
Abstract
Background and Aims:
Postoperative sore throat (POST) is a stereotypical postoperative complication that usually occurs in approximately 21%–65% of patients who are under general anaesthesia and is ranked around eighth among the most undesirable subjective and unpleasant complaints by the society of American anaesthesiologist after general anaesthesia. As airway management is a crucial factor in the causation of POST, various methods, especially non-pharmacological, are used to reduce the incidence of postoperative sore throat with the use of a small-sized endotracheal tube with low intracuff pressures. The tracheal tube is applied with other agents that may help in reducing the symptoms such as steroids, lozenges, lignocaine, ketamine gargles, inhalation of steroids (also included in pharmacological methods used for reducing the incidence of postoperative sore throat).
Aim and Objective:
The aim of this study was to evaluate the efficacy of prophylactic low-dose nebulised dexamethasone for decreasing the incidence of post-extubation sore throat and to evaluate the complications of low-dose dexamethasone nebulisation in patients undergoing surgery under general anaesthesia.
Patients and Methods:
The study was done in the Anaesthesiology Department of Maharishi Markandeshwar Institute of Medical Sciences and Research (MMIMSR) Mullana, Ambala, after institutional ethical committee approval and written, informed consent was obtained from the patients from March 2021 to March 2022 with a group size of Group S – 25 patients and Group D – 25 patients.
Observation and Results:
The results showed that patients in the dexamethasone group had a lower POST rate compared to the control group.
Conclusion:
We concluded that a low dose of 4 mg dexamethasone was effective in reducing the incidence and severity of POST in patients after anaesthesia, and no side effects compared to 4 mg normal saline.
Introduction
Postoperative sore throat(POST) is one of the complications that occur in 21%–65% of anesthetised patients, which is recorded and enumerated by American anaesthesiologists as the eighth most bothersome subjective discomfort after anaesthesia.[1] It is usually very unpleasant for the patient and is the definite source of postoperative morbidity[2] to the patients. The components involved in postoperative sore throat are mainly the endotracheal tube (ET) size, age of the patient, gender (male or female), cuff pressure in mm of HG, total number of suctioning attempts, time taken to place the ET,[3] development of oedema or mucosal lesions due to the contact of ET with both vocal cords and posterior pharyngeal wall.[4] Many factors such as type of surgery, type of anaesthesia, and patient status result in the cause of sore throat postoperatively.
Airway management is a determinant factor in the antecedent of POST. Some of the non-pharmacological methods used to reduce the incidence of sore throat include the use of smaller-sized ET with low intracuff pressure. The tracheal tube applied with steroids, lozenges, lignocaine, ketamine gargles,[5] and inhalation of steroids [6,7] is also included in pharmacological methods used for reducing the incidence of postoperative sore throat. The purpose of this study was to determine the efficacy of preoperative low-dose nebulised dexamethasone in decreasing the incidence of postoperative sore throat in patients undergoing surgery under general anaesthesia(GA). Most data show that dexamethasone at a dose of 0.2 mg/kg can reduce the frequency of POST. Because nebulised dexamethasone also requires some local immunosuppression, we think that lower doses of nebulised dexamethasone should be more effective in reducing postoperative sore throt.
Aim and Objectives
The aim of this study was to determine the efficacy of prophylactic low-dose nebulised dexamethasone in decreasing the incidence of post-extubation sore throat and to evaluate the complications of low-dose dexamethasone nebulisation in patients undergoing surgery under general anaesthesia.
Material and Methods
The research was done in Anaesthesiology Unit of Maharishi Markandeshwar Institute of Medical Sciences and Research (MMIMSR), Mullana, Ambala. Institutional ethical committee approval and written, informed consent were obtained. Randomly selected patients were allocated by computer-generated random numbers into one of the two groups of 25 each.
Group D: Patients received 4 mg dexamethasone with 4 mL normal saline nebulisation (total volume 5 mL) through nebulisation mask, which was connected to wall-mounted oxygen.
Group S: Patients received 5 mL N.S. nebulisation (total volume 5 mL) through nebulisation mask; the oxygen was connected to the wall mounts.
Inclusion Criteria
Patients aged ranged 20–60 years planned for surgeries under GA.
Patients who give written consent for enrolment.
American Society of Anesthesiologists (ASA) physical status I and II patients.
Surgical duration <2 hours.
Exclusion Criteria
History of sore throat.
Smokers.
Obese patients.
Patients with oral and maxillofacial surgery.
