
Abstract
Background:
Preeclampsia is a life-threatening multisystem disorder of pregnancy which has been observed in 2%–10% of pregnancies. The prevalence of Vitamin D deficiency ranges from 15% to 80%. Deficiency of Vitamin D is associated with the development of preeclampsia. This study was done to find out the prevalence of Vitamin D deficiency among preeclamptic/eclamptic and normal pregnant females, to establish Vitamin D deficiency as a causal factor of preeclampsia, and to elucidate the relation between 25 (OH) Vitamin D status and the severe preeclampsia.
Materials and Methods:
Blood samples were collected from 50 normotensives (controls) and 50 hypertensive pregnant females with preeclampsia/eclampsia (cases), and 25 (OH) Vitamin D level was measured by chemiluminescence Immunoassay.
Results:
Among the preeclamptic/eclamptic group, 32 (64%) were noted with Vitamin D deficiency and 18 (36%) with Vitamin D insufficiency. In the control group, 30 (60%) pregnant women showed Vitamin D deficiency, 19 (38%) with Vitamin D insufficiency, and a sufficient level of Vitamin D was observed in one woman (2%).
Conclusion:
Although it is difficult to demonstrate the correlation between Vitamin D levels and preeclampsia, there is a widespread global prevalence of Vitamin D deficiency during pregnancy. Hence, Vitamin D supplementation can be included routinely in the antenatal care program in India.
Introduction
Preeclampsia is a life-threatening multisystem disorder of pregnancy characterized by hypertension and proteinuria. This has been observed in 2%–10% of pregnancies. According to the WHO, it is reported to be seven times higher in developing countries (2.8% of live births) than in developed countries.[1] Various factors such as maternal internal milieu, immunological factors leading to endothelial disorder, angiogenesis factors, syncytiotrophoblastic microparticles, inflammatory mediators, and oxidative stress, play a role in the pathogenesis of preeclampsia. In addition, a poor diet with low calcium, magnesium, selenium, Vitamin A, and Vitamin C during pregnancy contributes to preeclampsia.[2] Vitamin D is one of the crucial nutritional factors for a healthy mother and child. Vitamin D deficiency is common even in tropical countries with abundant sunshine. The prevalence of Vitamin D deficiency ranges from 15% to 80%.[3] Detrimental maternal outcomes such as abortion, preeclampsia, diabetes mellitus during pregnancy, operative delivery, postpartum psychosis, osteoporosis, and infections are associated with insufficient levels of Vitamin D levels.[4,5]
Many studies have stated that despite Vitamin D supplementation for pregnant women worldwide, a frightening increase in the prevalence of Vitamin D deficiency is noted. Based on this background, this case–control study was conducted to determine the prevalence of Vitamin D deficiency among the preeclamptic/eclamptic and normal pregnant females, to establish Vitamin D deficiency as a causal factor of preeclampsia and to elucidate the relation between 25(OH) Vitamin D status and the severe preeclampsia.
Materials and Methods
This cross-sectional case-control study was conducted at the department of obstetrics and gynecology in a tertiary care hospital after obtaining ethics committee clearance (TIREC-Ref No 1145/O and G/2017) and informed consent from all participants. This study involved 50 healthy (controls) and 50 hypertensive pregnant females with preeclampsia/eclampsia (cases). Demographic details such as age, period of gestation, obstetric code, symptoms with duration, details pertaining to the selection criteria, relevant clinical and laboratory parameters, and crown-rump length by early ultrasonogram were recorded. All basic investigations were taken. Serum was collected from the study participants. 25(OH) Vitamin D concentration was measured by chemiluminescence immunoassay. 25(OH) Vitamin D level below 20 ng/mL was defined as Vitamin D deficient, levels between 21 and 29 ng/mL were diagnosed with insufficient and levels more than 30 ng/mL were considered as sufficient.[6] Statistical analysis was performed by using the statistical software (SPSS Inc, Chicago, USA). The data with P < 0.05 were interpreted as significant using the Chi-square test.
Inclusion criteria
Cases - Hypertensive pregnant females more than 20 weeks of gestation with preeclampsia/eclampsia
Controls - Normotensive pregnant females more than 20 weeks of gestational age.
Case
Preeclampsia presented with high systolic pressure > 140 mmHg or diastolic pressure > 90 mm Hg, proteinuria (>300 mg/L in 24 h urine/1 + by dipstick or more in random urine) with or without convulsions after 20 weeks of gestation in previously normal blood pressure and nonproteinuric female.
Control
Constitutes equal number of healthy normotensive pregnant women with comparable age, parity, socio-demographic position, and gestation period.
