
Abstract
Background and clinical presentation:
The adrenal hydatidosis is an exceptional site location for the occurrence of hydatid cyst with an incidence of being 0.073%. We hereby report this rare case of adrenal hydatid cyst in a 38-year-old male who presented with a history of right flank pain and no other associated complaints. On non-contrast computed tomography/high-resolution computed tomography, the whole abdomen revealed the finding of an adrenal hydatid cyst. He underwent laparoscopic right adrenalectomy, which was further confirmed with the pathological examination. In an adjunct to this, he was put on anti-helminthic drug Albendazole. On one year of follow-up, there was no recurrence.
Conclusion:
The hydatid cyst rarely occurs in the adrenal glands and is an uncommon pathology. It should always be suspected in the case of any cystic tumour of the adrenal gland, especially in endemic countries. The clinical features are variable and non-specific in the majority of the cases. Ultrasonography and CT abdomen hold a significant sensitivity in the diagnosis of the hydatid cyst. Surgical excision is the main choice of treatment. Adjunctive medical treatment improves the outcome and decreases the recurrence rate.
Introduction
Hydatid cyst is anthropozoonosis caused in humans by the larval form of Echinococcus granulosus. It affects all organs and tissue in the human body, with liver (45%–77%) and lungs (10%–50%) being the most common sites of involvement.[1,2] However, adrenal gland hydatidosis is exceptional with an incidence of being 0.073%.[3] Parasitic cysts involving adrenal glands are usually secondary or a part of generalised echinococcosis. They remain asymptomatic for years and are detected incidentally during the course of imaging conducted for some other reason. The differentiation of cystic adrenal hydatid form from other adrenal cysts and adrenal solid tumours with cystic change poses a diagnostic challenge on imaging alone and is quite difficult, especially in large-sized cysts. We hereby report this rare case in a 38-year-old male who presented with vague abdominal pain since last two years. On laparoscopic adrenalectomy, it was diagnosed as adrenal hydatidosis. On follow-up, the patient was quite stable.
Case Report
