self-esteem status of the children/adolescents.[22]
Conclusion
In this study, it was found that majority of the subjects had normal to high self-esteem scores. We were able to identify 10.5% of adolescents among our study subjects (200) who needed attention. Increasing age was the influencing factor for low self-esteem scores among adolescents in the study.
Recommendations
Routine screening for self-esteem scores using a simple Rosenberg’s scale can help in identifying adolescents at risk of mental health problems. Those with low self-esteem scores need to be reached out on a priority basis as they are at high risk of mental disorders. This can be done by ensuring continuous support from family, teachers and peers. Empowering these adolescents to excel academically or by imparting vocational skill training can enhance their self-esteem.
Urban Primary Health Centre resources in the form of Sneha Clinic and counselling by staff can also help in uplifting self-esteem. This in turn could make adolescents less vulnerable to mental health disorders like anxiety and depression in the future.
Limitations
Young adolescents (10–14 years) were excluded from the study due to difficulties in comprehension of the questionnaire. Large sample is required to understand the effect of marital status on self-esteem.
Footnotes
Acknowledgements
The authors would like to thank all the study participants and their parents for the support in conducting the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Institutional ethics committee number: KIMS/IEC/A123/M/2023.
Credit author statement
Dr Jayanthi Srikanth: Concept proposal, guiding through study, review of the final write-up of the research article, and critical appraisal.
Dr Sridevi Kulkarni: Plan the study, data analysis, and literature review, prepare the manuscript's final version, and correspond with the journal for submission.
Dr Niveditha Sharma: Permission from IEC, data collection, data entry, data analysis, and manuscript draft preparation.
Data availability
Data set is available.
Use of artificial intelligence
Artificial intelligence was not used in any stage of research and write up.