Patients with nasal surgery.
ASA physical status III and IV patients.
Long duration/unknown duration of surgery.
Patients on steroids.
Pregnant women.
On arrival at the operating room, all the patients were monitored with investigations of ECG, NIBP, and SPO2. Anaesthetic protocol was made fair for all the patients. GA was induced 15 minutes after completing nebulisation with intravenous (IV) fentanyl 2 mg/kg and IV propofol 2 mg/kg. 0.5 mg/kg atracurium was eased for endotracheal intubation. Macintosh laryngoscope blade of size 3 or 4 was used for laryngoscopy.
An ET with diameter (internal) of 7 or 7.5 was used for female patients and 8 or 8.5 was used for male patients. The tracheal tube cuff was checked with inflating with the room air until no air leak was felt to confirm its working. Mechanical ventilation was calibrated to maintain ETD (end-tidal levels) of CO (carbon dioxide) between 33 and 36 mm, and anaesthesia was maintained in nitrous oxide and isoflurane with oxygen 33%. Analgesia during surgery was supplemented with PCM 1g IV. IV ondansetron 4 mg was administered half hour (30 minutes) before the end of surgery. At the end point of procedure (surgery), careful suctioning using a soft disposable suction catheter of oropharynx was done. The neuromuscular block was reversed with the use of IV glycopyrrolate 0.1 mg/ and kg neostigmine 0.5 mg/kg. After obtaining the complete consciousness, the ET was removed. The primary investigator in Post Anesthesia Care Unit (PACU), who were unaware of the group randomisations of patients assessed the sore throat at 0, 2, 8, 12 and 24 hours postoperatively, from the time of extubation in the post-anaesthetic care unit, postoperative scores were measured through a scale (0–3):
Grade 0
Throat is not sore
Grade 1
Throat is sore mildly (patient feels pain when we are assessing)
Grade 2
Throat is sore moderately (patient experiences pain when he/she swallows any liquid)
Grade 3
Throat is sore severely (patient experiences pain in throat with change in voice or hoarseness)