A 38-year-old male presented with vague abdominal pain since last two years in the right flank at the Department of Surgical Oncology. Ultrasonography performed two years ago showed a right suprarenal mass with no definitive diagnosis. He had no history of hypertension, palpitation and syncopial attack. His serum cortisol, adrenocorticotropic hormone, metanephrine and normetanephrine were within normal limits. On general physical examination, his vitals were stable. On systemic per abdomen examination, he had tenderness in the right flank region. There was no other abnormality detected. Subsequently, a repeat non-contrast computed tomography/high-resolution computed tomography (NCCT/HRCT) and a contrast-enhanced computed tomography (CECT) study of whole abdomen were done at our centre at the time of admission.
Imaging Findings
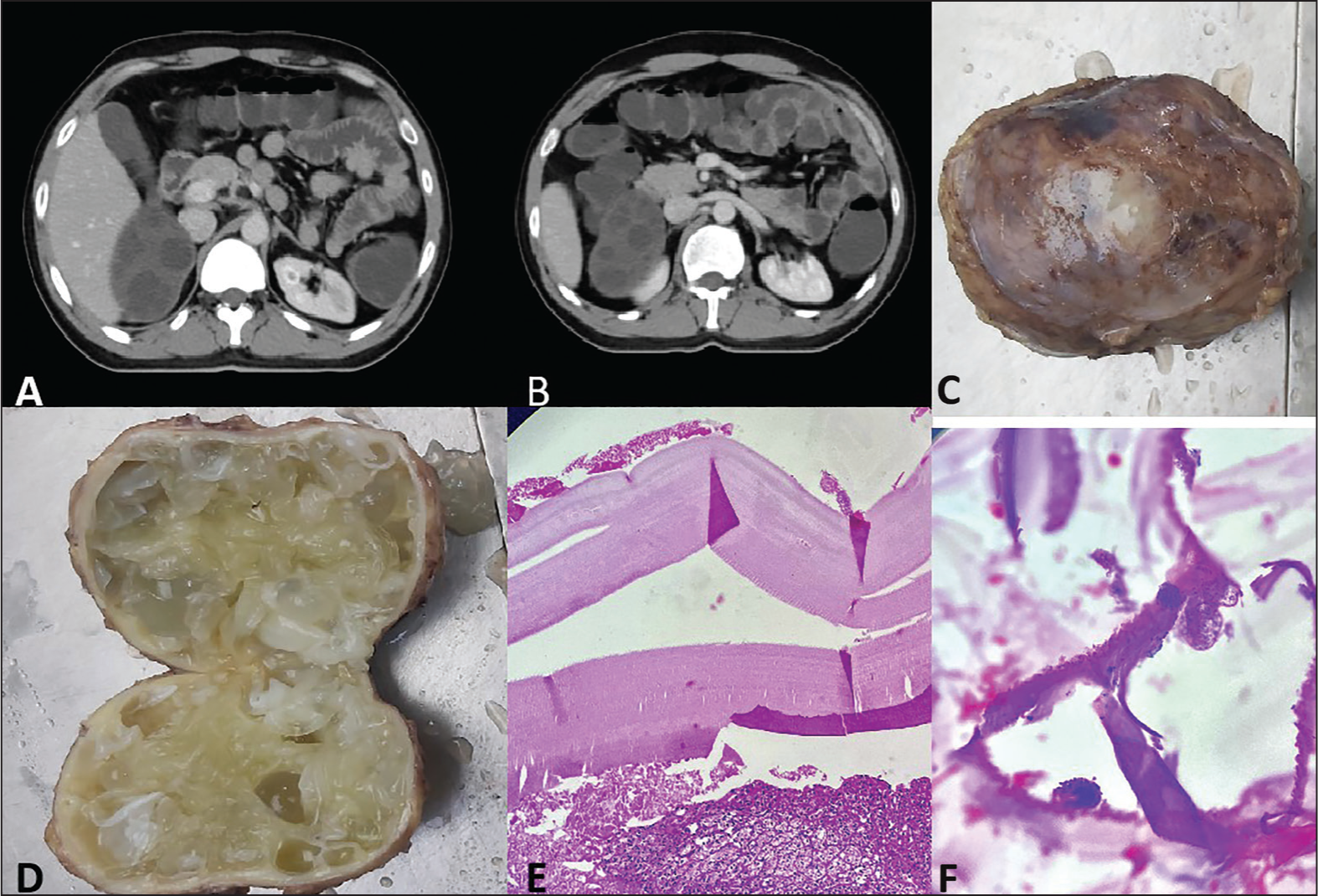
The NCCT/HRCT and CECT study of whole abdomen revealed a large, non-enhancing, multiloculated mass lesion/space-occupying lesion in the right suprarenal region, with non-visualisation of right adrenal gland separately, measuring approximately 8.3 × 6.3 × 6 cm.[3] The left adrenal gland was normal in size, shape and density. Features are likely to be benign lesions, most likely representing a right adrenal hydatid cyst. Further evaluation with hydatid serology and MRI was suggested. In view of this radiological diagnosis, the patient underwent laparoscopic right adrenalectomy [Figure 1A and B].
(A and B) NCCT/HRCT whole abdomen revealed a large, non-enhancing, multiloculated mass lesion/space-occupying lesion in the right suprarenal region; (C and D) gross photograph of adrenal gland with jelly-like vesicles; (E) trilamellated hydatid cyst with surrounding adrenal gland; (H and E ×100); (F) presence of scolex and daughter cyst (H and E ×200)
Pathological Examination
Grossly, a single grey-white to grey-brown cystic soft tissue mass measuring around 9 × 6 × 4 cm3 and weighing around 150 g was received. On serial sectioning, loculated cysts filled with jelly-like vesicles were seen [Figure 1C and D]. On histopathological examination, loculated cysts showed an outer acellular laminated membrane and an inner germinal layer with attached scolices and foci of calcification along with surrounding fibrosis, hyalinisation, focal granulomatous inflammation and giant cell reaction with the peripheral compressed adrenal gland. Morphological features were consistent with an adrenal gland echinococcal (hydatid) cyst. There was no evidence of malignancy seen [Figure 1E and F].
