
Abstract
Introduction:
Osseous metaplasia in the endometrium is a rare pathological condition characterised by the presence of mature bone, potentially leading to menorrhagia and infertility. The probable pathogenesis of this condition is metaplastic alterations in the endometrial stromal cells, leading to the formation of bony spicules. The gold standard for diagnosis of the condition remains histopathological examination, aided by radiological findings.
Methods:
This was a case report of a single case with evidence-based discussions. Informed consent was obtained.
Case report:
We present a case of a 26-year-old female with a previous lower segment caesarean section (LSCS) five years ago and an abortion, followed by dilation and curettage three years ago, presented with heavy menstrual bleeding. Trans-vaginal ultrasound revealed bright, highly echogenic and linear echo-reflective shadows in the endometrial cavity. The complete removal of bony spicules from the endometrium was done by hysteroscopy under sonographic guidance. On histology, a diagnosis of osseous metaplasia of the endometrium was given.
Conclusion:
The accuracy of the diagnosis is pivotal; it signifies a reversible factor contributing to infertility. Therefore, an accurate identification not only aids in appropriate treatment but also offers substantial relief and hope for those experiencing fertility challenges due to this condition.
Introduction
Due to its extensive morphological diversity, accurately diagnosing endometrial conditions remains among the more challenging aspects of gynaecological pathology. Endometrial osseous metaplasia is an infrequently encountered clinical condition characterised by the development of mature or immature bone within the endometrial tissue, found in approximately one out of every 10,000 cases observed during hysteroscopy.[1] Several theories have been postulated, and the prevailing hypothesis suggests a process of metaplasia in which stromal cells transform into osteoblastic cells, leading to the production of mature bone.[2] The majority of cases manifest clinically with secondary infertility following an abortion. The contraceptive-like action of the bony tissue presents attributes of secondary infertility. The spectrum ranges from reactive and degenerative lesions to those potentially linked with malignancy.[3]
Case Report
A 26-year-old female, with previous lower segment cesarean section (LSCS) five years back and abortion followed by dilation and curettage three years back, presented with heavy menstrual bleeding.