The main result of our study is to evaluate how effective dexamethasone nebulisation is in reducing postoperative sore throat in adults, and the secondary outcome is to examine its negativity, if any.
Sample Size Calculation
By using a previous study (reference),[7] POST incidence is 20% in dexamethasone and 56.3% in normal saline
Based on this assumption
The formula used in the situation is as follows:

where P = (P1 + P2)/2, P1 is the incidence rate in treatment, P2 is the incidence rate in treatment, {(P2–P1)} is the effect size, level of significance (usually = 5%), Zα is the value of standard α level of significance (1.96), and Zβ is the standard normal deviation for desired power (0.842). With the above assumptions, the sample size for 95% confidence level and 80% power works out to 25 in each group.
Results
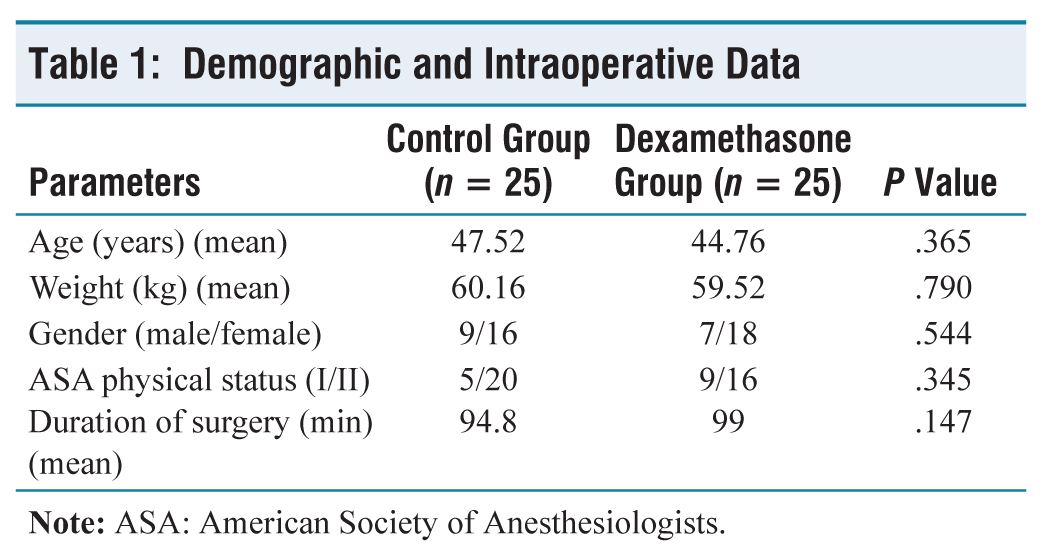
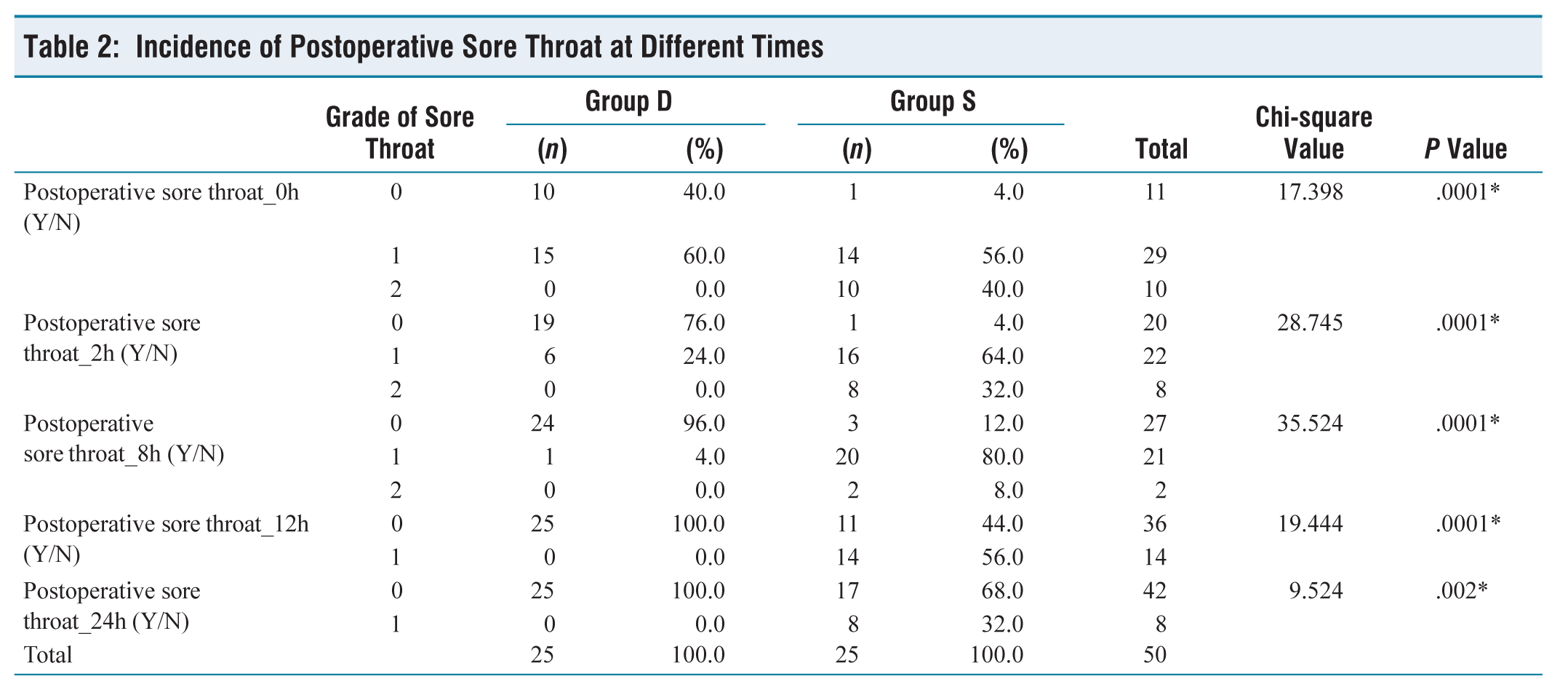
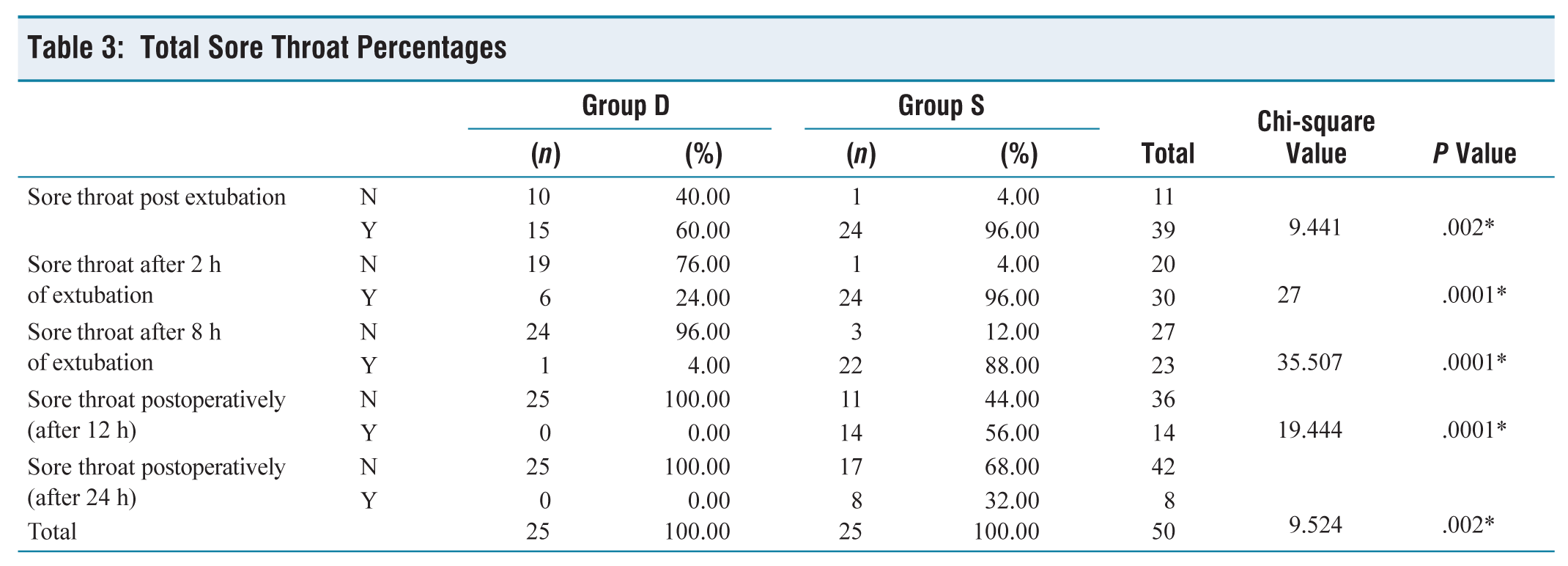
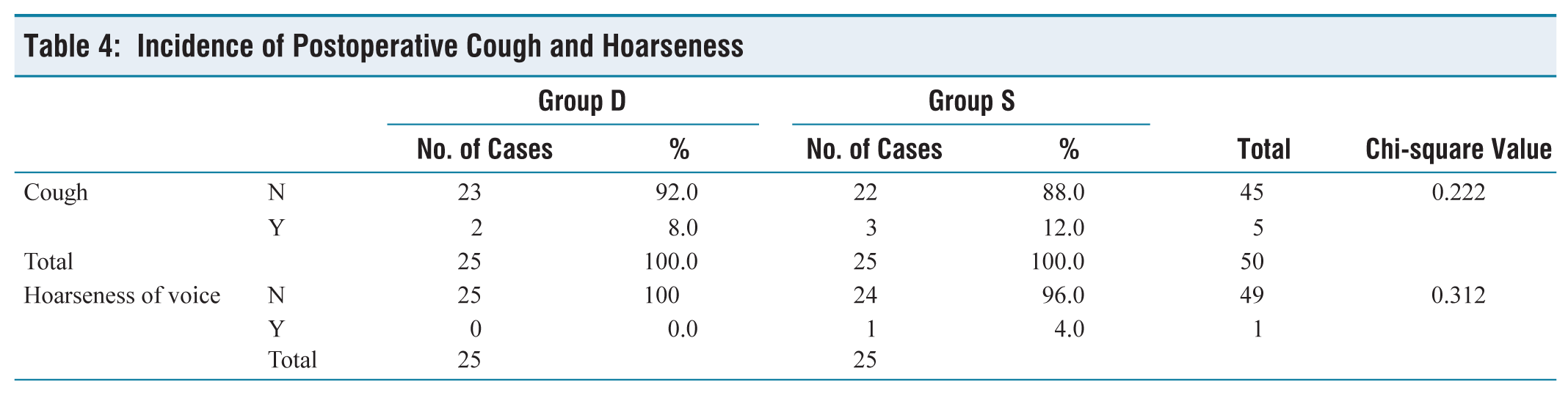
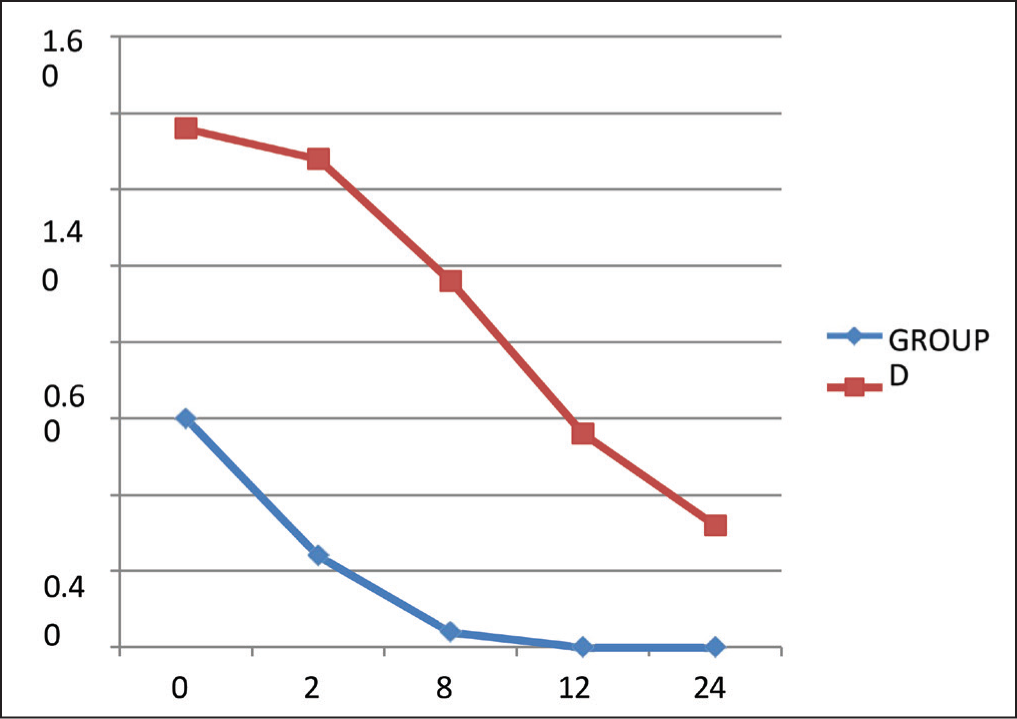
In our study, there were 25 subjects in each group as per our calculated sample size. The demographic data including age, sex, body weight, MPG grade and ASA status were found to be comparable (Table 1). The mean duration of surgery was 99.00 (minutes) in group D and it was 94.48 (minutes) in group S. Both the groups were proportionate in terms of duration of surgery and the difference between them remained statistically insignificant (P = 0.147). The overall incidence and severity of POST at 0, 2, 8, 12 and 24 hours after extubation was different in both groups, which was remarkably low in the dexamethasone group (Tables 2 and 3). After 24 hours of extubation, none of the patients in group D have shown postoperative sore throat while 8 (32%) patients in group S have shown postoperative sore throat. The incidence of postoperative sore throat was different in both groups and the difference between them was statistically significant (P = 0.002). However, the incidence of cough and hoarseness of voice was comparable in both groups (Table 4). Figure 1 shows the representation of the comparison of patients having POST at different time intervals in Groups D and S.