The patient well tolerated the procedure with an uneventful post-operative course. Later on, the patient was put on Albendazole 400 mg for six weeks and was quite stable thereafter. No recurrence was noted after one year of follow-up.
Discussion
Humans have no active role in the biological cycle of Echinococcus granulosus. They are infected by ingesting contaminated food items by dog faeces which pass through hepatic filtration system and reach the lungs and other sites of the body, with adrenal gland being the rarest.[2] Most adrenal gland hydatid cysts are asymptomatic and are usually a part of disseminated disease, whilst a primary adrenal hydatid cyst is very unusual.[4] The mechanism of adrenal involvement is not fully understood till date.
Few instances of such cases have been documented in the existing literature. The hypothetical theory suggests that the Echinococcus granulosus cyst embryos disseminate through the bloodstream. These cases are typically encountered incidentally through imaging or during surgery for other abdominal conditions. The most common symptoms include vague abdominal pain, gastrointestinal issues or the detection of a palpable mass. The systemic symptoms may also arise such as hypertension from renal artery occlusion or symptoms resembling pheochromocytoma owing to adrenal medulla compression by cysts.[5] Our patient was devoid of comorbidities and presented with vague abdominal discomfort. Radiological findings of a hydatid cyst vary with disease evolution stages. Ultrasonography and CT scans with a diagnostic sensitivity ranging from 7% to 99% categorise findings into five types.[6,7]
The differential diagnosis of the adrenal cyst includes an endothelial cyst, a pseudocyst owing to infarction or haemorrhage in the adrenal gland, cystic neoplasm, cystic lymphangioma, calcified haemorrhagic cyst, extra-adrenal cystic masses and post-traumatic cyst.
Complete surgical excision is the mainstay of treatment. Although pericystectomy and resection of the entire adrenal gland are the two preferred choices of management, in our patient, complete laparoscopic adrenalectomy was conducted. Puncture, aspiration, injection and re-aspiration treatment of hydatidosis are usually avoided in the adrenal cyst because of potential complications, such as anaphylactic shock and dissemination of cyst.
In endemic areas anti-helminthic agents have been used in the treatment of systemic echinococcosis, so as to reduce the size of the cyst; however, the chances of recurrence and dissemination persist.
In our case, post-operatively the patient was put on Albendazole and showed no recurrence on one year of follow-up.
Conclusion
The hydatid cyst rarely occurs in the adrenal glands and is an uncommon pathology. It should always be suspected in the case of any cystic tumour of the adrenal gland, especially in endemic countries. The clinical features are variable and non-specific in majority of the cases. Ultrasonography and CT abdomen hold a significant sensitivity in the diagnosis of the hydatid cyst. Surgical excision is the main choice of treatment. Adjunctive medical treatment improves the outcome and decreases the recurrence rate.
Footnotes
Acknowledgements
I would like to acknowledge the entire technical staff and supporting colleagues of Department of Pathology and Department of Surgical Oncology, for helping us in carrying out this case report.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Institutional ethical approval
Ethical approval has been obtained.
Informed consent
A written informed consent was obtained from the patient before the study.
Credit author statement
P and HMA conceived the study.
P and TPS were responsible for study design.
P, HMA, TPS and GS were involved in data collection/acquisition.
P, HMA, TPS and GS were involved in revising the article for intellectual content, and approving the paper for publication; statistical analysis was not required for this study (case report).
Data availability
Authors are available and ready to supply any data about this study upon any requests through the corresponding author.
Declaration of helsinki
The study was conducted according to the ethical principles of Helsinki Declaration.
Use of artificial intelligence
No artificial intelligence has been used while writing this manuscript.