Exclusion criteria
A known case of chronic hypertension
Pregnant women with multiple gestation
Patients are already diagnosed with chronic kidney and cardiovascular diseases.
Results
The age of the study population among cases and controls were similar. Thirty-eight (76%) healthy and 42 (84%) preeclamptic/eclamptic groups belong to 21–30 years of age. No significant association (P = 0.484) between the two groups based on age. The mean age among the preeclamptic/eclamptic was 25.22 and 25.76 among the control group. Correspondingly, the mean gestation period noted among preeclamptic/eclamptic and control populations was 32.83 and 35.91 weeks.
Of the 50 cases, 34 (68%) were primigravida. A significant association between parity and preeclampsia/eclampsia was observed (P = 0.016). Of them, Vitamin D estimation was performed in the third trimester in 45 (90%) participants.
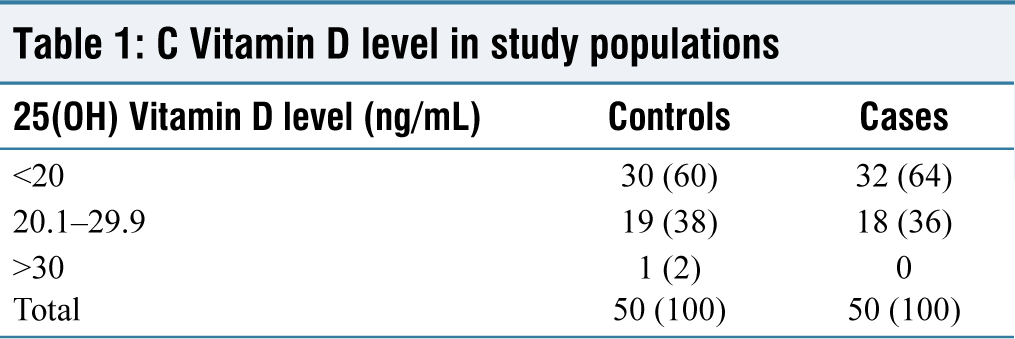
C Vitamin D level in study populations
The mean weight gain was recorded as 12.30 and 10.92 in the cases and healthy group, respectively. Weight gain noted was statistically significant in the cases (P = 0.004). Overweight/obesity was noted among seven (14%) cases and 11 (22%) controls. The mean body mass index (BMI) before pregnancy in the preeclamptic/eclamptic was 22.15 kg/m2 and controls was 22.37 kg/m2. The BMI (P = 0.471) and mean BMI before pregnancy (P = 0.789) were not statistically significant among cases and controls.
Correspondingly, in the preeclamptic/eclamptic and control groups, the mean systolic blood pressure was 162.40 and 118.20. Similarly, the mean diastolic blood pressure was recorded as 103.00 and 78.60 among the cases and controls.
The mean 25(OH) Vitamin D level was 18.55 and 18.65 among the cases and controls correspondingly. The mean Vitamin D levels between the cases and controls were not statistically significant (P = 0.669) and a null hypothesis was established.
25(OH) Vitamin D deficiency and insufficiency were noted as 32 (64%) and 18 (36%) respectively among the cases. Among the controls, 25(OH) Vitamin D deficiency and insufficiency were recorded as 30 (60%) and 19 (38%), respectively, and sufficient level was noted in 1 (2%) female. The prevalence of Vitamin D deficiency/insufficiency was almost equal among cases and controls [Table 1].
Among the preeclamptic/eclamptic group, mild preeclampsia (10), severe preeclampsia (36), and eclampsia (4) were recorded. Among the severe preeclamptic women (36), a Vitamin D level <20 ng/ml was observed in 24 females.