Trans-vaginal ultrasound revealed bright, highly echogenic and linear echo-reflective shadows in the endometrial cavity. Complete removal of bony spicules from the endometrium was done by hysteroscopy under sonographic guidance.
On gross examination, multiple irregular haemorrhagic tissue bits labelled endometrial curetting and osseous flakes were received in the Department of Pathology.
Microscopic examination of the Haematoxylin and Eosin-stained sections showed mature bony trabeculae with intertrabecular marrow spaces amidst the endometrial glands and stroma (Figure 1). The endometrial glands were round to tubular, present in a dense stroma with mixed chronic inflammatory infiltrates.
Photomicrograph Showing Endometrial Glands and Stroma Along with Mature Bony Trabeculae (H & E, 20×)
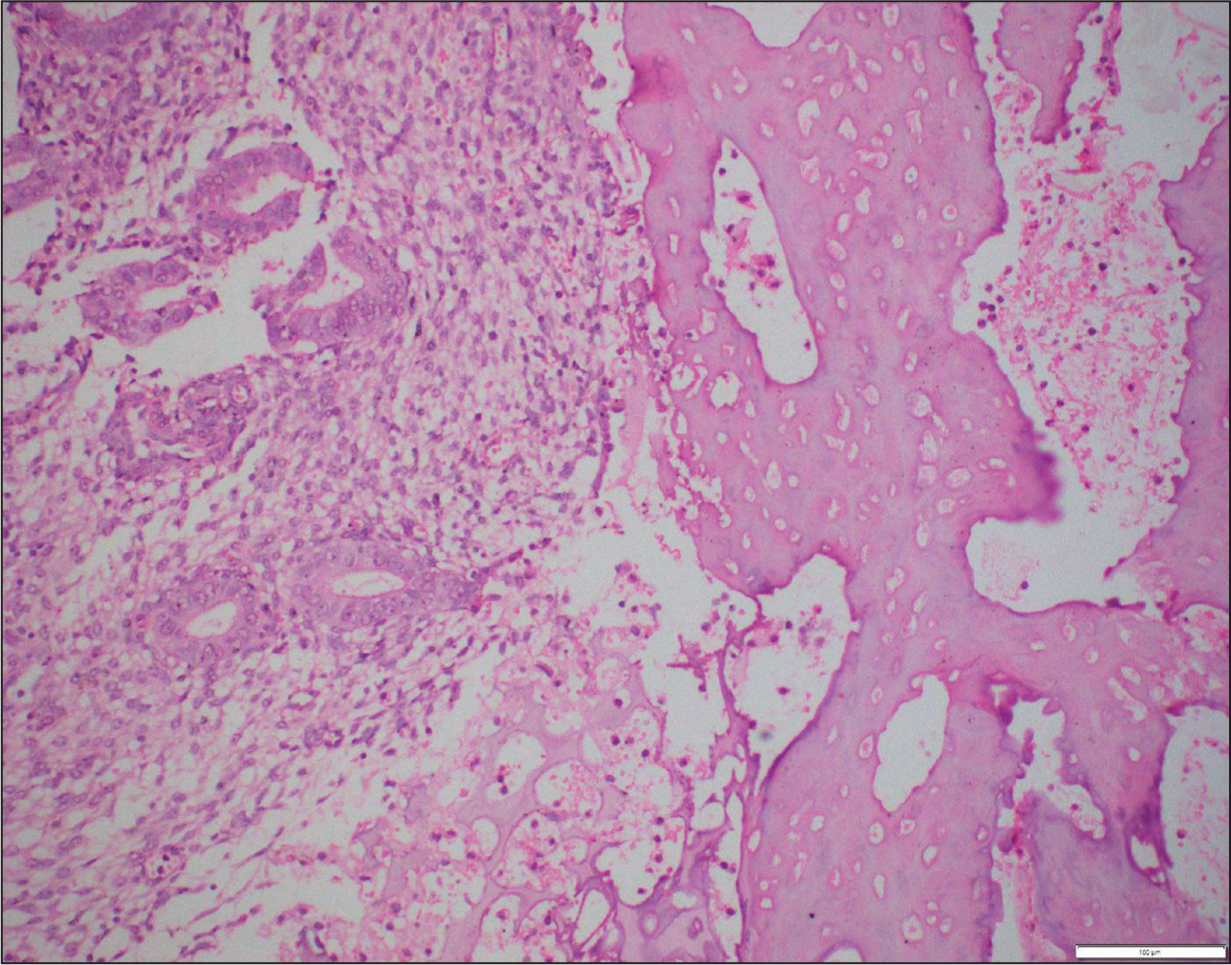
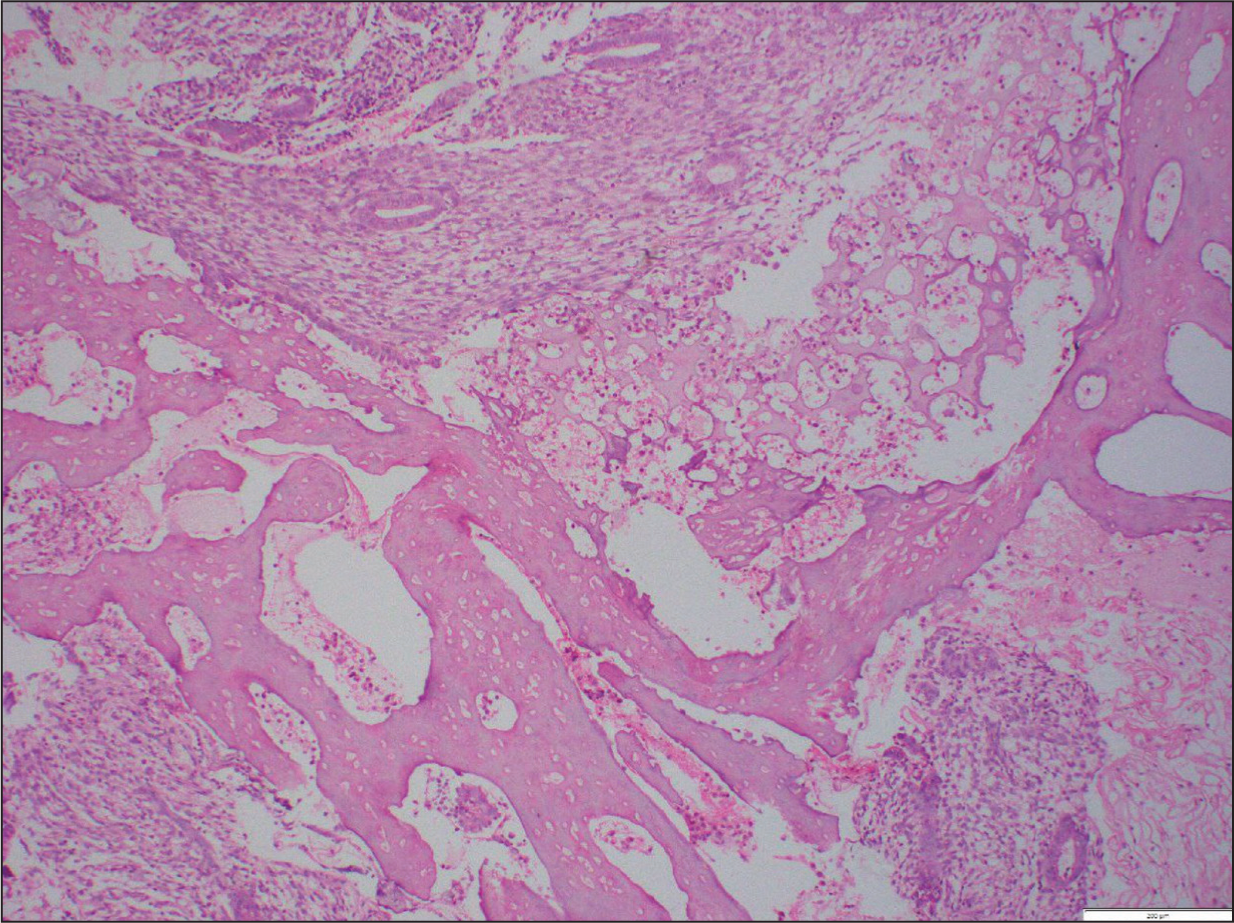
The findings were consistent with osseous metaplasia of the endometrium. The condition is proved by continuity of bony trabeculae with stromal cells (Figure 2).
There was no evidence of associated granulomatous and the patient did not have laboratory features suggestive of calcium metabolic disorder.
Photomicrograph Showing Continuity of Bony Trabeculae with Stromal Cells (H & E, 10×)
Discussion
Metaplasia is the process where one cell type undergoes a non-neoplastic transformation into another cell type within the body.[4] Endometrial metaplasia is of varying types. They involve the replacement of either epithelial or mesenchymal components with similar cells or by elements that differ from the usual tissues. Stromal metaplasia refers to the development of smooth muscle, cartilage and bone islands within the endometrial stroma.[5]
In most documented cases, osseous changes in the endometrium were preceded by a history of prior abortion.[1],[3],[6],[7] A considerable number of patients belong to the reproductive age group and have a history of first-trimester abortions, either spontaneously or due to therapeutic procedures. Studies have documented a time frame of eight weeks to 23 years between an abortion and the onset of osseous metaplasia. Although it is commonly present in women of reproductive age, there are reported cases in postmenopausal women as well.[8]
