
Abstract
Background and Aims:
Meningitis in immunocompromised patients is a significant cause of mortality and morbidity. In HIV-infected cases, it is majorly of infectious origin, with Cryptococcus neoformans and Mycobacterium tuberculosis being two opportunistic pathogens together accounting for about 75% of meningitis cases. However, other variants like bacterial, aseptic, fungal or acanthamoeba meningitis can also occur in patients with HIV. The present study aimed to observe the clinical profile and aetiology of different types of meningitis in HIV-infected patients.
Methods:
A cross-sectional observational study included HIV-infected patients with symptoms and signs suggestive of meningitis. Patients were then assessed according to clinical, blood and CSF biochemical, blood and CSF microbiological and/special test parameter and/or radiological parameters. Data was statistically analysed.
Results:
Of 120 patients included, a majority belonged to the age group 26–49 years. Common presenting features included headache, fever, photophobia, neck stiffness and altered mental status. Various aetiologies of the cases included 55% cases of cryptococcal meningitis, 38.33% cases of tubercular meningitis, 3.33% cases of tubercular/cryptococcal co-infection meningitis and 1.66% cases of syphilis and pyogenic infection each. CSF findings suggested elevated opening pressure in 64.16% cases, followed by positive serum CrAg in 63.33% cases. CSF CrAg and India ink were positive, and budding yeast cell was seen in 58.33% cases.
Conclusion:
Tuberculosis and cryptococcal meningitis continue to be the prevailing culprits of meningitis in individuals with HIV. As treatment is readily available for these infections, early suspicion and prompt diagnosis coupled with effective early initiation of treatment can improve the lifespan of these patients.
Introduction
The inflammation of the meninges is the hallmark of meningitis, which is one of the most prevalent infectious disorders affecting the central nervous system (CNS) and a major cause of morbidity and death.[1] Human immunodeficiency virus (HIV) infection is a major and rising risk factor for adult meningitis.[2-5] The long-term effects of bacterial meningitis in adults include problems with hearing and vision, convulsions and deterioration of cognitive function.[6] Neurological and neuropsychological deficiencies have similarly been observed in adults who have experienced cryptococcal, tuberculous and viral meningitis.[7] The mortality rate due to meningitis appears significantly elevated in developing nations compared to developed ones.[8] This heightened mortality is influenced by factors such as delays in diagnosis and treatment as well as severe immunosuppression in people living with HIV (PLHIV).[9,10] Notably, India ranks as the third-highest country in the world in terms of the HIV epidemic. In sub-Saharan Africa and Asia, tubercular meningitis (TBM) and cryptococcal meningitis (CM) are common opportunistic CNS infections among the HIV population.[11,12] Meningitis is one of the most common CNS infections among HIV-infected individuals worldwide; though there has been a marked decline in developed countries, the scenario is different in India, and it is not uncommon to have meningitis in its initial presentation.[13] Meningitis in HIV-infected patients is almost always of infective aetiology. Cryptococcus neoformans and Mycobacterium tuberculosis are the two opportunistic pathogens together accounting for about 75% of the cases of meningitis.[14] However, other variants like bacterial, aseptic, fungal or acanthamoeba meningitis can also occur in HIV seropositive cases.