Discussion
Preeclampsia is akin to an escalated burden of severe obstetric complications. Very young and older women above 40 are at a greater risk of developing preeclampsia. Preeclampsia primarily affects primigravida. They are at increased risk of developing preeclampsia in subsequent pregnancy, as observed by many researchers.[7]
Vitamin D is implicated in various aspects of human life, namely bone metabolism, cell function, reproduction, implantation, and placental development. It has antiproliferative and immunomodulatory effects.[8] Vitamin D deficiency is the most common nutritional deficiency, which remains the major public health menace. Maternal 25(OH) Vitamin D started rising during the first trimester and can be two- or three-fold the prepregnancy values in the second and third trimesters.[9] Prevalence of Vitamin D deficiency/insufficiency and mean 25 (OH) Vitamin D level were similar among the cases and controls in the present study. Powe et al. also reported that there was no association between 25(OH) Vitamin D levels and preeclampsia.[10]
Regardless of high, normal, or low BMI before pregnancy, inadequate Vitamin D level was noted in the present study. Agarwal et al. recorded that obese females with >30 BMI had Vitamin D deficiency because of entrapment of Vitamin D in adipose tissue and negligible Vitamin D in the diet.[11]
Additional weight gain in a pregnant female is 12.5 kg normally. In the present study, among the cases, 12.3 kg weight gain was recorded. This is because of edema throughout the body, highly permeable vascularity, and Vitamin D deficiency. Significant weight gain was observed even among pregnant women with Vitamin D deficiency in a study by Pratumvinit et al.[12]
The mean systolic and diastolic blood pressure among the cases was 162.40 and 103.00, respectively. Correspondingly, the mean systolic and diastolic blood pressure among the control population was 118.20 and 78.6. Both systolic and diastolic blood pressures were remarkably elevated in the cases in contrast to the controls. Similar results were observed by Gogaram et al.[13] The renin–angiotensin system (RAS) is important in the regulation of blood pressure, electrolyte, and plasma volume homeostasis. Inappropriate stimulation of the RAS results in the elevation of blood pressure. Li et al. emphasized Vitamin D as a potent endocrine suppressor of renin synthesis in the regulation of RAS.[14]
In the present study, 98% of controls and 100% of cases had Vitamin D deficiency/insufficiency. The estimated prevalence of Vitamin D deficiency and insufficiency in pregnant females by Agarwal et al. was 94.5% and by Gogaram et al. was 90%.[11,13]
Poor consumption of dietary Vitamin D, environmental pollution, very little exposure to the sun, and tendency of excessive use of sunscreen attribute to inadequate Vitamin D levels. Dark-skinned people may have decreased synthesis of Vitamin D in the body.[15]
A sufficient level of Vitamin D is crucial during pregnancy, but it continues to be inconclusive to define the optimal serum 25 (OH) Vitamin D concentration among pregnant females. It depends on the range of Vitamin D among the general population.
Different assay methods such as enzyme-linked immunosorbent assay, radioimmunoassay, enzyme immunoassay, chemiluminescent immunoassay, and high-performance liquid chromatography
Among the cases, 36 had severe preeclampsia, of which 24 women were noted with Vitamin D levels <20 ng/mL. This was established by Singh et al.[1] However, a prospective case-control study by Arumaikannu et al. stated that severe Vitamin D deficiency was not associated with severity of preeclampsia.[17] However, Akkar et al., in their prospective study, observed that maternal serum paraoxonase 1 level and Neutrophil to Lymphocyte Ratio distinguish severe preeclampsia.[18]
However, a study stated that a 25(OH) Vitamin D/Triacyl glycerol ratio is preferably used in the prediction of Vitamin D status and detrimental maternal outcomes.[19]
Vitamin D requirement is increased during pregnancy. Despite that pregnant women in most countries are encouraged to consume a daily prenatal multivitamin supplement containing Vitamin D, a disturbingly high prevalence of Vitamin D deficiency has been demonstrated amongst pregnant women in most of the studies. Many researchers across the globe have begun to estimate the prevalence, its association with various feto-maternal outcomes, and effective strategies to prevent deficiency. In addition, seasonal variation is noted, with higher prevalence in winter in contrast to summer. There are disputes about the dose of Vitamin D supplements to achieve adequate Vitamin D in the body.
Limitations
The sample size was small
The prevalence of Vitamin D deficiency among the general population was not studied
Vitamin D status between pregnant and nonpregnant women was not compared
25(OH) Vitamin D levels during different seasons and different stages of pregnancy, before pregnancy, all the trimesters, were not measured
25(OH) Vitamin D estimation was done only once, and adverse maternal/fetal outcome was not recorded.
Conclusion
Although it is difficult to demonstrate the association between 25(OH) Vitamin D levels and preeclampsia, there is a high prevalence of Vitamin D deficiency during pregnancy worldwide. Consequently, its impact on detrimental feto-maternal outcomes in the present and future generations is the field of emphasis. Routine screening of 25(OH) Vitamin D levels among all pregnant females cripples huge cost; hence, cost-effective assay is required. Therefore, Vitamin D supplementation can be included routinely in the antenatal care program in India.
Footnotes
Acknowledgements
I sincerely thank Liberty Laboratory, Tirunelveli for helping in the estimation of 25 (OH) Vitamin D levels.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Institutional Ethical Committee Approval Number
TIREC-Ref No 1145/O and G/2017.
CRediT Author Statement
The author SN has substantial contributions to each of the three components mentioned below: 1. Concept and design of study or acquisition of data or analysis and interpretation of data; 2. Drafting the article or revising it critically for important intellectual content; and 3. Final approval of the version to be published.
Data Availability
Data supporting the study will be available with the author and is not published or presented anywhere else.
Use of Artificial Intelligence
Nil.