Bone found in the uterine cavity may originate from various sources. One of the theories of osseous metaplasia is the implantation of foetal tissue after an abortion. The presence of foetal cells within the endometrium could contribute to a metaplastic transformation, leading to the formation of osseous structures.[9] In cases of second-trimester miscarriages where foetal bones are retained, it can trigger ossification, leading to ongoing inflammation and tissue damage resulting in osseous metaplasia.[10]
Studies postulate that osseous metaplasia could also be a result of a dystrophic phenomenon secondary to chronic endometritis arising in the setting of abortion. Following an abortion, persistent endometritis triggers the release of superoxide radicals and tumour necrosis factor from inflammatory cells. The multipotent endometrial stromal cells in individuals with inadequate superoxide dismutase activity on prolonged exposure to these radicals and tumour necrosis factor results in the metaplasia of stromal cells into osteoblastic cells.[7]
Conclusion
Endometrial osseous metaplasia, though a rarity, possesses the potential to significantly impact fertility by creating obstacles to the usual conception process. This occurs due to the formation of intrauterine bone, stemming from metaplastic alterations in the endometrial stromal cells. Detecting and correctly identifying this condition is crucial for surgical pathologists, as misinterpretation might lead to a misdiagnosis, potentially mistaking it for a malignant mixed Müllerian tumour, which could have grave consequences.
Addressing this condition involves a procedure wherein hysteroscopic removal of the bony fragments from the endometrial cavity is performed under ultrasonographic guidance. This precise intervention holds the key to restoring fertility in affected individuals. The accuracy of the diagnosis is pivotal; it signifies a reversible factor contributing to infertility. Therefore, an accurate identification not only aids in appropriate treatment but also offers substantial relief and hope for those experiencing fertility challenges due to this condition.
Footnotes
Declaration of Conflicting Interests
The authors declare no conflict of interest with respect to the authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional Ethical Committee Approval Number
Approved: Approval Number CG/105/2023.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
CRediT Author Statement
Data Availability
No new data were created or analysed in this study. Data sharing is not applicable to this article.
Use of Artificial Intelligence
Not used.