Cryptococcus neoformans infection is extremely rare in immunocompetent individuals; however, it is a major cause of illness in PLHIV, with an estimated 1 million cases of CM occurring worldwide each year resulting in 625,000 deaths.[15] CM is documented as the predominant opportunistic infection affecting the CNS in PLHIV, especially in Southeast Asia and southern and eastern Africa. In sub-Saharan Africa, it surpasses tuberculosis in terms of mortality. In developed countries, mortality rates due to HIV-associated CM range from 10% to 30%, whereas in developing nations, the rate is higher, approximately 13%–40%. This elevated mortality in developing countries is attributed to factors such as delayed presentation, restricted access to antifungal therapy and challenges in adequately monitoring intracranial pressure, among other reasons. Common clinical features of CM include acute, subacute or chronic meningitis, though a majority of patients present with headache or altered sensorium.[16]
Tuberculosis associated with HIV poses a substantial risk of mortality, contributing to approximately 25% of annual global HIV-related deaths. In India, the estimated mortality rate of TBM is 1.5 per 100,000 population, with higher complication and case fatality rates in the presence of HIV coinfection. Patients with TBM may exhibit either acute or chronic meningitis. The acute presentation closely resembles bacterial meningitis, and the duration of symptoms can range from one day to six months before presentation.[17]
Neurosyphilis is also known to complicate HIV infection. Involvement of CNS in cases of syphilis can occur at any time after initial infection. Especially, syphilitic meningitis may manifest as a primary presenting symptom within first few weeks of infection. The involvement of meninges and meningovascular systems can be suspected when there are changes in mental status, dysfunction of auditory or other cranial nerves, ocular abnormalities, signs of meningeal irritation or stroke. Bacterial meningitis is associated with the disruption of the blood–brain barrier, leading to an increased influx of the virus into the CNS, heightening the risk of AIDS dementia or a more severe progression. Existing literature indicates that inflammatory stimuli, whether from infection or vaccination, are linked to an uptick in viral replication outside the CNS.[18,19] Because immunosuppression reduces the inflammatory response, people with immunosuppression may not exhibit the characteristic symptoms of meningeal irritation.[20] Rarely, an HIV infection can result in acute bacterial meningitis. The existing data is limited and indicates that individuals living with HIV may have a slightly higher risk of invasive Neisseria meningitidis infections than the general population. Nevertheless, occurrences of meningococcal meningitis and septicaemia are still uncommon.[21] The present study aimed to observe the clinical profile and aetiology of different types of meningitis in HIV-infected patients.
Methods
A cross-sectional observational study was conducted in a tertiary care centre for four years. The Institutional Ethics Committee granted approval for the research protocol. Patients, their guardians or their relatives provided written informed consent. HIV-infected patients aged over 15 years, with signs and symptoms suggestive of meningitis regardless of their antiretroviral treatment status and who consented to be the part of the study or consented by their guardians or relatives, were included for the study. Those aged below 15 years and/or HIV-negative patients and those not consenting for participation were excluded.
Meningitis may be diagnosed if a case presents with two or more clinical features such as headache, fever, altered mental state and neck stiffness, along with the presence of CSF pleocytosis and/or identification of a specific microbiological agent in the CSF.[22] To confirm various types of meningitis, TBM can be detected by finding AFB on smears, mycobacterium growth on CSF culture, suggestive biochemical marker in CSF (including ADA), molecular biological evidence of tuberculosis (CB-NAAT) and typical neuro-radiological findings. CM can be diagnosed by detecting encapsulated yeast cells of Cryptococcus neoformans in CSF by India ink stain, positive CSF culture for C. neoformans or positive CSF cryptococcal antigen (CrAg) test. Bacterial or pyogenic meningitis can be diagnosed when pyogenic bacteria are observed on Gram stain or culture and/or increased neutrophilic count on cytology with a typical biochemistry picture of CSF.
All the selected patients were subjected to detailed clinical assessment including elicitation of history with particular emphasis relating to meningeal involvement. Venous blood was drawn for routine haematological (Hb%, TLC, DLC, PCV, platelet count), biochemical (LFT, urea, creatinine, sodium and potassium) and microbiological (blood culture) examination and/or for some special tests like serum VDRL, serum CrAg etc. The fundus was examined by an ophthalmoscope for the presence or absence of papilledema, optic atrophy etc. After that, lumbar puncture was performed by a lumbar puncture needle and the CSF opening pressure was observed and CSF was sent for cell type, cell count, sugar and protein content estimation (biochemical), Gram stain and culture, AFB stain and culture, fungal stain and culture and for some special tests such as CSF VDRL, CSF CrAg and CSF ADA estimation whenever indicated. CT/MRI scan with contrast was performed if there was any focal neurological deficit or convulsion or for evaluation of patients whenever indicated. Patients were then assessed according to clinical, blood and CSF biochemical, blood and CSF microbiological and/special tests parameter and/or radiological parameters.
Data collected was statistically analysed. Descriptive data was presented as mean, standard deviation, frequency and percentages. Measures were expressed at the 95% confidence interval. All analyses were performed using software packages—Microsoft Excel and GraphPad Prism.