Demographic and Intraoperative Data
Incidence of Postoperative Sore Throat at Different Times
Total Sore Throat Percentages
Incidence of Postoperative Cough and Hoarseness
Representation of Comparison of Patients Having POST at Different Time Intervals in Group D and Group S
Discussion
POST is the most common complication that is accompanied by endotracheal intubation.[1] It occurs in both genders and can be unpleasant causing discomfort to the patient.[2] Various studies have been previously done to get rid of this complication by means of both pharmacological as well as non-pharmacological methods. In Group 1 he applied betamethasone gel to the tracheal tube and in another group, he used IV dexamethasone and found that use of betamethasone gel is more effective in reducing POST than IV dexamethasone.[3] Applying steroids, lignocaine jelly to ET, nebulisation with steroids are a few pharmacological methods while non-pharmacological methods include the use of smaller size ETs to reduce the incidence of POST.[5,6] Tabari et al. [8] conducted a study to check the efficacy of topical application of steroid in comparison with IV dexamethasone. Dexamethasone also belongs to steroids as it is a potent synthetic gluco-corticoid possessing anti-inflammatory effects. Various studies have reported the use of IV dexamethasone and have shown it to be effective in reducing POST and also in other studies preoperative nebulisation with dexamethasone 8 mg effectively decreases the incidence of sore throat. So, in this study we used a low dose of dexamethasone to evaluate its effectiveness in reducing POST. This study enrolled 50 patients aged between 20 and 60 years. Patients were randomised into two groups of 25 each; Group D – 25 patients received dexamethasone 4 mg in 4 mL saline nebulised for 10–15 minutes before endotracheal intubation. Group S – 25 patients received 5 mL saline nebulisation 10–15 minutes before intubation in patients undergoing surgery under GA. Postoperative sore throat was graded on a 4-point scale (0–3) and was recorded to be significantly lower in group D than in group S at the following time intervals. In our study the values of POST at 0, 2, 4, 8, 12 and 24 hours are given below; Immediately after extubation, the result was found to be statistically significant (P = 0.024). Two hours after extubation the result was found to be statistically significant (P = 0.004) 4 hours after extubation the result was found to be (P = 0.000) statistically significant(ss). After 8 hours of extubation the result was found to be (P = 0.000) statistically significant(ss) After 12 hours of extubation the result was found to be statistically significant (P = 0.002) After 24 hours, no significant difference was observed in the incidence of POST (P = 0.513).
In our study, the difference remained statistically insignificant between both groups with respect to patients’ characteristics, that is, age, weight, sex, Mallampati classification, ASA, duration of surgery, type of surgery. The prevalence and the severity of POST were significantly decreased in Group D as compared to Group S. Both groups show insignificant differences with respect to postoperative complications such as cough, nausea and vomiting in this study. Similar results with decreased incidence of postoperative sore throat by peri-operative nebulisation with dexamethasone have been reported. Gihan Nasr et al.[9] found the incidence of postoperative sore throat was 2, meaning that a single dose of nebulised dexamethasone effectively decreases the occurrence and severity of POST in patients following GA with endotracheal intubation. Bagchi et al.[3] found that 0.2 mg/kg dexamethasone can reduce the incidence of POST by around 30% at 1-hour post-extubation with an efficacy of around 60%. Saladi Aruna Kumari et al.[10] found that patients who were nebulised with dexamethasone had less percentage of POST as compared to patients nebulised with ketamine. Salama et al.[1] found that a single dose of nebulised dexamethasone reduced the incidence and severity of POST at 0, 2, 4, 6 and 12 hours, respectively. Park et al.[18] reported that at 1 hour after extubation there is a decrease in the incidence of POST by 22% and 42% with 0.1 mg/kg and 0.2 mg/kg dexamethasone IV with a decrease of around 30% at 24 hours after extubation with 0.2 mg/kg dexamethasone IV. Thomas et al.[11] found that after 24 hours after extubation 36.3% decrease in the overall incidence of POST with dexamethasone 8 mg IV preoperatively. Ashwini et al.[12] in their study reported an occurrence of 27.5% of POST in Group D (dexamethasone) in comparison to Group M (magnesium sulphate) in prevention of POST. The occurrence of POST in group D was 27.5% while in group M it was 57.5%. Sharma et al.[13] studied comparison of equal doses of dexamethasone in preventing POST via three different routes, that is, IV, topical, and nebulisation before surgery, and found that topical dexamethasone is as effective as IV dexamethasone in reducing POST but these techniques are not effective in decreasing hoarseness of voice while nebulisation is effective in decreasing both POST and hoarseness of voice. Regarding the incidence of postoperative sore throat, this study showed that there was a remarkable decrease in the occurrence of POST in Group D as compared to Group S. The side-effects were minimal and inconsequential among both groups in this study.
Conclusion
We conclude from our study that low-dose nebulisation with dexamethasone 4 mg pre-operatively effectively attenuates the occurrence and severity of POST in patients following GA with endotracheal intubation compared to saline 4 mg without any adverse effects.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional Ethical Committee Approval Number
Institute Ethics Committee MMIMSR – Project No IEC 2177.
CRediT Author Statement
Arbal Parvez and Ritu Gupta had Concept and design of study or acquisition of data or analysis and interpretation of data, Dr Arvinpreet Kour did drafting the article or revising it critically for important intellectual content. Dr Ajaydeep Singh did final approval of the version to be published with all modifications.
Data Availability
MMIMSR patients.
Use of Artificial Intelligence
None.