Results
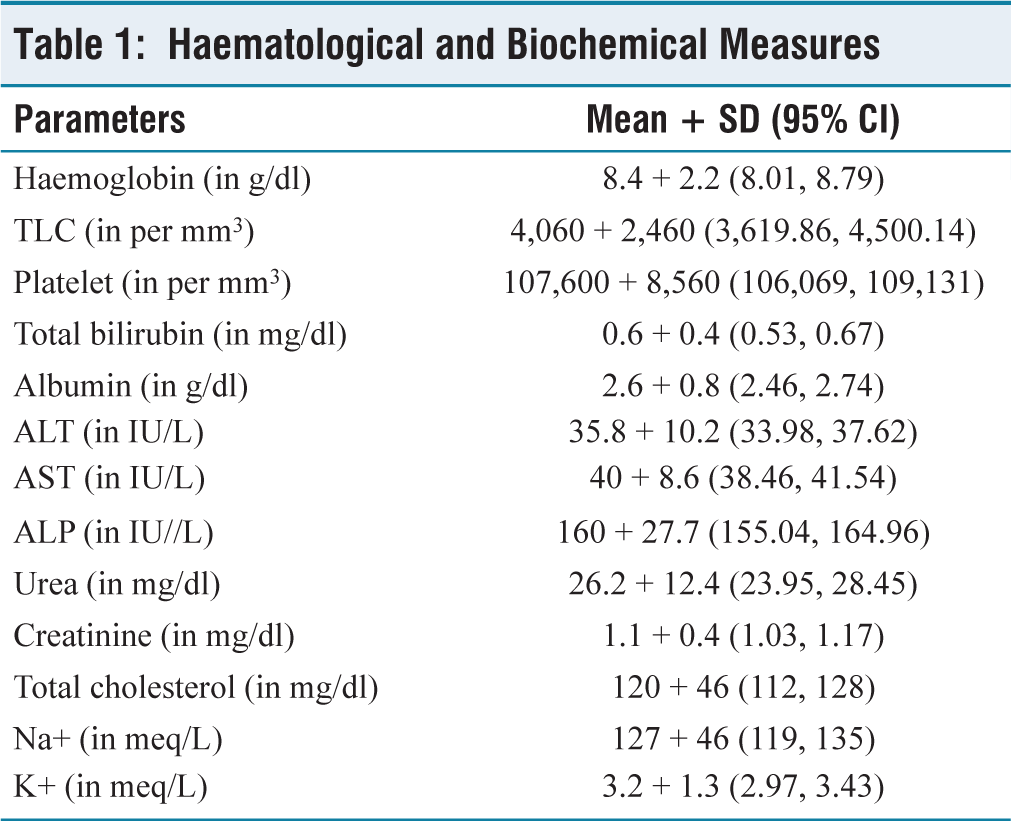
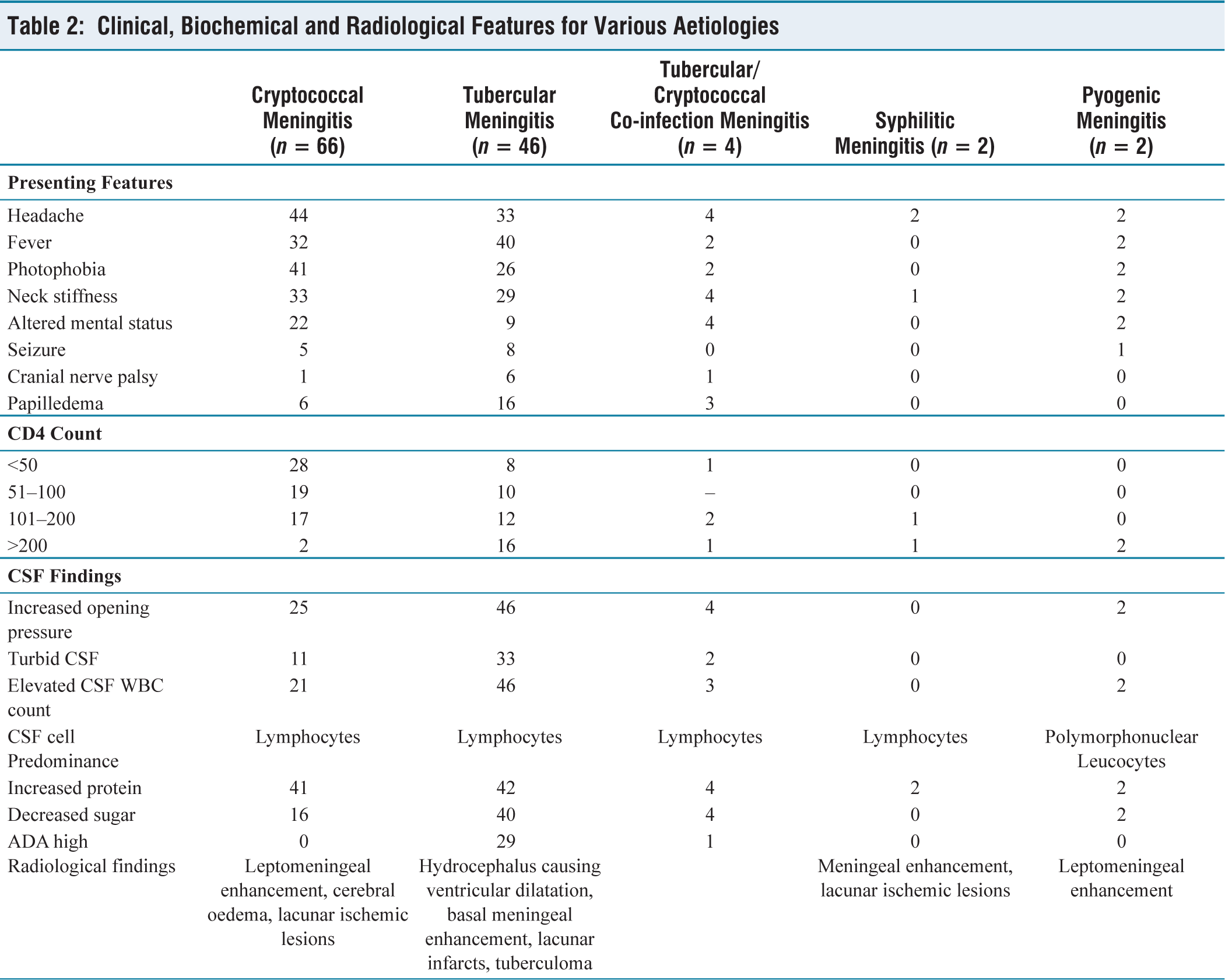
Among 120 patients, the mean age of the study population was 36.36 years (±10.08 years). A majority were males (83), and the rest were females. Thirty-three patients had unknown HIV status on admission. Ninety patients out of 120 (75%) were 26–49 years of age. Haematological and biochemical measures of the participants were noted and tabulated, as shown in Table 1. Headache was the most common presenting feature, noted in 70.83% of cases, followed by fever, photophobia and neck stiffness noted in 63.33%, 59.16% and 57.5% of cases, respectively. Altered mental status was observed in 30.83%, papilledema in 20.83%, seizure in 11.66% and cranial nerve palsy in 6.66% cases (Table 2). Abducens nerve palsy was noted in one case of cryptococcal and one case of dual infection. In the six cases of TBM where cranial nerve palsy was detected, five had abducens nerve palsy and one had oculomotor palsy. Various aetiologies of the cases included 55% cases (n = 66) of CM, 38.33% cases (n = 46) of TBM, 3.33% cases (n = 4) of tubercular/cryptococcal co-infection meningitis and 1.66% cases (n = 2) of syphilis and pyogenic infection each.
Haematological and Biochemical Measures
Clinical, Biochemical and Radiological Features for Various Aetiologies
Out of 120 patients, 37 had a CD4 count below 50 cells/mm3, 29 had a CD4 count between 51 and 100 cells/mm3, 32 were in the CD4 range of 101–200 cells/mm3 and the rest 22 patients had a CD4 count above 200 cells/mm3. Regarding the cases of CM with CD4 > 50, all were ART failure cases and on second-line ART (NRTI with INSTI—integrase inhibitors or boosted protease inhibitors). Regarding the TB meningitis cases, CD4 < 100 were ART failure cases and on second-line ART (NRTI with INSTI—integrase inhibitors or boosted protease inhibitors). Cases with CD4 > 100 were on first-line or second-line ART based on the NACO guidelines but presented with meningitis as TB may manifest at any CD4 count in HIV seropositive subjects.
CSF findings suggested elevated opening pressure in 64.16% cases (n = 77), followed by positive serum CrAg in 63.33% cases (n = 76). CSF CrAg and India ink were positive, and budding yeast cell was seen in 58.33% cases (n = 70). AFB was detected in 2.5% cases (n = 3); VDRL and Gram stain were positive in 1.6% (n = 2) and 0.83% (n = 1) cases, respectively. There were no drug-resistant cases.
Patients with TBM and CM dual infection died. Four patients with TBM with CD4 < 50 and three cases of CM with CD4 < 50 also died. Weakness of limbs, mild speech and memory disturbances were noted in 12 of the survivors at one-month follow-up. All had CD4 < 100 and were TBM cases.
Discussion
Neurological complications of HIV disease can be noticed in many outpatient cases in HIV clinics and almost half of the inpatient HIV cases. Since many cases of meningitis are caused by treatable pathogens, it is important to understand the spectrum of meningitis in India. In the present study, the incidence of meningitis was noted to be the highest in the age group 26–49 years (75%), which is similar to a study done by Sircar et al, in which the maximum incidence was 77.9% among the age group 21–40 years.[23] This was the sexually active age group, and hence, increased prevalence of HIV and meningitis was found in this age group. The male-to-female ratio in patients with meningitis was found to be 1.78:1, which is comparable to results of studies by Solu et al and Sircar et al: 2.9:1 and 3.1:1, respectively.[23,24] This is due to the fact that in India, the incidence of HIV is more in males than in females.
This study observed a correlation between CD4 count and various causes of meningitis. CM was more prevalent in individuals with lower CD4 counts, while TBM was more common in those with higher CD4 counts. In our study, the most frequent presentations included headache, fever, photophobia, neck stiffness and altered consciousness. These findings align with studies by Sircar et al and Mansuri et al, where fever was the most common symptom in 64% of individuals, followed by headache in 48%.[23,25] Our analysis indicated that CM was the leading cause of headaches, followed by TBM. In contrast, Attili et al[26] identified TBM as the most common cause of headaches. Regarding altered consciousness, CM was the primary cause in our study, followed by TBM. This differs from the findings of Mansuri et al, whose study identified TBM as the most common cause of altered consciousness.[25]
While neurological manifestations have been documented across all stages of HIV infection, they are particularly prevalent in advanced HIV disease. This underscores the urgent need for sensitive, rapid and cost-effective tests that facilitate prompt diagnosis and treatment. Swift intervention can subsequently mitigate morbidity and mortality associated with HIV-related meningitis in these contexts. The susceptibility of HIV patients to various opportunistic infections is contingent on their CD4 cell count.[27] Opportunistic infections remain the primary cause of secondary neurological manifestations linked to meningitis in HIV. As indicated by the study findings, the prevalence of HIV-associated meningitis was higher in younger adults, typically representing an economically productive age group with a pronounced male preponderance. Headache was the most common presentation upon admission, and it served as a significant predictor of neurological complications. Meningeal irritation emerged as the most frequent abnormal neurological finding, while neuroimaging revealed meningeal enhancement followed by basal exudates as the most common observations. Cerebrospinal fluid analysis and neuroimaging investigations continue to be essential for the diagnosis of opportunistic infections of the nervous system. It is important to maintain a high level of suspicion for any neurological involvement in HIV patients, regardless of the stage of the disease. This can help in an early diagnosis and timely initiation of specific therapy, thus reducing the morbidity and mortality associated with the disease.
This study has a few limitations. The resource constraints of available laboratory diagnostics, atypical presentation of few cases complicating the diagnosis of meningitis, could have led to missing few cases due to other aetiologies. Moreover, the small sample size was also a limitation. Despite all these, our study does provide some degree of evidence on the clinico-aetiological profile of meningitis cases in HIV seropositive individuals. Further research with a larger sample size is warranted for better neuropsychological evaluation and for follow-up to determine any long-term sequelae.
Conclusion
Meningitis in immunocompromised patients like those infected with HIV is an important cause of morbidity and mortality. TBM and CM remain the most common causes of meningitis in HIV cases. As treatment is readily available for these infections, early suspicion and prompt diagnosis coupled with effective early initiation of treatment can improve the lifespan of these patients.
Footnotes
Acknowledgements
The authors express their gratitude to Prof S. K. Guha, Prof D. K. Bera, Dr Dolanchampa Modak and Dr Soumendra Nath Halder for their valuable guidance and support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional Ethical Committee Approval Number
The study was approved by the Institutional Ethics Committee vide approval no CREC-STM/338.
Informed Consent
Patients, their guardians or their relatives provided written informed consent.
CRediT Author Statement
All authors contributed to the study conception, design and data collection.
Material preparation and analysis were performed by MC, AC, MB and SM.
All authors read and approved the final manuscript.
Data Availability
Data supporting the finding of this study are available within the article text and tables.
Use of Artificial Intelligence
No artificial intelligence was used for this piece of research.